Download as pdf or txt
You might also like
- Surgery Clerkship Oral Exam ReviewDocument18 pagesSurgery Clerkship Oral Exam Reviewpanther795100% (1)
- Dermatitis SOAP NOTEDocument10 pagesDermatitis SOAP NOTEHugs100% (2)
- Refractive ErrorssDocument6 pagesRefractive ErrorssOphthalmology DiscussionNo ratings yet
- Refractive ErrorsDocument38 pagesRefractive ErrorszahraaNo ratings yet
- L2A Refractive ErrorsDocument34 pagesL2A Refractive ErrorsazraNo ratings yet
- Physics of Eyes and VisionDocument57 pagesPhysics of Eyes and VisionNIKHILA RAKESHNo ratings yet
- Optics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDDocument52 pagesOptics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDHidayadNo ratings yet
- TBL 1 - Refractive Error SlidesDocument66 pagesTBL 1 - Refractive Error SlidesAmirah Azman100% (4)
- Publication 4 8578 1650Document9 pagesPublication 4 8578 1650NIKHILA RAKESHNo ratings yet
- OphthalmologyDocument6 pagesOphthalmologyPeter AbikoyeNo ratings yet
- CH 11Document30 pagesCH 11piyushNo ratings yet
- Physics U2Document6 pagesPhysics U2Alima IqbalNo ratings yet
- Refraction and AccommodationDocument80 pagesRefraction and Accommodationapi-19916399100% (2)
- 2 Dioptrique de Loeil Normal 2021.anglaisDocument7 pages2 Dioptrique de Loeil Normal 2021.anglaisHoussemNo ratings yet
- Optics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDDocument52 pagesOptics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDShahar ShababNo ratings yet
- Refractive Errors: Dr. Leow Thye YngDocument55 pagesRefractive Errors: Dr. Leow Thye YngRaissaNo ratings yet
- Biophysics of The Visual SystemDocument5 pagesBiophysics of The Visual SystemIfe AzeezNo ratings yet
- Clinical Optics and Refractive Errors 09Document33 pagesClinical Optics and Refractive Errors 09somebody_maNo ratings yet
- Physiology of Optic-VioDocument42 pagesPhysiology of Optic-VioViora RiandaNo ratings yet
- Refractive errors-محولDocument9 pagesRefractive errors-محولYasin KadriNo ratings yet
- Special SensesDocument152 pagesSpecial SensesCor GuerreroNo ratings yet
- Human Eye Structure and Defects of VisionDocument25 pagesHuman Eye Structure and Defects of Visionmailansh904No ratings yet
- Error of RefractionDocument37 pagesError of RefractionIka KrastanayaNo ratings yet
- Error of RefractionDocument3 pagesError of RefractionMargot SanchezNo ratings yet
- Refractive ErrorsDocument6 pagesRefractive ErrorsMayur kaleNo ratings yet
- Phys ProjDocument11 pagesPhys Projben-jNo ratings yet
- Anisometropia 4Document18 pagesAnisometropia 4Mamtha MMNo ratings yet
- Refractive ErrorsDocument48 pagesRefractive Errorsnekko2230No ratings yet
- Visual AcuityDocument21 pagesVisual AcuityLynCapiliNo ratings yet
- Chap 4 MicrosDocument28 pagesChap 4 MicrosPatricio ArruéNo ratings yet
- 3 - Refractive ErrorsDocument17 pages3 - Refractive ErrorsF ParikhNo ratings yet
- Refraction Error VinaDocument27 pagesRefraction Error VinaHardiNo ratings yet
- Basic Optics 1Document52 pagesBasic Optics 1Mamtha MMNo ratings yet
- Physics of Eye and Vision - Updated DR Bakhtiar 2023Document46 pagesPhysics of Eye and Vision - Updated DR Bakhtiar 2023mhamadmhamad1184No ratings yet
- Human Eye and Colourful World: NotesDocument38 pagesHuman Eye and Colourful World: NotesEsha TwinkleNo ratings yet
- Why 25 CMDocument13 pagesWhy 25 CMEgiNo ratings yet
- The Optical Quality of The CorneaDocument32 pagesThe Optical Quality of The CorneaacalossiNo ratings yet
- Physics of The EyeDocument59 pagesPhysics of The EyePrincess Dianna SulitNo ratings yet
- PrismsDocument42 pagesPrismsa100% (1)
- Human EyeDocument9 pagesHuman EyeNimish MalhotraNo ratings yet
- Human Eye and Colourful World - Notes - 1Document4 pagesHuman Eye and Colourful World - Notes - 1Sidra EqbalNo ratings yet
- Humam EyeDocument7 pagesHumam EyeMahamNo ratings yet
- OPTIK Ketik UlangDocument8 pagesOPTIK Ketik Ulangad_campretNo ratings yet
- Refractive Errors: Dr. Kemal DikiciDocument77 pagesRefractive Errors: Dr. Kemal DikiciFirman CappoNo ratings yet
