Download as pdf or txt
You might also like
- Behavioral System ModelDocument38 pagesBehavioral System Modelmalyn1218100% (15)
- The Education of Nurses On The Leading Edge of TransformationDocument31 pagesThe Education of Nurses On The Leading Edge of TransformationDip Ayan M100% (2)
- The Helping Art of Clinical Nursing by Ernestine WeidenbachDocument16 pagesThe Helping Art of Clinical Nursing by Ernestine Weidenbachhasan rashid100% (1)
- Levine's Four Conservation Principles PDFDocument6 pagesLevine's Four Conservation Principles PDFTINJU123456100% (1)
- Trends and Issues in Nursing PracticeDocument2 pagesTrends and Issues in Nursing PracticeVanesa Guillano100% (1)
- Evidence Based Practice in ObstetricsDocument17 pagesEvidence Based Practice in ObstetricsAnn Merlin JobinNo ratings yet
- Faye Glenn Abdellah's Nursing TheoryDocument11 pagesFaye Glenn Abdellah's Nursing TheoryAnna Vanezza Dee100% (1)
- Chapter 4. Determinants of LearningDocument36 pagesChapter 4. Determinants of LearningAlyssa Marie SociasNo ratings yet
- List of Nursing Theories and TheoristsDocument4 pagesList of Nursing Theories and Theoristscecedrake100% (2)
- ICN Code of Ethics For NursesDocument4 pagesICN Code of Ethics For NursesSj Eclipse100% (1)
- Jean WatsonDocument14 pagesJean WatsonJoanne Garcia Feliciano100% (5)
- ALUMNI BERBAGI - Dr. Andreas Wahyu Wicaksono - PPDS OrthopaediDocument30 pagesALUMNI BERBAGI - Dr. Andreas Wahyu Wicaksono - PPDS OrthopaediUmiNo ratings yet
- Assignment 1. Learning TheoriesDocument5 pagesAssignment 1. Learning Theoriesmpumientombela2305No ratings yet
- Introduction in Nursing Research: Prepared By, Mrs Arjita Associate ProfesorDocument22 pagesIntroduction in Nursing Research: Prepared By, Mrs Arjita Associate Profesorsivaspb5No ratings yet
- Health Care TeamDocument20 pagesHealth Care TeamSumit YadavNo ratings yet
- Classification - of - Nursing - TheoriesDocument20 pagesClassification - of - Nursing - Theoriesako at ang exoNo ratings yet
- Rogers TheoryDocument50 pagesRogers TheoryREVATHI H KNo ratings yet
- Lumbar Puncture ReportDocument5 pagesLumbar Puncture ReportTweenie DalumpinesNo ratings yet
- Faye Glenn AbdellahDocument12 pagesFaye Glenn AbdellahAnnapurna Dangeti100% (1)
- Developing A Teaching PlanDocument6 pagesDeveloping A Teaching PlanAntonette Africa MercadoNo ratings yet
- Autonomy and AccountabilityDocument9 pagesAutonomy and AccountabilityaparnaNo ratings yet
- Bio Physiological MethodsDocument4 pagesBio Physiological MethodsDelphy VargheseNo ratings yet
- Family Health Nursing: Ms - Neethu Vincent Asst Professor KVM College of NursingDocument9 pagesFamily Health Nursing: Ms - Neethu Vincent Asst Professor KVM College of NursingNeethu VincentNo ratings yet
- Theories in CHNDocument38 pagesTheories in CHNSujatha J Jayabal80% (5)
- Ethical Issues in Nursing ResearchDocument34 pagesEthical Issues in Nursing Researchvishnu100% (1)
- The Problems and Adjustments Encountered by The NursingDocument32 pagesThe Problems and Adjustments Encountered by The Nursingjezzabellganda100% (3)
- On Handerson TheoryDocument26 pagesOn Handerson Theoryvikas tak100% (1)
