Download as pdf or txt
You might also like
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Distributor ObatDocument3 pagesDistributor Obatkimiafarma antang75% (4)
- Tohen 2003Document9 pagesTohen 2003Francisco VillalonNo ratings yet
- Jurnal ReadingDocument10 pagesJurnal ReadingAndreas NatanNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Clozapine Alone Versus Clozapine and Risperidone With Refractory SchizophreniaDocument11 pagesClozapine Alone Versus Clozapine and Risperidone With Refractory SchizophreniawardahNo ratings yet
- Longterm Safety and Effectiveness of Lurasidone in Schizophrenia A 22month Openlabel Extension StudyDocument10 pagesLongterm Safety and Effectiveness of Lurasidone in Schizophrenia A 22month Openlabel Extension Studyromany hosnyNo ratings yet
- Green 2009Document8 pagesGreen 2009Nadia SaiNo ratings yet
- Treatment of Delirium With Quetiapine: One Personal Copy May Be PrintedDocument3 pagesTreatment of Delirium With Quetiapine: One Personal Copy May Be PrintedMahmoud WardNo ratings yet
- Potkin2002 QTP+ Hal Risp Thiridazine RCTDocument10 pagesPotkin2002 QTP+ Hal Risp Thiridazine RCTIulia CiocotisanNo ratings yet
- Rituximab in Hephrotic SyndromeDocument8 pagesRituximab in Hephrotic Syndromejennylau0809No ratings yet
- Childhood Idiopathic Nephrotic Syndrome in Turkey: Original ArticleDocument4 pagesChildhood Idiopathic Nephrotic Syndrome in Turkey: Original ArticleDrago BakovicNo ratings yet
- Clozapin RisperidonDocument7 pagesClozapin RisperidonAnonymous 2LcGdsRNo ratings yet
- Alpha-Dihydroergocryptine vs. Pramipexole As Adjunct Symptomatic Treatment of Idiopathic Parkinson'sDocument9 pagesAlpha-Dihydroergocryptine vs. Pramipexole As Adjunct Symptomatic Treatment of Idiopathic Parkinson'sRizka Leonita FahmyNo ratings yet
- Journal Presentation Dr. Jasmine RSSSDocument48 pagesJournal Presentation Dr. Jasmine RSSSAhuja SaurabhNo ratings yet
- Britishjournalofpsychiatry BRITISHJOURNALOFPSYCHIATRY (2001), 179,514 518 (2 0 0 1), 1 7 9, 5 1 4 5 1 8Document6 pagesBritishjournalofpsychiatry BRITISHJOURNALOFPSYCHIATRY (2001), 179,514 518 (2 0 0 1), 1 7 9, 5 1 4 5 1 8Imam FirdausNo ratings yet
- Valproic Acid and Risperidone: A Drug Interaction?: To The EditorDocument2 pagesValproic Acid and Risperidone: A Drug Interaction?: To The EditorFariz RifqiNo ratings yet
- Valproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Document7 pagesValproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Juan ParedesNo ratings yet
- A Randomized, Double-Blind, Placebo-Controlled Study of Citalopram in Adolescents With Major Depressive Disorder - Von Knorring 2006Document5 pagesA Randomized, Double-Blind, Placebo-Controlled Study of Citalopram in Adolescents With Major Depressive Disorder - Von Knorring 2006Julio JuarezNo ratings yet
- J Schres 2004 01 014Document17 pagesJ Schres 2004 01 014xhdrv7nvdrNo ratings yet
- 1 s2.0 S2772408522006408 MainDocument2 pages1 s2.0 S2772408522006408 MainloloasbNo ratings yet
- Ajp 156 5 702Document8 pagesAjp 156 5 7029 PsychologyNo ratings yet
- TX Nmda EncefDocument9 pagesTX Nmda EncefserftyNo ratings yet
- Alzheimer PicoDocument6 pagesAlzheimer PicoRaja Friska YulandaNo ratings yet
- Apathy in Currently Nondepressed Patients Treated With A SSRI For A Major Depressive Episode - Outcomes Following RandomDocument8 pagesApathy in Currently Nondepressed Patients Treated With A SSRI For A Major Depressive Episode - Outcomes Following RandomMooyongNo ratings yet
- Aac 37 2 178Document5 pagesAac 37 2 178Marcelo salvador silva MacotoraNo ratings yet
- Safety and Effectiveness of Lurasidone in Adolescents With Schizophrenia: Results of A 2-Year, Open-Label Extension StudyDocument11 pagesSafety and Effectiveness of Lurasidone in Adolescents With Schizophrenia: Results of A 2-Year, Open-Label Extension StudyNaiana PaulaNo ratings yet