- The Eye-Optics, Retina, CNS1Document109 pagesThe Eye-Optics, Retina, CNS1Cor GuerreroNo ratings yet
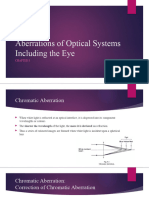
- Aberrations of Optical Systems Including The EyeDocument20 pagesAberrations of Optical Systems Including The EyeCherry OrtegaNo ratings yet
- What Is A Medical Device?Document5 pagesWhat Is A Medical Device?Jan Kenneth BarazonNo ratings yet
- 5-Eye and Vision-1Document63 pages5-Eye and Vision-1a7ma1212019No ratings yet
- Our Eye As A Camera Refraction, Errors and Solutions.: DR - Ali.A.Taqi Fifth Year StudentsDocument44 pagesOur Eye As A Camera Refraction, Errors and Solutions.: DR - Ali.A.Taqi Fifth Year Studentsabigail100% (1)
- Human Eye and The Colorful World NotesDocument17 pagesHuman Eye and The Colorful World NotesSourav MaityNo ratings yet
- Accommodation: Shubhangi ShuklaDocument17 pagesAccommodation: Shubhangi ShuklaShubhangi ShuklaNo ratings yet
- Jahandar Hajiyev-1Document33 pagesJahandar Hajiyev-1aze2005aze2020No ratings yet
- 14.9a Eye and VisionDocument40 pages14.9a Eye and VisionsotheenathansaideepikaaNo ratings yet
- Refractive Mgmt/Intervention: Question 1 of 90Document39 pagesRefractive Mgmt/Intervention: Question 1 of 90NoorNo ratings yet
- 2-Special SensesDocument63 pages2-Special Sensestmqt2fbnzgNo ratings yet
- 020 Errors PresbyopiaDocument131 pages020 Errors PresbyopiaSuhaila El MuzoghiNo ratings yet
- Refraction by The EyeDocument28 pagesRefraction by The EyeCherry OrtegaNo ratings yet
- Unit 2 - Study MaterialDocument11 pagesUnit 2 - Study MaterialKrunal ParmarNo ratings yet
- 10 Eye DefectsDocument7 pages10 Eye DefectsRogel Ramiterre100% (1)
- Detailed Notes - Section 10 Medical Physics - AQA Physics A-Level7956784564Document40 pagesDetailed Notes - Section 10 Medical Physics - AQA Physics A-Level7956784564David HolmesNo ratings yet
- Refractive ErrorsDocument19 pagesRefractive ErrorsAbdul Rafay ShaikhNo ratings yet
- Essential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 2 PDFDocument1 pageEssential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 2 PDFMariam Qais100% (1)
- C Major Scale - Fretboard Diagrams, Chords, Notes and Charts - Guitar Gear FinderDocument12 pagesC Major Scale - Fretboard Diagrams, Chords, Notes and Charts - Guitar Gear FinderMariam QaisNo ratings yet
- Essential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 137Document6 pagesEssential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 137Mariam QaisNo ratings yet
- Dermatomyositis: By: Mariam Qais Hatef - 5 Stage Supervised By: DR - Sabeeh AlmashhadaniDocument6 pagesDermatomyositis: By: Mariam Qais Hatef - 5 Stage Supervised By: DR - Sabeeh AlmashhadaniMariam QaisNo ratings yet
- The Relation Between Polycystic Ovarian Syndrome and BMI in Females at Age (15-30) y in Baghdad Medical City From 2015 To 2017Document6 pagesThe Relation Between Polycystic Ovarian Syndrome and BMI in Females at Age (15-30) y in Baghdad Medical City From 2015 To 2017Mariam QaisNo ratings yet
- اهداءDocument1 pageاهداءMariam QaisNo ratings yet
- Chapter One: Introduction and Literature ReviewDocument7 pagesChapter One: Introduction and Literature ReviewMariam QaisNo ratings yet
- Chapter 5Document2 pagesChapter 5Mariam QaisNo ratings yet
- 10Kuea6Bpgienymmt - Q2Mufbwq Z8Vqs5Iw6Lka7Lzbpe/EditDocument3 pages10Kuea6Bpgienymmt - Q2Mufbwq Z8Vqs5Iw6Lka7Lzbpe/EditMariam QaisNo ratings yet
- RMB2 16 67 PDFDocument5 pagesRMB2 16 67 PDFMariam QaisNo ratings yet
- Research Proposal Completion Certificate 1Document1 pageResearch Proposal Completion Certificate 1Mariam QaisNo ratings yet
- Nutrients: Weight Management Interventions in Women With and Without PCOS: A Systematic ReviewDocument19 pagesNutrients: Weight Management Interventions in Women With and Without PCOS: A Systematic ReviewMariam QaisNo ratings yet
