Download as pdf or txt
You might also like
- The Genius in All of UsDocument4 pagesThe Genius in All of UsVisesh50% (2)
- A Primer On Binge Eating Disorder Diagnosis and ManagementDocument11 pagesA Primer On Binge Eating Disorder Diagnosis and ManagementWalter VillalobosNo ratings yet
- Cns Spectrums: The Clinical Challenges of Akathisia CME Review ArticleDocument16 pagesCns Spectrums: The Clinical Challenges of Akathisia CME Review Articledzakiyah nurul israNo ratings yet
- A Pragmatic Approach To The Diagnosis and Treatment of Mixed Features in Adults With Mood DisordersDocument9 pagesA Pragmatic Approach To The Diagnosis and Treatment of Mixed Features in Adults With Mood DisordersWalter VillalobosNo ratings yet
- MedEdicus Insomnia CME and Test Questions PDFDocument20 pagesMedEdicus Insomnia CME and Test Questions PDFmeiutaNo ratings yet
- Pi Is 0025619617308716Document11 pagesPi Is 0025619617308716nicloverNo ratings yet
- Perilunate DislocationsDocument5 pagesPerilunate DislocationsJuanHoyosNo ratings yet
- Var WWW HTML Wp-Content Uploads 2021 02 17532 Schizophrenia-Remission-Roller-CoasterDocument8 pagesVar WWW HTML Wp-Content Uploads 2021 02 17532 Schizophrenia-Remission-Roller-CoasterArif IrpanNo ratings yet
- Pi Is 002561961500378 XDocument12 pagesPi Is 002561961500378 XTatiana IonascuNo ratings yet
- A Clinical Guide To URINE DRUG TESTING PDFDocument26 pagesA Clinical Guide To URINE DRUG TESTING PDFTavo ANo ratings yet
- Annual Fundamentals SymposiumDocument40 pagesAnnual Fundamentals SymposiumAnonymous 1AzEYdYNo ratings yet
- Medical CannabisDocument6 pagesMedical CannabisJUAN JOSE BOTIA NARANJONo ratings yet
- A Case-Based Monograph Focusing On Pediatric IBD: FacultyDocument12 pagesA Case-Based Monograph Focusing On Pediatric IBD: FacultyVijayakanth VijayakumarNo ratings yet
- Kidneystones 02012012 PDFDocument7 pagesKidneystones 02012012 PDFYudiatmaNo ratings yet
- Crista Udo 2016Document12 pagesCrista Udo 2016Allison DiêgoNo ratings yet
- Ben-Zacharia - Impact of Shared Decision MakingDocument11 pagesBen-Zacharia - Impact of Shared Decision Makingmarkludacris55No ratings yet
- 1540 1413 Article p972Document9 pages1540 1413 Article p972Lieblingsmensch andipaNo ratings yet
- Merritt-Putnam Symposium - Neurobiology of Memory in EpilepsyDocument36 pagesMerritt-Putnam Symposium - Neurobiology of Memory in EpilepsyRuda AlessiNo ratings yet
- Proton Pump Inhibitors: Review of Emerging Concerns: Concise Review For CliniciansDocument7 pagesProton Pump Inhibitors: Review of Emerging Concerns: Concise Review For CliniciansmaxNo ratings yet
- E20161212 FullDocument33 pagesE20161212 FullRicardoNo ratings yet
- Join Our Grand Rounds 1644188790Document1 pageJoin Our Grand Rounds 1644188790Elizabeth Ramos DuránNo ratings yet
- Wernicke Encephalopathydclinical PearlsDocument8 pagesWernicke Encephalopathydclinical PearlsCristian Barajas HdzNo ratings yet
- NewTreatmentsAgitationCME CITROME CNSNews2003Document6 pagesNewTreatmentsAgitationCME CITROME CNSNews2003Leslie CitromeNo ratings yet
- Epilepsy Specialist SymposiumDocument49 pagesEpilepsy Specialist SymposiumLili CRNo ratings yet
- REVISADO Y LEEREnf Celíaca. 2019. Clínica MayoDocument16 pagesREVISADO Y LEEREnf Celíaca. 2019. Clínica MayoCamilo ReyesNo ratings yet
- Optimizing Treatment Choices To Improve Adherence and Outcome Un SchizophreniaDocument11 pagesOptimizing Treatment Choices To Improve Adherence and Outcome Un SchizophreniaJosep GasconNo ratings yet
