Download as pdf or txt
You might also like
- One Answer To Cancer by William Donald Kelley, D.D.S., M.S.Document53 pagesOne Answer To Cancer by William Donald Kelley, D.D.S., M.S.Teti Haxhidauti94% (16)
- Occupational Toxicology PDFDocument633 pagesOccupational Toxicology PDFEmilia Dunca75% (4)
- 1 s2.0 S2210261221006337 MainDocument5 pages1 s2.0 S2210261221006337 MainRubén LimaNo ratings yet
- en Papilla Vaters Tumor in Elderly An InterDocument5 pagesen Papilla Vaters Tumor in Elderly An InterAyip Bahsan AlBantaniNo ratings yet
- Synchronous Pancreatic Neuroendocrine Tumor and Pancreatic Cyst A Case ReportDocument4 pagesSynchronous Pancreatic Neuroendocrine Tumor and Pancreatic Cyst A Case ReportWorld Journal of Clinical SurgeryNo ratings yet
- AppendicitisDocument3 pagesAppendicitisRindayu Julianti NurmanNo ratings yet
- Multiple Bilateral Choroidal Metastasis From Anal MelanomaDocument2 pagesMultiple Bilateral Choroidal Metastasis From Anal MelanomaMoazzam FarooqiNo ratings yet
- Case Report - Omental TorsionDocument9 pagesCase Report - Omental TorsionProf. M AmirNo ratings yet
- JournalDocument5 pagesJournalMuhammad SyariefNo ratings yet
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinNo ratings yet
- 5 - Hung, 2004Document4 pages5 - Hung, 2004Henrique MachadoNo ratings yet
- 17-09-2019 Lower GI FINALDocument32 pages17-09-2019 Lower GI FINALNaima HabibNo ratings yet
- Endoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudyDocument6 pagesEndoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudySamuel0651No ratings yet
- Otolaryngology Head and Neck Surgery 2011 Abadie P176Document2 pagesOtolaryngology Head and Neck Surgery 2011 Abadie P176Gus JanantaraNo ratings yet
- (Final Edit) Ventral Onlay Buccal Graft For Urethrorectal FistulaDocument13 pages(Final Edit) Ventral Onlay Buccal Graft For Urethrorectal FistulaNadia Rezky ElizaNo ratings yet
- Medicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasDocument8 pagesMedicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasPatricia BezneaNo ratings yet
- General Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueDocument3 pagesGeneral Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueRahul SinghNo ratings yet
- HydronephrosisDocument3 pagesHydronephrosisCarla AlmerolNo ratings yet
- Erectile Function After Partial Penectomy For Penile CancerDocument8 pagesErectile Function After Partial Penectomy For Penile CancerTai rascunhos TaiNo ratings yet
- Inflammatory Myofibroblastic TumourDocument4 pagesInflammatory Myofibroblastic TumourThiruNo ratings yet
- Pseudotumoral Form of Schistosomiasis Mimicking Neuroendocrine TumorDocument8 pagesPseudotumoral Form of Schistosomiasis Mimicking Neuroendocrine Tumortitelascosminas6No ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- Journal of Gastroenterology and Hepatology (2013)Document1 pageJournal of Gastroenterology and Hepatology (2013)Norberto MolloNo ratings yet
- 2020-01 - Endoscopic Retrograde Cholangiopancreatography in Recurrent Acute Pancreatitis - Determining The Optimal Subgroup of Patients in Whom The Procedure Is BeneficialDocument2 pages2020-01 - Endoscopic Retrograde Cholangiopancreatography in Recurrent Acute Pancreatitis - Determining The Optimal Subgroup of Patients in Whom The Procedure Is BeneficialNawzad SulayvaniNo ratings yet
- Bulging PapillaDocument17 pagesBulging PapillailkoapNo ratings yet
- Pathophysiology, Diagnosis, and Management of Chronic Intestinal Pseudo-ObstructionDocument13 pagesPathophysiology, Diagnosis, and Management of Chronic Intestinal Pseudo-ObstructionJosealberto ArenasNo ratings yet
- Hepatobiliary and Pancreatic Disorders: Guest EditorialDocument2 pagesHepatobiliary and Pancreatic Disorders: Guest EditorialiweNo ratings yet
- Rare Small Bowel Carcinoid Tumor A Case ReportDocument5 pagesRare Small Bowel Carcinoid Tumor A Case ReportAthenaeum Scientific PublishersNo ratings yet