- Dexmedetomidine Is Effective For Sedation For Outpatient ElectroencephalographyDocument6 pagesDexmedetomidine Is Effective For Sedation For Outpatient ElectroencephalographyRudi HerdiansyahNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- The Efficacy of Propofol and Midazolam in Treatment of Refractory Status Epilepticus in ChildrenDocument6 pagesThe Efficacy of Propofol and Midazolam in Treatment of Refractory Status Epilepticus in ChildrenReci MaulitaNo ratings yet
- Ajp.161.10.1837 2Document11 pagesAjp.161.10.1837 2HKANo ratings yet
- Use of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaDocument4 pagesUse of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaPutu Agus GrantikaNo ratings yet
- Coping Therapy Dependence: Naltrexone and Skills For AlcoholDocument7 pagesCoping Therapy Dependence: Naltrexone and Skills For AlcoholOana BumbucNo ratings yet
- Lurasidone in Older Adults With Bipolar DepressionDocument8 pagesLurasidone in Older Adults With Bipolar DepressionSarah El HalabiNo ratings yet
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- Update On Therapeutics: Shehan Williams and Thilini RajapakseDocument3 pagesUpdate On Therapeutics: Shehan Williams and Thilini RajapakseAnjula KumarasingheNo ratings yet
- ZiprasidoneHaloperidolAgitationlPostHocAbstractICOSR CITROME SchizBull2005Document2 pagesZiprasidoneHaloperidolAgitationlPostHocAbstractICOSR CITROME SchizBull2005Leslie CitromeNo ratings yet
- Propofol Kelly 1999Document11 pagesPropofol Kelly 1999dai leNo ratings yet
- Deberdt 2008Document8 pagesDeberdt 2008Lidia BorleanNo ratings yet
- A Comparison of Risperidone and Haloperidol For The Prevention of Relapse in Patients With SchizophreniaDocument8 pagesA Comparison of Risperidone and Haloperidol For The Prevention of Relapse in Patients With SchizophreniaIlham WahyuNo ratings yet
- LurasidoneDocument1 pageLurasidoneRaju Teach KapsNo ratings yet
- IJP Volume 4 Issue 1 Pages 1233-1242Document10 pagesIJP Volume 4 Issue 1 Pages 1233-1242Anca AdamNo ratings yet
- HEAD NeurologieDocument13 pagesHEAD NeurologieMihaela MavrodinNo ratings yet
- Rathore SS. Digoxin in Treatment of Heart FailureDocument8 pagesRathore SS. Digoxin in Treatment of Heart FailureDinhLinhNo ratings yet
- Espironolactona en DiálisisDocument11 pagesEspironolactona en DiálisisMaria Juliana ValenzuelaNo ratings yet
- Weinblad 2001Document1 pageWeinblad 2001remiNo ratings yet
- Daytime Sleepiness Associated With LurasidoneDocument9 pagesDaytime Sleepiness Associated With Lurasidoneromany hosnyNo ratings yet
- Donepezil in Vascular Dementia: A Randomized, Placebo-Controlled StudyDocument9 pagesDonepezil in Vascular Dementia: A Randomized, Placebo-Controlled StudyDian ArdiansyahNo ratings yet
- Aripiprazole Monotherapy in Acute Mania: 12-Week Randomised Placebo-And Haloperidol - Controlled StudyDocument12 pagesAripiprazole Monotherapy in Acute Mania: 12-Week Randomised Placebo-And Haloperidol - Controlled StudySherly VeronicaNo ratings yet
- Modafinil and Armodafinil in Schizophrenia: Chittaranjan Andrade, MDDocument3 pagesModafinil and Armodafinil in Schizophrenia: Chittaranjan Andrade, MDbenedicte lewinNo ratings yet
- Riociguat - ReviewDocument4 pagesRiociguat - Reviewapi-302147754No ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- Singh. NMP Better Result VS DYDDocument2 pagesSingh. NMP Better Result VS DYDRuth RachmawatyNo ratings yet
- Wei Zheng, 2018Document8 pagesWei Zheng, 2018Hananya ManroeNo ratings yet
- Wilcock 2008Document11 pagesWilcock 2008Nadia SaiNo ratings yet
- Ann Pharmacother 2011 Owenby 95 100Document6 pagesAnn Pharmacother 2011 Owenby 95 100Mahmud AnshoriNo ratings yet
- Hyper Na CorrectionDocument11 pagesHyper Na CorrectionalizanNo ratings yet