- Assessing Learning Needs of Nursing Staff Jesson PlantasDocument4 pagesAssessing Learning Needs of Nursing Staff Jesson PlantasMarjorie PacatanNo ratings yet
- Apgar ScoreDocument22 pagesApgar ScoreBharat ThapaNo ratings yet
- NIGHTINGALEDocument7 pagesNIGHTINGALEvikas tak100% (1)
- Roles & Functions of Community Health NurseDocument9 pagesRoles & Functions of Community Health NurseJan Jewey33% (3)
- Myra LevineDocument13 pagesMyra LevineLarra Suzainne Vanguardia FanegaNo ratings yet
- Community Health Nursing Bag Technique PDFDocument2 pagesCommunity Health Nursing Bag Technique PDFRachael50% (2)
- Rogers Theory AnpDocument12 pagesRogers Theory AnpJoshNo ratings yet
- Standards 2Document11 pagesStandards 2Krishnaveni MurugeshNo ratings yet
- ScalesDocument41 pagesScalesBelbi Mol100% (1)
- Health Educ1Document6 pagesHealth Educ1Märsh Pascual-DapunNo ratings yet
- Abdellah TheoryDocument12 pagesAbdellah TheorygopscharanNo ratings yet
- Nursing ProcessDocument45 pagesNursing ProcessSukmaErfiana100% (1)
- Rubin's TheoryDocument3 pagesRubin's TheoryBeerna Grande50% (2)
- Knowledge Regarding Skin Banking Among Student NursesDocument5 pagesKnowledge Regarding Skin Banking Among Student NursesAnonymous izrFWiQNo ratings yet
- The Home VisitDocument7 pagesThe Home VisitMayur Patel0% (1)
- Theory of Goal AttainmentDocument18 pagesTheory of Goal AttainmentCarla ParongNo ratings yet
- Concept of Self-HealthDocument14 pagesConcept of Self-HealthAastha Ramawat100% (2)
- Lesson 1 Intro To BiochemDocument15 pagesLesson 1 Intro To BiochemJulius Memeg PanayoNo ratings yet
- Jean Watson's Theory of Care & Its Application in Nursing PracticeDocument2 pagesJean Watson's Theory of Care & Its Application in Nursing PracticeJan Oneille Y. Valles100% (1)
- Health AssessmentDocument115 pagesHealth Assessmentteuuuu100% (1)
- Assignment On Historcal Evolution of Research in NursingDocument35 pagesAssignment On Historcal Evolution of Research in NursingPoonam Dhatwalia100% (1)
- Journal Reading (SICU)Document12 pagesJournal Reading (SICU)Kian HerreraNo ratings yet
- A. Nursing Process in The Care of Population, Groups, and CommunityDocument6 pagesA. Nursing Process in The Care of Population, Groups, and Communityanne marie50% (2)
- Introduction To Nursing ResearchDocument17 pagesIntroduction To Nursing ResearchYounas BhattiNo ratings yet
- Clinical TeachingDocument48 pagesClinical TeachingAmy Roc100% (3)
- Assignment On Concept of Nursing EducationDocument6 pagesAssignment On Concept of Nursing Educationmaya verma100% (1)
- Peplau's Nursing Theory (Theory of Interpersonal Relation)Document11 pagesPeplau's Nursing Theory (Theory of Interpersonal Relation)Gayatri Mudliyar100% (1)
- A Study To Assess The Effectiveness of Planned Teaching Module Regarding Oral Health Care Among 10-14 Years Old Children in Chakore Primary SchoolDocument4 pagesA Study To Assess The Effectiveness of Planned Teaching Module Regarding Oral Health Care Among 10-14 Years Old Children in Chakore Primary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- File1-Role of Nurse in EpidemiologyDocument14 pagesFile1-Role of Nurse in EpidemiologyRufus Raj83% (23)