- SMITH, T. J. SAIKI, C. B. Cancer Pain Management. Symposium On Pain Medicine. Mayo Clin Proc, v. 90, P. 1428-1439, 2015.Document12 pagesSMITH, T. J. SAIKI, C. B. Cancer Pain Management. Symposium On Pain Medicine. Mayo Clin Proc, v. 90, P. 1428-1439, 2015.Fran WermannNo ratings yet
- Abx DosingDocument16 pagesAbx DosingckeshavaNo ratings yet
- PIIS0025619620303049Document9 pagesPIIS0025619620303049Matías Jesús Flamm ZamoranoNo ratings yet
- Doul 2016 HootenDocument20 pagesDoul 2016 HootenAfif SutriyadiNo ratings yet
- Chronic Pain and Mental Health Disorders: Shared Neural Mechanisms, Epidemiology, and TreatmentDocument16 pagesChronic Pain and Mental Health Disorders: Shared Neural Mechanisms, Epidemiology, and TreatmentWahyuni SetiawatiNo ratings yet
- Community Acquired Pneumonia 2Document22 pagesCommunity Acquired Pneumonia 2carosegurallNo ratings yet
- Annual Fundamentals Symposium - Epilepsy On The Consult ServiceDocument48 pagesAnnual Fundamentals Symposium - Epilepsy On The Consult ServiceRuda AlessiNo ratings yet
- Ovarian Masses and O-RADS - A Systematic Approach To Evaluating and Characterizing Adnexal Masses With MRIDocument12 pagesOvarian Masses and O-RADS - A Systematic Approach To Evaluating and Characterizing Adnexal Masses With MRIDanteAugustoVazquezGonzalezNo ratings yet
- Risk-Benefit Considerations in ADHDDocument12 pagesRisk-Benefit Considerations in ADHDJeannette DorfmanNo ratings yet
- Documento 4aDocument8 pagesDocumento 4aBelen SozaNo ratings yet
- Neuropsicologia en Cancer PediatricoDocument7 pagesNeuropsicologia en Cancer PediatricoNinaNo ratings yet
- Lumbago y Bloqueo CorticoidesDocument9 pagesLumbago y Bloqueo Corticoidesmario palma jaraNo ratings yet
- 2013 Prevention and Treatment of Elbow StiffnessDocument12 pages2013 Prevention and Treatment of Elbow StiffnessGajendra ShahNo ratings yet
- Expectations Regarding Cognitive EnhancementDocument3 pagesExpectations Regarding Cognitive EnhancementAdam RafkinNo ratings yet
- AAP - Guideline For Monitoring and Management of Pediatric Patients Before During and After Sedation For Diagnostic and Therapeutic ProceduresDocument31 pagesAAP - Guideline For Monitoring and Management of Pediatric Patients Before During and After Sedation For Diagnostic and Therapeutic Proceduresfuka priesleyNo ratings yet
- 2023 MGMT Anxiety Depression SlidesDocument33 pages2023 MGMT Anxiety Depression SlidesAnil RajaniNo ratings yet
- Pulmonary Function Tests For The Generalist: A Brief ReviewDocument9 pagesPulmonary Function Tests For The Generalist: A Brief ReviewFitria ChandraNo ratings yet
- Leche Materna 1Document15 pagesLeche Materna 1Elliot David Zelaya LaraNo ratings yet
- 118 - Week 2Document35 pages118 - Week 2Ma. Kristina Cazandra IbañezNo ratings yet
- A Protocol For The Management of Adhesive Small Bowel ObstructionDocument9 pagesA Protocol For The Management of Adhesive Small Bowel ObstructiontanyasisNo ratings yet
- PrintVersion PDFDocument28 pagesPrintVersion PDFUswaPutriemelelaNo ratings yet
- Panduan Stress Post Trumatik AustraliaDocument5 pagesPanduan Stress Post Trumatik AustraliaRizki KokoNo ratings yet
- Personalized Medicine and Psychiatry - Dream or RealityDocument6 pagesPersonalized Medicine and Psychiatry - Dream or RealityAwais QureshiNo ratings yet
- Benzodiazepine Use in Older AdultsDocument8 pagesBenzodiazepine Use in Older AdultsHendik RiawanNo ratings yet
- Articulo Farmacologia PDFDocument4 pagesArticulo Farmacologia PDFMichelle RojoNo ratings yet