- A Rare Case of Colon Cancer in A Young Patient: A Case Report and Literature ReviewDocument5 pagesA Rare Case of Colon Cancer in A Young Patient: A Case Report and Literature ReviewIJAR JOURNALNo ratings yet
- ANZ J. Surg. 2008 78 (Suppl. 1) A68-A80Document13 pagesANZ J. Surg. 2008 78 (Suppl. 1) A68-A80Ammar magdyNo ratings yet
- Af13e6df 9c91 4284 A3ae Feb2bacbcba4Document7 pagesAf13e6df 9c91 4284 A3ae Feb2bacbcba4alberto cabelloNo ratings yet
- International Journal of SurgeryDocument4 pagesInternational Journal of SurgeryNatalindah Jokiem Woecandra T. D.No ratings yet
- Calcagno 2018Document10 pagesCalcagno 2018cut normaya putriNo ratings yet
- Laparoscopic Resection of Pancreatic Neuroendocrine TumorsDocument10 pagesLaparoscopic Resection of Pancreatic Neuroendocrine TumorsWahyudi Permana DarlisNo ratings yet
- Palliative Care in A Patient With Unresectable Pancreatic CancerDocument1 pagePalliative Care in A Patient With Unresectable Pancreatic CancerrenthaNo ratings yet
- Gallstone Pancreatitis - CST PDFDocument5 pagesGallstone Pancreatitis - CST PDFDaniel Rosero CadenaNo ratings yet
- Multiple Episodes of Hypoglycemia Secondary To An Insulinoma Case ReportDocument4 pagesMultiple Episodes of Hypoglycemia Secondary To An Insulinoma Case ReportmiguelNo ratings yet
- Masson Et Al-2007-Colorectal DiseaseDocument4 pagesMasson Et Al-2007-Colorectal DiseaseCamy CarmenNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportsSulaeman Andrianto SusiloNo ratings yet
- Lateral ColposuspentionDocument24 pagesLateral ColposuspentionMohammad QuayyumNo ratings yet
- Role of Diagnostic Laparoscopy in The Management of Gastro Oesophageal, Pancreatic and Colorectal CancersDocument7 pagesRole of Diagnostic Laparoscopy in The Management of Gastro Oesophageal, Pancreatic and Colorectal CancersIOSRjournalNo ratings yet
- Neuroendocrine Tumors Dr. WarsinggihDocument20 pagesNeuroendocrine Tumors Dr. WarsinggihAndi Eka Putra PerdanaNo ratings yet
- Case report-PALDocument5 pagesCase report-PALHeshan SiriwardenaNo ratings yet
- Esophageal Composite Tumor With Neuroendocrine Component: A Rare EntityDocument4 pagesEsophageal Composite Tumor With Neuroendocrine Component: A Rare EntityIJAR JOURNALNo ratings yet
- CHSJ 2012.2.5Document5 pagesCHSJ 2012.2.5Gabriel IonescuNo ratings yet
- Unexplained Ascites, A Sign For Neuroendocrine Carcinoma: Case ReportDocument3 pagesUnexplained Ascites, A Sign For Neuroendocrine Carcinoma: Case ReportsandzatNo ratings yet
- Liver Abscess ThesisDocument7 pagesLiver Abscess Thesisjenniferalexanderfortlauderdale100% (1)
- AACE Clinical Case Reports: Ebtihal Y. Alyusuf, MBBS, Aishah A. Ekhzaimy, MD, Juan A. Rivera, MDDocument5 pagesAACE Clinical Case Reports: Ebtihal Y. Alyusuf, MBBS, Aishah A. Ekhzaimy, MD, Juan A. Rivera, MDalingh98No ratings yet
- Brunner's Gland Adenoma: Case ReportDocument3 pagesBrunner's Gland Adenoma: Case ReportasclepiuspdfsNo ratings yet
- Frantz's Tumor (Solid Pseudopapillary Tumor) of The Pancreas. A Case ReportDocument3 pagesFrantz's Tumor (Solid Pseudopapillary Tumor) of The Pancreas. A Case ReportcostachemfNo ratings yet
- Wada 2015Document12 pagesWada 2015Paulina Sobarzo VegaNo ratings yet
- Liver Abscess DissertationDocument4 pagesLiver Abscess DissertationPayForAPaperAtlanta100% (1)
- Autopsy 10 4 E2020176Document7 pagesAutopsy 10 4 E2020176PriyakrishnaVasamsettiNo ratings yet
- Long Term (10 Year) Outcomes and Prognostic FactorDocument8 pagesLong Term (10 Year) Outcomes and Prognostic FactorNICOLÁS DANIEL SANCHEZ HERNANDEZNo ratings yet
- Bitcoin DiscussionDocument6 pagesBitcoin Discussionmrpoopy123No ratings yet
- Barret 2015.Document6 pagesBarret 2015.Elizabeth VegaNo ratings yet
- Amyloid Goiter Diagnosis by Ultrasound-Guided Fine NeedleDocument4 pagesAmyloid Goiter Diagnosis by Ultrasound-Guided Fine NeedlejNo ratings yet