- Life Process & Seminar On Growth & DevelopmentDocument48 pagesLife Process & Seminar On Growth & Developmenttinsjohn100% (9)
- PROBLEM SOLVING APPROCH M.SC Nursing 2nd YearDocument4 pagesPROBLEM SOLVING APPROCH M.SC Nursing 2nd Yearkavita100% (1)
- Jean Watson'S Transpersonal Care TheoryDocument14 pagesJean Watson'S Transpersonal Care Theorymay catahan100% (2)
- Jean Watson'S Philosophy and Theory of Human Caring: Dr. Is A Theorist Who DevelopedDocument6 pagesJean Watson'S Philosophy and Theory of Human Caring: Dr. Is A Theorist Who DevelopedSimmy DhaliwalNo ratings yet
- Jean Watson's Human Caring Science, A Theory of NursingDocument30 pagesJean Watson's Human Caring Science, A Theory of NursingLiza Carillo0% (1)
- Jean WatsonDocument27 pagesJean Watsonapi-248689867No ratings yet
- General Referral GuidelinesDocument6 pagesGeneral Referral GuidelinesJan Oneille Y. VallesNo ratings yet
- School Form 1 (SF 1 - YakalDocument4 pagesSchool Form 1 (SF 1 - YakalJan Oneille Y. VallesNo ratings yet
- Activity Design SBFP TrainingDocument3 pagesActivity Design SBFP TrainingJan Oneille Y. VallesNo ratings yet
- Clinical Referral FormDocument2 pagesClinical Referral FormJan Oneille Y. VallesNo ratings yet
- Referral PolicyDocument5 pagesReferral PolicyJan Oneille Y. Valles100% (2)
- School Form 1 (SF 1 - KamagongDocument6 pagesSchool Form 1 (SF 1 - KamagongJan Oneille Y. VallesNo ratings yet
- 1 Universal Health Care v1Document39 pages1 Universal Health Care v1Jan Oneille Y. Valles100% (1)
- Activity Design in BSFP 2021Document6 pagesActivity Design in BSFP 2021Jan Oneille Y. VallesNo ratings yet
- School Form 1 (SF 1 - MolaveDocument4 pagesSchool Form 1 (SF 1 - MolaveJan Oneille Y. VallesNo ratings yet
- School Form 1 (SF 1) - MahoganyDocument4 pagesSchool Form 1 (SF 1) - MahoganyJan Oneille Y. VallesNo ratings yet
- School Form 1 (SF 1 - LawaanDocument6 pagesSchool Form 1 (SF 1 - LawaanJan Oneille Y. VallesNo ratings yet
- Jean Watson's Theory of Care & Its Application in Nursing PracticeDocument2 pagesJean Watson's Theory of Care & Its Application in Nursing PracticeJan Oneille Y. Valles100% (1)
- Siow NorraDocument9 pagesSiow NorraJan Oneille Y. VallesNo ratings yet
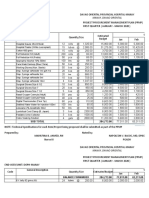
- PPMP Medical Supplies 2020Document16 pagesPPMP Medical Supplies 2020Jan Oneille Y. VallesNo ratings yet
- Jean Watson: Dr. Transpersonal Caring" or "Caring Science" and Founder of Watson Caring ScienceDocument21 pagesJean Watson: Dr. Transpersonal Caring" or "Caring Science" and Founder of Watson Caring ScienceJan Oneille Y. VallesNo ratings yet
- Nursing Theory An Application of Watson's Theory of Caring ModelDocument6 pagesNursing Theory An Application of Watson's Theory of Caring ModelJan Oneille Y. VallesNo ratings yet
- Nightingale Env Theory Mga AbstractsDocument10 pagesNightingale Env Theory Mga AbstractsJan Oneille Y. VallesNo ratings yet
- Good Air and Bad Air: The Importance of Ventilation: Posted On byDocument5 pagesGood Air and Bad Air: The Importance of Ventilation: Posted On byJan Oneille Y. VallesNo ratings yet
- Perspective of Postpartum Depression TheoriesDocument9 pagesPerspective of Postpartum Depression TheoriesJan Oneille Y. VallesNo ratings yet