- Hormonal Contraception in Women With Polycystic Ovary Syndrome: Choices, Challenges, and Noncontraceptive BenefitsDocument11 pagesHormonal Contraception in Women With Polycystic Ovary Syndrome: Choices, Challenges, and Noncontraceptive BenefitsMariam QaisNo ratings yet
- Polycystic Ovary Syndrome - Definition, ..Document24 pagesPolycystic Ovary Syndrome - Definition, ..Mariam QaisNo ratings yet
- 404 2017 Article 4623 PDFDocument9 pages404 2017 Article 4623 PDFMariam QaisNo ratings yet
- Clinical, Biochemical, and Hormonal Associations in Female Patients With AcneDocument7 pagesClinical, Biochemical, and Hormonal Associations in Female Patients With AcneMariam QaisNo ratings yet
- 2017 Article 313 PDFDocument17 pages2017 Article 313 PDFMariam QaisNo ratings yet
- Polycystic Ovary Syndrome and Circulating Inflammatory MarkersDocument8 pagesPolycystic Ovary Syndrome and Circulating Inflammatory MarkersMariam QaisNo ratings yet
- HDTD-E-1 Introduction To EmbryologyDocument14 pagesHDTD-E-1 Introduction To EmbryologyMariam QaisNo ratings yet
- Microsoft Word - Aow 11-15-20Document2 pagesMicrosoft Word - Aow 11-15-20api-539266252No ratings yet
- Module 3 - ProteobacteriaDocument63 pagesModule 3 - ProteobacteriaReginaNo ratings yet
- Textbook Ebook The Mistress of Bhatia House Sujata Massey All Chapter PDFDocument43 pagesTextbook Ebook The Mistress of Bhatia House Sujata Massey All Chapter PDFeugenio.stern776100% (7)
- ENGLISH FOR NURSING-FIKES 6, Mita Suci R 701180002Document4 pagesENGLISH FOR NURSING-FIKES 6, Mita Suci R 701180002MitaNo ratings yet
- Sheet: OSHA's Bloodborne Pathogens StandardDocument2 pagesSheet: OSHA's Bloodborne Pathogens StandardAaquil RaziNo ratings yet
- MINOR DISORDER IN PREGNANCY MaterialDocument8 pagesMINOR DISORDER IN PREGNANCY MaterialAnuradha Maurya100% (1)
- Factor Affecting HIV and AIDs ProgressionDocument15 pagesFactor Affecting HIV and AIDs Progressionbilkiz chauriraNo ratings yet
- TBT-Heat Disorders - DehydrationDocument2 pagesTBT-Heat Disorders - DehydrationRohit SinghNo ratings yet
- Kyasanur Forest DiseaseDocument11 pagesKyasanur Forest DiseasesurabhisprNo ratings yet
- Conversion Disorder-1Document11 pagesConversion Disorder-1zainiNo ratings yet
- Brosura Belgica de Weerd 2010Document22 pagesBrosura Belgica de Weerd 2010dlgdesignsrvNo ratings yet
- Trigeminal NeuralgiaDocument4 pagesTrigeminal Neuralgiawally ziembickiNo ratings yet
- WHO Risk Assessment Template - Annex2Document7 pagesWHO Risk Assessment Template - Annex2Chester KyleNo ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Journal Homepage: - : ObservationDocument10 pagesJournal Homepage: - : ObservationIJAR JOURNALNo ratings yet
- PneumoniaDocument5 pagesPneumoniarjshubhNo ratings yet
- Protein-Losing Enteropathy: Francisco A. SylvesterDocument10 pagesProtein-Losing Enteropathy: Francisco A. SylvesterNIKEN PUSPITASARINo ratings yet
- HTP FinalDocument3 pagesHTP Finalאורזלין לנזוןNo ratings yet
- Resultados SaludDignaDocument2 pagesResultados SaludDignaAdriana RamosNo ratings yet
- Amilase LipaseDocument7 pagesAmilase LipaseNovindy Lubis FahlawaniNo ratings yet
- Salivary Gland DisordersDocument30 pagesSalivary Gland DisordersSangeeta BSRNo ratings yet
- NASM Essentials of Personal Fitness Training: Chapter 1 - Lab ActivityDocument2 pagesNASM Essentials of Personal Fitness Training: Chapter 1 - Lab ActivityNosce Te IpsumNo ratings yet
- Congenital Diaphragmatic HerniaDocument48 pagesCongenital Diaphragmatic HerniaShahd IdaisNo ratings yet
- Neuropsychological Rehabilitation For Traumatic Brain Injury Patients PDFDocument12 pagesNeuropsychological Rehabilitation For Traumatic Brain Injury Patients PDFFausto D. GomezNo ratings yet
- Whooping CoughDocument9 pagesWhooping Coughvaishali TMU studentNo ratings yet
- Report HPV, Shingles and Chicken PoxDocument4 pagesReport HPV, Shingles and Chicken PoxJarold PerezNo ratings yet
- Maersk VN - Benefit Summary - Staff - 2020 (En)Document36 pagesMaersk VN - Benefit Summary - Staff - 2020 (En)Thanh TraNo ratings yet
- CP Opd Lec Cuartero MidDocument7 pagesCP Opd Lec Cuartero MidjimwelluismNo ratings yet