- International Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. AwasthiDocument3 pagesInternational Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. Awasthijohanna monsalveNo ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- 1 s2.0 S1091255X23056731 MainDocument8 pages1 s2.0 S1091255X23056731 MainPaul SantiagoNo ratings yet
- Afferent Loop Decompression Technique Is Associated With A Reduction in Pancreatic Fistula Following PancreaticoduodenectomyDocument10 pagesAfferent Loop Decompression Technique Is Associated With A Reduction in Pancreatic Fistula Following PancreaticoduodenectomyDrDipesh Kumar YadavNo ratings yet
- Imaging of the Liver and Intra-hepatic Biliary Tract: Volume 2: Tumoral PathologiesFrom EverandImaging of the Liver and Intra-hepatic Biliary Tract: Volume 2: Tumoral PathologiesNo ratings yet
- Routine Tissue Processing: SectioningDocument33 pagesRoutine Tissue Processing: SectioningMarj MendezNo ratings yet
- Routine Steps (No.2) (For Soft Specimens) : DehydrationDocument68 pagesRoutine Steps (No.2) (For Soft Specimens) : DehydrationMarj MendezNo ratings yet
- Blood Donor Screening: Arce Lubang Bolima Mondoy Gocela Penero Bmls 4DDocument25 pagesBlood Donor Screening: Arce Lubang Bolima Mondoy Gocela Penero Bmls 4DMarj MendezNo ratings yet
- Routine Steps: DecalcificationDocument41 pagesRoutine Steps: DecalcificationMarj MendezNo ratings yet
- Histotech 1Document61 pagesHistotech 1Marj MendezNo ratings yet
- Methods of Tissue Examinations: Preserved / Fixed TissuesDocument38 pagesMethods of Tissue Examinations: Preserved / Fixed TissuesMarj MendezNo ratings yet
- RH Grouping: James Pretencio Kate Febrian Dabuet Rey Angelo Z. Hidalgo Victor Francis A. SalvanaDocument8 pagesRH Grouping: James Pretencio Kate Febrian Dabuet Rey Angelo Z. Hidalgo Victor Francis A. SalvanaMarj MendezNo ratings yet
- Broad Spectrum Compatibility Test: Post-Lab DiscussionDocument18 pagesBroad Spectrum Compatibility Test: Post-Lab DiscussionMarj Mendez0% (1)
- The Antiglobulin Test (Coomb's Test) Direct & Indirect: Group 1Document23 pagesThe Antiglobulin Test (Coomb's Test) Direct & Indirect: Group 1Marj Mendez100% (1)
- Abo Reverse Grouping: Becios, Cabus, Del Rosario and ManaloDocument6 pagesAbo Reverse Grouping: Becios, Cabus, Del Rosario and ManaloMarj MendezNo ratings yet
- Immunohematolog y and Blood Banking: Prerequisites - Immunology and Serology - CytogeneticsDocument6 pagesImmunohematolog y and Blood Banking: Prerequisites - Immunology and Serology - CytogeneticsMarj MendezNo ratings yet
- ABO Blood Typing: Forward Typing (Glass Slide Method)Document2 pagesABO Blood Typing: Forward Typing (Glass Slide Method)Marj MendezNo ratings yet
- 1901 - Karl Landsteiner Discovered The ABO Blood GroupDocument9 pages1901 - Karl Landsteiner Discovered The ABO Blood GroupMarj MendezNo ratings yet
- Rushing2007 PDFDocument1 pageRushing2007 PDFMarj MendezNo ratings yet
- Big Words!!: Homozygous Vs Heterozygous Dominant Vs RecessiveDocument5 pagesBig Words!!: Homozygous Vs Heterozygous Dominant Vs RecessiveMarj MendezNo ratings yet
- Bacterial Cell Morphology and ComponentsDocument59 pagesBacterial Cell Morphology and ComponentsMarj MendezNo ratings yet
- Lab Policies Beta HCG - Cobas E601 Lab 4005Document5 pagesLab Policies Beta HCG - Cobas E601 Lab 4005Marj MendezNo ratings yet
- PD 1534Document2 pagesPD 1534Marj MendezNo ratings yet
- Bacti PhsDocument12 pagesBacti PhsMarj MendezNo ratings yet
- PT & Aptt: Manish PandeyDocument42 pagesPT & Aptt: Manish PandeyMarj MendezNo ratings yet
- Republic Act No. 8504: Section 1. Title Section 2. PurposeDocument10 pagesRepublic Act No. 8504: Section 1. Title Section 2. PurposeMarj MendezNo ratings yet
- Dr. Chintan Parmar Year Resident,: - 1 - Dept. of Physiology. - Dt.:10/02/2011Document53 pagesDr. Chintan Parmar Year Resident,: - 1 - Dept. of Physiology. - Dt.:10/02/2011Marj MendezNo ratings yet
