Download as pdf or txt
You might also like
- K Sembulingam Essentials of Medical Physiology 6th 105 PDFDocument11 pagesK Sembulingam Essentials of Medical Physiology 6th 105 PDFBlerta Deari100% (3)
- Michael W, COMAT SurgeryDocument14 pagesMichael W, COMAT SurgerySeanNo ratings yet
- Ploughing Through PACES Collected by DR Azmy PDFDocument385 pagesPloughing Through PACES Collected by DR Azmy PDFtejbirsingh2013No ratings yet
- Anorectal MalformationsDocument28 pagesAnorectal MalformationsVisu ReddyNo ratings yet
- Tumours of The Adrenal GlandDocument34 pagesTumours of The Adrenal GlandSonam JoshiNo ratings yet
- ABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Document26 pagesABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Malueth AnguiNo ratings yet
- Abdominal Trauma: Fatin Amirah KamaruddinDocument29 pagesAbdominal Trauma: Fatin Amirah Kamaruddinvirz23No ratings yet
- Kidney, Bladder and Prostate Pathology For Allied Health SciencesDocument38 pagesKidney, Bladder and Prostate Pathology For Allied Health SciencesMichael BrownNo ratings yet
- Defecte Abdominale NNDocument56 pagesDefecte Abdominale NNDiana CostanNo ratings yet
- Examination of Urinary SystemDocument31 pagesExamination of Urinary SystemvipinamohanofficialNo ratings yet
- Ploughing Through PACESDocument252 pagesPloughing Through PACESSmallsNo ratings yet
- Metatarsal Apophysis - Linear and Not FractureDocument14 pagesMetatarsal Apophysis - Linear and Not Fracturenithin shenoiNo ratings yet
- Approach To Abdominal Masses in ChildrenDocument36 pagesApproach To Abdominal Masses in ChildrenMia Lesaca-Medina100% (3)
- Approaches To Abdominal MassDocument49 pagesApproaches To Abdominal MassPatrick JohnNo ratings yet
- Intestinal ObstructionDocument52 pagesIntestinal ObstructionArcr BbNo ratings yet
- Acute Urinary ObstructionDocument34 pagesAcute Urinary ObstructionHafizur RashidNo ratings yet
- Intestinal Obstruction in Pediatric SurgeryDocument69 pagesIntestinal Obstruction in Pediatric Surgeryabhinay_1712No ratings yet
- Assessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesDocument45 pagesAssessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesboubiyouNo ratings yet
- Acute Abdomen: Medic Curses A MopDocument50 pagesAcute Abdomen: Medic Curses A MopSharaz AhmedNo ratings yet
- Surgical Problems in ChildrenDocument56 pagesSurgical Problems in ChildrenHugh McGregorNo ratings yet
- ACUTE ABDOMEN by DR NajamDocument65 pagesACUTE ABDOMEN by DR NajamdasdasfNo ratings yet
- Ipi 82603Document18 pagesIpi 82603Megawati LiwangNo ratings yet
- Abdominal Wall DefectsDocument14 pagesAbdominal Wall Defectsskeebs23No ratings yet
- Mass in Epigastrium-2Document37 pagesMass in Epigastrium-2brown_chocolate87643100% (1)
- Anomalies of The Upper Urinary TractDocument6 pagesAnomalies of The Upper Urinary TractMohamed Al-zichrawyNo ratings yet
- 2.4.5.2.3.a Bowel ObstructionDocument35 pages2.4.5.2.3.a Bowel ObstructionProject ByNo ratings yet
- Abdominal MassDocument5 pagesAbdominal MassArthana PutraNo ratings yet
- Neonatal Emergencies: Abdominal MassesDocument3 pagesNeonatal Emergencies: Abdominal MassesHENINo ratings yet
- Longcase Surgery ListDocument11 pagesLongcase Surgery ListDiyana ZatyNo ratings yet
- Deviriligo Notes 12Document99 pagesDeviriligo Notes 12A Fish100% (1)
- Developmental Anomalies of Gastrointestinal Tract: Dr. Dev LakheraDocument66 pagesDevelopmental Anomalies of Gastrointestinal Tract: Dr. Dev LakheraNatashaNo ratings yet
- General Surgery A Revision Session For FinalsDocument69 pagesGeneral Surgery A Revision Session For Finalsimperiallight100% (2)
- Abdominal Wall Defects: Omphalocele vs. GastroschisisDocument15 pagesAbdominal Wall Defects: Omphalocele vs. GastroschisisSerag MonierNo ratings yet
- VolvulusDocument20 pagesVolvulusParul VarshneyNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- Acute Intestinal ObstructionDocument50 pagesAcute Intestinal ObstructionDin LukbanNo ratings yet