- Postpartum Depression TheoryDocument9 pagesPostpartum Depression TheoryJan Oneille Y. Valles100% (1)
- Kolcaba CompleteDocument9 pagesKolcaba CompleteJan Oneille Y. VallesNo ratings yet
- Work Experience SheetDocument1 pageWork Experience SheetJan Oneille Y. VallesNo ratings yet
- Grammar Translation Was The Offspring of German ScholarshipDocument4 pagesGrammar Translation Was The Offspring of German ScholarshipRam ChannelNo ratings yet
- Sinan Wang-ResumeDocument3 pagesSinan Wang-Resumeapi-186000749No ratings yet
- The Importance of Research in Daily LifeDocument1 pageThe Importance of Research in Daily LifeGeralyn NabaysaNo ratings yet
- (Paper) Silent ReadingDocument13 pages(Paper) Silent ReadingSahmiral Amri Rajagukguk100% (1)
- Revised Comm TheoryDocument7 pagesRevised Comm TheoryJona Mae CamachoNo ratings yet
- Dramatisation Method of TeachingDocument14 pagesDramatisation Method of TeachingRingle Job100% (4)
- Est RSDocument6 pagesEst RSJanine CallanganNo ratings yet
- C o T - 1st-QuarterDocument2 pagesC o T - 1st-QuarterJeric Espinosa CabugNo ratings yet
- BIFM Level 3 Qualifications SpecificationDocument73 pagesBIFM Level 3 Qualifications SpecificationRaaf Rifandi0% (1)
- Intelligence TestDocument38 pagesIntelligence TestDr. Tapan Kr. DuttaNo ratings yet
- Learning How To LearnDocument33 pagesLearning How To Learnantony garcesNo ratings yet
- IMRaD Sample 2Document13 pagesIMRaD Sample 2JIGO LOCANANo ratings yet
- Round Up The SheepDocument7 pagesRound Up The SheepYuhuan ZhaoNo ratings yet
- Unit 3 - Learning TheoriesDocument40 pagesUnit 3 - Learning TheoriesJuvelyn Balbosa TaladuaNo ratings yet
- Lesson Plan VII - First Time at A Festival!Document6 pagesLesson Plan VII - First Time at A Festival!ema100% (1)
- Career Portfolio Presentation RubricDocument2 pagesCareer Portfolio Presentation Rubricapi-261468231No ratings yet
- FREN 141 Out Line ATELIERDocument2 pagesFREN 141 Out Line ATELIERxvNo ratings yet
- Sunil ResumeDocument2 pagesSunil ResumeVineet LakhmaniNo ratings yet
- Monir Manir CV PsDocument3 pagesMonir Manir CV PsSurzo Chandra DasNo ratings yet
- Eloisa May A. Masibag RPMS 2023Document56 pagesEloisa May A. Masibag RPMS 2023Eloisa MaibagNo ratings yet
- Final Answer Key Developmet of Values EducationDocument8 pagesFinal Answer Key Developmet of Values EducationDaenielle Angela GranzonNo ratings yet
- Google Classroom Project Lesson PlanDocument7 pagesGoogle Classroom Project Lesson Planapi-563599311No ratings yet
- Thesis-Dissertation Defense Evaluation 2013CDocument4 pagesThesis-Dissertation Defense Evaluation 2013CWilson GayoNo ratings yet
- SFES Action Plan in English 2017-2018Document2 pagesSFES Action Plan in English 2017-2018Arlene MarasiganNo ratings yet
- Jamia Millia Islamia AlumniDocument128 pagesJamia Millia Islamia AlumniSm Arif100% (1)
- Lesson Plan de ComprasDocument22 pagesLesson Plan de Comprasamlande2No ratings yet
- Mang-Lesson Plan Template - ArtsDocument8 pagesMang-Lesson Plan Template - ArtsIverson MangNo ratings yet
- Math 5 Q2 FDocument41 pagesMath 5 Q2 FLorefe Delos SantosNo ratings yet