- Turn The Power Switch On': Test Procedure Test SetupDocument1 pageTurn The Power Switch On': Test Procedure Test SetupMarj MendezNo ratings yet
- I Chroma II Immune Assay AnalyzerDocument2 pagesI Chroma II Immune Assay AnalyzerMarj MendezNo ratings yet
- Inflammatory Choroidal NeovascularizationDocument7 pagesInflammatory Choroidal NeovascularizationMarj MendezNo ratings yet
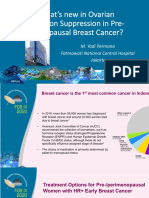
- 2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-MenopausalDocument36 pages2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-Menopausaltepat rshsNo ratings yet
- Introduction of Clinical OncologyDocument52 pagesIntroduction of Clinical OncologyThis is Pony100% (1)
- Power Foods For Daily Health and VitalityDocument38 pagesPower Foods For Daily Health and Vitalitycarpop52No ratings yet
- Dr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaDocument10 pagesDr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaOnkologi Radiasi Angkatan 23No ratings yet
- The Law of Bergonie and Triboundeau A Nice Formula For A First Approximation - Vogin and Foray (2012)Document8 pagesThe Law of Bergonie and Triboundeau A Nice Formula For A First Approximation - Vogin and Foray (2012)DanielNo ratings yet
- MCN pt3Document5 pagesMCN pt3Jerusa AbabatNo ratings yet
- LeukemiaDocument33 pagesLeukemiaChristian PasicolanNo ratings yet
- Soft Tissue SarcomaDocument34 pagesSoft Tissue SarcomanatnaelNo ratings yet
- CA A Cancer J Clinicians - January February 1982 - Unproven Methods of Cancer Management O Carl Simonton M DDocument4 pagesCA A Cancer J Clinicians - January February 1982 - Unproven Methods of Cancer Management O Carl Simonton M DabacatoteNo ratings yet
- Trifluridine and TipiracilDocument3 pagesTrifluridine and TipiracilKristine AcasioNo ratings yet
- Medicinal Plants For Cosmetics, Health and DiseasesDocument577 pagesMedicinal Plants For Cosmetics, Health and DiseasesAlou CruzNo ratings yet
- Anemia of Chronic Disease - Inflammation - UpToDateDocument36 pagesAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloNo ratings yet
- Khorana AA - Thromboembolism in Hospitalized Neutropenic Cancer PatientsDocument8 pagesKhorana AA - Thromboembolism in Hospitalized Neutropenic Cancer PatientsFarid RakhmanNo ratings yet
- Updated NCCN Guidelines For Cervical Cancer.22Document2 pagesUpdated NCCN Guidelines For Cervical Cancer.22Hari NugrohoNo ratings yet
- Celiac Lymph Node Resection and Porta Hepatis DiseaseDocument6 pagesCeliac Lymph Node Resection and Porta Hepatis DiseaseAndreeaPopescuNo ratings yet
- Hodgkin's Lymphoma: Mbimbi Joseph MBCHB Leve Iii 25 May 2011Document22 pagesHodgkin's Lymphoma: Mbimbi Joseph MBCHB Leve Iii 25 May 2011Cakama MbimbiNo ratings yet
- Varian Medical Systems JPM PresentationDocument34 pagesVarian Medical Systems JPM PresentationmedtechyNo ratings yet
- Patrick TB Ch18aDocument50 pagesPatrick TB Ch18aLily M MoNo ratings yet
- 3 CancerDocument47 pages3 Cancerkirubel getyeNo ratings yet
- Pdhpe HSC MG 2011Document14 pagesPdhpe HSC MG 2011Duncan LinNo ratings yet
- Lipoma Grey Yellow Lipoma Grey Yellow Lipoma Grey Yellow Lipoma Grey YellowDocument10 pagesLipoma Grey Yellow Lipoma Grey Yellow Lipoma Grey Yellow Lipoma Grey Yellowrashmi drNo ratings yet
- InformationFeb19 ABOUT ROHTAKDocument20 pagesInformationFeb19 ABOUT ROHTAKsushmita singhNo ratings yet
- Fix DapusDocument6 pagesFix Dapuseka saptaning windu fitriNo ratings yet
- Musawi 24Document22 pagesMusawi 24Full MarksNo ratings yet
- Hello and Welcome To Our Case Study On HRTDocument9 pagesHello and Welcome To Our Case Study On HRTDaniel Dwi NugrohoNo ratings yet
- SP BRDocument10 pagesSP BRElinor Christy BaggaoNo ratings yet
- MCQ, Cases, Neoplasia 3rd YearDocument9 pagesMCQ, Cases, Neoplasia 3rd YearTony Dawa100% (2)
- What Is NeoplasmsDocument38 pagesWhat Is NeoplasmsRashid HussainNo ratings yet