- Imperforate Hymen Complicated by Obstructive Acute Renal FailureDocument3 pagesImperforate Hymen Complicated by Obstructive Acute Renal FailureQonny WelendriNo ratings yet
- Emergencies in GITDocument7 pagesEmergencies in GITsssajiNo ratings yet
- General Presentations:: SplenomegalyDocument4 pagesGeneral Presentations:: SplenomegalyDaniela DiazNo ratings yet
- Common Pediatric Surgery ProblemsDocument141 pagesCommon Pediatric Surgery Problemssedaka26100% (4)
- Gastrointestinal Disturbances: Abdominal Masses Include Hydronephrosis, Multicystic-Dysplastic KidneysDocument4 pagesGastrointestinal Disturbances: Abdominal Masses Include Hydronephrosis, Multicystic-Dysplastic Kidneysira guntoroNo ratings yet
- Colon 2Document56 pagesColon 2EnydLaRejNo ratings yet
- Intestinal Obstruction: Presented byDocument24 pagesIntestinal Obstruction: Presented byShirley Koeh100% (1)
- RenalDocument81 pagesRenalandreaNo ratings yet
- 1g wzxLn3krsRyRYUh3H63nEdTy1YBTsKDocument35 pages1g wzxLn3krsRyRYUh3H63nEdTy1YBTsKmedical1acc2No ratings yet
- Pathological Fracture: DR .JustinjoseDocument23 pagesPathological Fracture: DR .JustinjoseCharley CampbellNo ratings yet
- 7tumor Abdomen - DR EndangjjDocument32 pages7tumor Abdomen - DR EndangjjDhinie NovianiNo ratings yet
- 5 Congenital Malformation (Continue)Document4 pages5 Congenital Malformation (Continue)Mohamed Al-zichrawyNo ratings yet
- Scrotal Sonography Us אשכיםDocument116 pagesScrotal Sonography Us אשכיםOded YanaNo ratings yet
- Renal SystemDocument76 pagesRenal SystemDaNy ChiriacNo ratings yet
- PathologyDocument28 pagesPathologyninja-2001No ratings yet
- Intussusception 161007042729 PDFDocument44 pagesIntussusception 161007042729 PDFDina MarselinaNo ratings yet
- Large Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005Document22 pagesLarge Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005samsabesNo ratings yet
- 07 Intussusception and Midgut Volvulus - 2015-05-12 - AHC Media: Continuing Medical Education PublishingDocument10 pages07 Intussusception and Midgut Volvulus - 2015-05-12 - AHC Media: Continuing Medical Education PublishingPridina SyadirahNo ratings yet
- Askep Tumor Wilms: Ni Nyoman Udiani, S.Kep - Ns.,M.KepDocument36 pagesAskep Tumor Wilms: Ni Nyoman Udiani, S.Kep - Ns.,M.KepRelysa Magdalena IssiNo ratings yet
- Gi HyDocument2 pagesGi HyAbhineeth BhatNo ratings yet
- Disorders of The IntestinesDocument64 pagesDisorders of The IntestinesCharmaine Torio PastorNo ratings yet
- Breast DiseasesDocument35 pagesBreast Diseasesheba1997bshNo ratings yet
- Abdominal (Retroperitoneal) Cystic Lympangioma.: KeywordsDocument3 pagesAbdominal (Retroperitoneal) Cystic Lympangioma.: KeywordsIordachescu AmaliaNo ratings yet
- Evaluation of The Incontinent Woman: Yeditepe University, Medical Faculty Dept of Ob&GynDocument47 pagesEvaluation of The Incontinent Woman: Yeditepe University, Medical Faculty Dept of Ob&GynAdnan WalidNo ratings yet
- Urinary Incontinence in Women: DR Mangala DissanayakeDocument59 pagesUrinary Incontinence in Women: DR Mangala DissanayakeAdnan WalidNo ratings yet
- DR Tanvir APSB DJ StentDocument16 pagesDR Tanvir APSB DJ StentAdnan WalidNo ratings yet
- Jpurol S 20 00396 PDFDocument24 pagesJpurol S 20 00396 PDFAdnan WalidNo ratings yet
- List of Surgical Procedures Managed: AbdominalDocument3 pagesList of Surgical Procedures Managed: AbdominalAdnan WalidNo ratings yet
- Journal of Pediatric UrologyDocument24 pagesJournal of Pediatric UrologyAdnan WalidNo ratings yet
- Principles of LaparosDocument132 pagesPrinciples of LaparosAdnan WalidNo ratings yet
- Cleft Lip and Palate: Dr. Azmiry Sultana MousumiDocument33 pagesCleft Lip and Palate: Dr. Azmiry Sultana MousumiAdnan Walid100% (1)
- Overnight and Long Term Urethral Stenting After Tubularized Incised Plate (TIP) Urethroplasty For Anterior Hypospadias: A Comparative StudyDocument13 pagesOvernight and Long Term Urethral Stenting After Tubularized Incised Plate (TIP) Urethroplasty For Anterior Hypospadias: A Comparative StudyAdnan WalidNo ratings yet