- Research Paper: NeuropsychiatryDocument11 pagesResearch Paper: NeuropsychiatryveerrajuNo ratings yet
- Clinical Cardiology - May 1992 - Massie - 24 Hour Efficacy of Once Daily Diltiazem in Essential HypertensionDocument4 pagesClinical Cardiology - May 1992 - Massie - 24 Hour Efficacy of Once Daily Diltiazem in Essential Hypertensionarkarchitecture2023No ratings yet
- 5 PharmacologyDocument4 pages5 Pharmacologyshiv_prhNo ratings yet
- Treatment–Refractory Schizophrenia: A Clinical ConundrumFrom EverandTreatment–Refractory Schizophrenia: A Clinical ConundrumPeter F. BuckleyNo ratings yet
- ZolpidemProductLabel 0819 PDFDocument7 pagesZolpidemProductLabel 0819 PDFLeslie CitromeNo ratings yet
- Restoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsDocument14 pagesRestoril™ (Temazepam) Capsules USP RX Only Warning: Risks From Concomitant Use With OpioidsLeslie CitromeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument14 pagesSee Full Prescribing Information For Complete Boxed WarningLeslie CitromeNo ratings yet
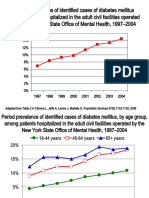
- DiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Document8 pagesDiabetesEpidemiologySlidesForDistribution CITROME AdaptedPsychServ2006Leslie CitromeNo ratings yet
- WhatIsTranscranialMagneticStimulation CITROME KlineLine1999Document1 pageWhatIsTranscranialMagneticStimulation CITROME KlineLine1999Leslie CitromeNo ratings yet
- CATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Document2 pagesCATIENNTEditorialRegardingCITROME KERWIN IntJClinPract2006Leslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME CINP2006Leslie CitromeNo ratings yet
- UpdateBiologicalTreatmentAggression VOLAVKA ActaEspPsiquiatr2006Document13 pagesUpdateBiologicalTreatmentAggression VOLAVKA ActaEspPsiquiatr2006Leslie CitromeNo ratings yet
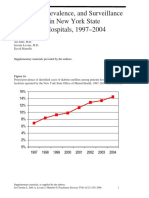
- DiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineDocument5 pagesDiabetesEpidemiologyFiguresSupplement CITROME PsychServ2006onlineLeslie CitromeNo ratings yet
- ZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Document1 pageZiprasidoneHaloperidolHostilitySchizophreniaPoster CITROME APA2006Leslie CitromeNo ratings yet
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Document5 pagesOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeNo ratings yet
- OlanzapineHighDoseRCTHGLFPoster KINON CINP2006Document19 pagesOlanzapineHighDoseRCTHGLFPoster KINON CINP2006Leslie CitromeNo ratings yet
- IncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Document1 pageIncidencePrevalenceSurveillanceDiabetesMellitusInpatientsPoster CITROME NCDEU2006Leslie CitromeNo ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- Benefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderDocument1 pageBenefits of A Second Dose of Intramuscular (IM) Aripiprazole To Control Agitation in Patients With Schizophrenia or Bipolar I DisorderLeslie CitromeNo ratings yet
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- ZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Document1 pageZiprasidoneHaloperidolAgitationlPostHocPoster CITROME ACNP2004Leslie CitromeNo ratings yet
- MedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Document2 pagesMedicalTrainingUnitedStatesAddendum CITROME CMAJ1992Leslie CitromeNo ratings yet
- Leslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDDocument1 pageLeslie Citrome, MD, MPH, Richard Josiassen, PHD, Nigel Bark, MD, Karen S Brown, MS, Suresh Mallikaarjun, PHD, Daniel E Salazar, PHDLeslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlACNPPoster CITROME ACNP2003Leslie CitromeNo ratings yet
- MoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Document1 pageMoodStabilizerUtilizationAbbottAPAPoster CITROME 2004Leslie CitromeNo ratings yet
- AtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Document1 pageAtypicalAntipsychoticsDiabetesMellitusCaseControlAPAPoster CITROME APA2004Leslie CitromeNo ratings yet
- DosingSGAPosterWCBPHandout CITROME 2005Document4 pagesDosingSGAPosterWCBPHandout CITROME 2005Leslie CitromeNo ratings yet
- NewTreatmentsAgitationReview CITROME PsychQuarterly2004Document18 pagesNewTreatmentsAgitationReview CITROME PsychQuarterly2004Leslie CitromeNo ratings yet
- Mood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Document1 pageMood Stabilizer and Antipsychotic Medication Coprescribing (Polypharmacy)Leslie CitromeNo ratings yet
- Annex 1 - Health Facilities For The Police and PrisonsDocument4 pagesAnnex 1 - Health Facilities For The Police and PrisonsZuhura NassorNo ratings yet
- Activity 12: Parts of A Drug Guide: Generic NameDocument8 pagesActivity 12: Parts of A Drug Guide: Generic NameJerry LicayanNo ratings yet
- Regulatory AffairsDocument8 pagesRegulatory Affairsnsk79in@gmail.com100% (1)
- CostPlusDrugs - Price ListDocument66 pagesCostPlusDrugs - Price ListCBS 11 NewsNo ratings yet
- BiopharmaceuticsDocument21 pagesBiopharmaceuticsStefano PorzioNo ratings yet
- IP121lec - Topic 3 - Calculation of Doses PDFDocument47 pagesIP121lec - Topic 3 - Calculation of Doses PDFBj LarracasNo ratings yet
- Nada Lincomycyn and Espectynomycin Solubleucm061812Document4 pagesNada Lincomycyn and Espectynomycin Solubleucm061812laurz95No ratings yet
- A Simple Practice Guide For Dose Conversion Between Human and AnimalsDocument5 pagesA Simple Practice Guide For Dose Conversion Between Human and AnimalsKishor BajgainNo ratings yet
- 9 - DR Arun Bhatt - Schedule YDocument27 pages9 - DR Arun Bhatt - Schedule Yvivek100% (1)
- Drugs ActDocument44 pagesDrugs ActBhavithavNo ratings yet
- Unit 13-English for Medicine and Pharmacy 2: *Bắt buộcDocument8 pagesUnit 13-English for Medicine and Pharmacy 2: *Bắt buộcNguyễn Thành LongNo ratings yet
- Drug ResearchDocument33 pagesDrug ResearchJakobus Benny SalimNo ratings yet
- E PrescribingDocument2 pagesE PrescribingDakota SimbsNo ratings yet
- CONOL - BETA BLOCKERS (Selective and Non Selective)Document22 pagesCONOL - BETA BLOCKERS (Selective and Non Selective)Jewelyn ConolNo ratings yet
- Grade 6 Answer KeyDocument8 pagesGrade 6 Answer KeyAngelica BuquiranNo ratings yet
- HJM 25 Okt 2023Document16 pagesHJM 25 Okt 2023Mel WsNo ratings yet
- Study Guide-Pharmacology-PrelimDocument20 pagesStudy Guide-Pharmacology-Prelimcath payotNo ratings yet
- Buffer Stock RJDocument9 pagesBuffer Stock RJardinaNo ratings yet
- Pharmacy CareDocument9 pagesPharmacy CareJoslin RozNo ratings yet
- Medicine Prescriptions JavaDocument6 pagesMedicine Prescriptions Javaapi-636650239No ratings yet
- Pharmaceuticals Executive Summary PDFDocument10 pagesPharmaceuticals Executive Summary PDFPaes C. MarceloNo ratings yet
- Inactive Ingredient Search For Approved Dhtghrug ProductsDocument2 pagesInactive Ingredient Search For Approved Dhtghrug ProductsDang Chi CongNo ratings yet
- Ijpab 2015 3 1 224 235 PDFDocument12 pagesIjpab 2015 3 1 224 235 PDFDrAmit VermaNo ratings yet
- Pharmacology Daily Practice PaperDocument7 pagesPharmacology Daily Practice PaperSunil Kumar MahapatraNo ratings yet
- Julfar Ksa - Google SearchDocument1 pageJulfar Ksa - Google Searchptq9cpxpf9No ratings yet
- Annex A1 - KonSulTa Meds PDFDocument4 pagesAnnex A1 - KonSulTa Meds PDFEric Monte de RamosNo ratings yet
- Covid Resource Bhopal v1.0.KTDocument14 pagesCovid Resource Bhopal v1.0.KTKapil TilwaniNo ratings yet
- Polypharmacy: Gina Desevo Bellotti and Emily R. HajjarDocument8 pagesPolypharmacy: Gina Desevo Bellotti and Emily R. Hajjarwidodo adi prasetyoNo ratings yet
- Laiman'S Pharmacy: Pre-Test ExaminationDocument3 pagesLaiman'S Pharmacy: Pre-Test ExaminationChristine PaulineNo ratings yet