- Extracorporeal Life Support Organization.1Document6 pagesExtracorporeal Life Support Organization.1Jesica DiazNo ratings yet
- CDEM 18january WebDocument24 pagesCDEM 18january WebRicardo Jonathan Ayala GarciaNo ratings yet
- 2016 Effects of Ehealth For Patients and Informal Caregivers Confronted With Cancer A Meta ReviewDocument14 pages2016 Effects of Ehealth For Patients and Informal Caregivers Confronted With Cancer A Meta ReviewDwiNo ratings yet
- A.S.P.E.N. Clinical Guidelines Nutrition Support of Children With Human Immunodeficiency Virus InfectionDocument19 pagesA.S.P.E.N. Clinical Guidelines Nutrition Support of Children With Human Immunodeficiency Virus Infectionmededep273No ratings yet
- 10 1016@j Jacc 2019 09 022Document14 pages10 1016@j Jacc 2019 09 022Kardio - Akhmad IsnaNo ratings yet
- Activity OverviewDocument44 pagesActivity OverviewSnezana MihajlovicNo ratings yet
- 10 1002@aorn 12722Document10 pages10 1002@aorn 12722Francisco NenteNo ratings yet
- Guia Sindrome Ovario PoliquisticoDocument56 pagesGuia Sindrome Ovario Poliquisticopalomazul007No ratings yet
- Piis0025619618310085 PDFDocument13 pagesPiis0025619618310085 PDFJonnathan SuarezNo ratings yet
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
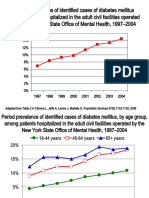
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- DiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Document8 pagesDiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Leslie CitromeNo ratings yet
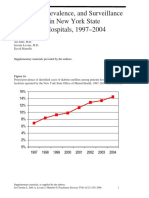
- DiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineDocument5 pagesDiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineLeslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Leslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- DivalproexDRtoERClinicalTrialAPA Poster CITROME APA2004Document1 pageDivalproexDRtoERClinicalTrialAPA Poster CITROME APA2004Leslie CitromeNo ratings yet
- UpdateBiologicalTreatmentAggression VOLAVKA ActaEspPsiquiatr2006Document13 pagesUpdateBiologicalTreatmentAggression VOLAVKA ActaEspPsiquiatr2006Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Document1 pageZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Leslie CitromeNo ratings yet
- Leslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDDocument1 pageLeslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDLeslie CitromeNo ratings yet
- MoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Document1 pageMoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Leslie CitromeNo ratings yet
- Mood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Document1 pageMood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Leslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Leslie CitromeNo ratings yet
- NewTreatmentsAgitationReview CITROME PsychQuarterly2004Document18 pagesNewTreatmentsAgitationReview CITROME PsychQuarterly2004Leslie CitromeNo ratings yet
- DosingSGAPosterWCBPHandout CITROME 2005Document4 pagesDosingSGAPosterWCBPHandout CITROME 2005Leslie CitromeNo ratings yet
- CHO-KLAT Version2.0 - Young2013Document5 pagesCHO-KLAT Version2.0 - Young2013Nay AungNo ratings yet
- The Feline Eosinophilic Granuloma ComplexDocument7 pagesThe Feline Eosinophilic Granuloma ComplexpantelisNo ratings yet
- Jishan ExamDocument4 pagesJishan ExamShawn IsaacNo ratings yet
- Insecticidal Activity of Tomato (Solanum Lycopersicum) Extract On American Cockroach (Periplenata Americana)Document7 pagesInsecticidal Activity of Tomato (Solanum Lycopersicum) Extract On American Cockroach (Periplenata Americana)heheeheheNo ratings yet
- Rhesus Iso-ImmunizationDocument20 pagesRhesus Iso-Immunizationahmed shorshNo ratings yet
- Kimera Exosomes, Kimera Labs, Inc. - 649343 - 09:01:2023 - FDADocument1 pageKimera Exosomes, Kimera Labs, Inc. - 649343 - 09:01:2023 - FDAseenfgNo ratings yet
- Ross, C. (2020) - PTSD As A Future-Oriented Survival Strategy. Richardson The Colin A. Ross Institute For Psychological TraumaDocument5 pagesRoss, C. (2020) - PTSD As A Future-Oriented Survival Strategy. Richardson The Colin A. Ross Institute For Psychological TraumaEraNo ratings yet
- Juvenile Justice Reform/Restoring Arkansas Families BillDocument12 pagesJuvenile Justice Reform/Restoring Arkansas Families BillMarine GlisovicNo ratings yet
- Hypertension in PregnancyDocument21 pagesHypertension in PregnancyIndah LatifahNo ratings yet
- Why You Should Quit Social Media 2Document6 pagesWhy You Should Quit Social Media 2api-650392913No ratings yet
- Hemoglobin Measured by Hemocue and A Reference Method in Venous and Capillary Blood: A Validation StudyDocument9 pagesHemoglobin Measured by Hemocue and A Reference Method in Venous and Capillary Blood: A Validation StudyMamad GGNo ratings yet
- Antimicrobial ResistanceDocument4 pagesAntimicrobial ResistanceDip Ayan MNo ratings yet
- Journal Pre-Proof: Biomedicine & PharmacotherapyDocument50 pagesJournal Pre-Proof: Biomedicine & Pharmacotherapysebastiangomez4No ratings yet
- Chapter 1-2 Intro To Healthy AgingDocument22 pagesChapter 1-2 Intro To Healthy AgingGladz C CadaguitNo ratings yet
- Laparoscopic Splenectomy For Pediatric Wandering Spleen - A Case ReportDocument11 pagesLaparoscopic Splenectomy For Pediatric Wandering Spleen - A Case ReportAdlyn Bea Albesa-BernaldezNo ratings yet
- 2015-06-10 - (McCrossin, James) Final REDACTED - CondensedDocument112 pages2015-06-10 - (McCrossin, James) Final REDACTED - CondensedAnonymous dHerywYZ8pNo ratings yet
- Mucolytics, Expectorants, and Mucokinetic MedicationsDocument7 pagesMucolytics, Expectorants, and Mucokinetic MedicationsDhayu Mart Hindrasyah PandiaNo ratings yet
- Anxiety, Stress & Coping: An International JournalDocument10 pagesAnxiety, Stress & Coping: An International JournalPhany Ezail UdudecNo ratings yet
- RTG CPRed Jumpstart HSGCharsDocument6 pagesRTG CPRed Jumpstart HSGCharsOrlando SaallNo ratings yet
- Chrome Galvanize - AerosolDocument1 pageChrome Galvanize - AerosolJodyNo ratings yet
- Atrial Septal DefectDocument3 pagesAtrial Septal Defectktin17No ratings yet
- HistopathologyDocument107 pagesHistopathologyKing Daniel AzurinNo ratings yet
- Mystery-Venusian Arts Handbook (Compact Edition) PDFDocument39 pagesMystery-Venusian Arts Handbook (Compact Edition) PDFjustnewaroundNo ratings yet
- Mental Health Law Abolish or Reform Kay Wilson Download PDF ChapterDocument51 pagesMental Health Law Abolish or Reform Kay Wilson Download PDF Chapterrichard.martin380100% (20)
- Novilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Eng8 Q4 Mod1Document25 pagesEng8 Q4 Mod1Janine Loresco-FernandezNo ratings yet
- Artigo Depressão Na TCCDocument21 pagesArtigo Depressão Na TCCLarissa BenderNo ratings yet
- The Political Economy of Growth-Democracy and Human CapitalDocument15 pagesThe Political Economy of Growth-Democracy and Human CapitalArchietasari NindyamurtiNo ratings yet
- BurnsDocument31 pagesBurnsLouis Carlos RoderosNo ratings yet