- 2019 Book DiseasesOfTheChestBreastHeartA PDFDocument237 pages2019 Book DiseasesOfTheChestBreastHeartA PDFAdnan WalidNo ratings yet
- 1st ROUND: Case & InstructionsDocument7 pages1st ROUND: Case & InstructionsAdnan WalidNo ratings yet
- PIIS0022347615008574Document1 pagePIIS0022347615008574Adnan WalidNo ratings yet
- PDF BMJ 1678Document2 pagesPDF BMJ 1678Adnan WalidNo ratings yet
- Acute Urinary RetentionDocument4 pagesAcute Urinary RetentionAdnan WalidNo ratings yet
- Practical Aspects of Urinary IncontinenceDocument343 pagesPractical Aspects of Urinary IncontinenceAdnan WalidNo ratings yet
- Mr. Mahesh Chand Nursing TutorDocument7 pagesMr. Mahesh Chand Nursing TutorAdnan WalidNo ratings yet
- Primary Female Epispadias: Perineal Approach or Kelly Repair?Document7 pagesPrimary Female Epispadias: Perineal Approach or Kelly Repair?Adnan WalidNo ratings yet
- Lecture 5, GoiterDocument56 pagesLecture 5, GoiterAna-Maria TobescuNo ratings yet
- The Structure & Functioning of The Nervous SystemDocument177 pagesThe Structure & Functioning of The Nervous SystemISHITA GOEL 19224115No ratings yet
- Lecture (5) Kidney Function Tests Part IDocument33 pagesLecture (5) Kidney Function Tests Part IAmine GobranNo ratings yet
- SCI Bladder SurgeryDocument4 pagesSCI Bladder SurgeryKrish NevageNo ratings yet
- Reproductive and Endocrine System: Role of Hormones in The Male and Female Reproductive SystemDocument47 pagesReproductive and Endocrine System: Role of Hormones in The Male and Female Reproductive Systempj100% (2)
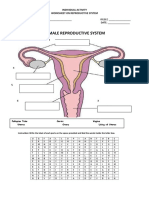
- Individual Activity Reproductive SystemDocument3 pagesIndividual Activity Reproductive Systemshiela100% (1)
- Digestive System PowerpointDocument27 pagesDigestive System Powerpointringo1101100% (1)
- Pathology of The Nervous System PDFDocument17 pagesPathology of The Nervous System PDFAnaNo ratings yet
- Organic DiseasesDocument3 pagesOrganic DiseasesGlenn Cabance LelinaNo ratings yet
- Transport CirculationDocument39 pagesTransport CirculationClara MaeNo ratings yet
- Cardiac Electrophysiology Basics (RL-204-Tn)Document5 pagesCardiac Electrophysiology Basics (RL-204-Tn)Navojit ChowdhuryNo ratings yet
- Dermatology HandbookDocument70 pagesDermatology Handbookrobchris1975100% (12)
- 3 Anatomy and Physiology (Male)Document18 pages3 Anatomy and Physiology (Male)AYO NELSONNo ratings yet
- Suprarenal GlandDocument13 pagesSuprarenal GlandAaa JjjjNo ratings yet
- Melanin Myth #7 Melanin and The Pineal GlandDocument1 pageMelanin Myth #7 Melanin and The Pineal GlandNnamdi Azikiwe100% (1)
- Grossing Templates (S)Document51 pagesGrossing Templates (S)Jack GuccioneNo ratings yet
- Lymphatic System Anatomy and Physiology - NurseslabsDocument35 pagesLymphatic System Anatomy and Physiology - NurseslabsAlyssum MarieNo ratings yet
- Biological Development in Adolescent MalesDocument2 pagesBiological Development in Adolescent MalesrobertlordNo ratings yet
- Pathology of The Respiratory SystemDocument57 pagesPathology of The Respiratory SystemAngelic khanNo ratings yet
- Reseptor AdrenergikDocument3 pagesReseptor AdrenergikAhmad Ikbal PurnawarmanNo ratings yet
- UB Human Physiology Syllabus 2012Document5 pagesUB Human Physiology Syllabus 2012Anonymous MPdGkx87bNo ratings yet
- Telinga Hidung TenggorokanDocument111 pagesTelinga Hidung Tenggorokanharyo wiryantoNo ratings yet
- Introduction Blok 17Document15 pagesIntroduction Blok 17Stephanie LyonsNo ratings yet
- Nonalcoholic Fatty Liver DiseaseDocument4 pagesNonalcoholic Fatty Liver DiseaseAshvanee sharmaNo ratings yet
- Development of TongueDocument2 pagesDevelopment of TongueCornelia GheorghitaNo ratings yet
- What Are Hormones?Document4 pagesWhat Are Hormones?Uzair SoomroNo ratings yet
- Sensory & Motor Tracts of Spinal ChordDocument38 pagesSensory & Motor Tracts of Spinal ChordtiiandiNo ratings yet
- Hemithyroidectomy Papillary Thyroid Carcinoma in Low Risk Group PatientsDocument5 pagesHemithyroidectomy Papillary Thyroid Carcinoma in Low Risk Group PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet