Download as pdf or txt
You might also like
- Accuracy of Half Guided Implant Placement With Machine DrivenDocument9 pagesAccuracy of Half Guided Implant Placement With Machine DrivenGustavo IsmaelNo ratings yet
- CVC Reading PassagesDocument8 pagesCVC Reading PassagesChase Smythe100% (1)
- 4L80EDocument156 pages4L80EJames Winsor100% (14)
- Artificial Intelligence in Dentistry Current Applications and Future PerspectivesDocument10 pagesArtificial Intelligence in Dentistry Current Applications and Future PerspectivesSkAliHassanNo ratings yet
- Eastar SpecificationsDocument2 pagesEastar SpecificationsUmar ShamsudinNo ratings yet
- Comparison of Conventional PhotogrammetrDocument9 pagesComparison of Conventional PhotogrammetrPhạm CườngNo ratings yet
- Precision and Accuracy of A Digital Impression Scanner in Full-Arch Implant RehabilitationDocument5 pagesPrecision and Accuracy of A Digital Impression Scanner in Full-Arch Implant Rehabilitationgeorgios031No ratings yet
- Ear ProsthesisDocument6 pagesEar ProsthesisSkAliHassan100% (1)
- DR Meni Implanto 1Document7 pagesDR Meni Implanto 1Itzel MarquezNo ratings yet
- Comparison of Accuracy Between A Conventional and Two Digital Intraoral Impression TechniquesDocument7 pagesComparison of Accuracy Between A Conventional and Two Digital Intraoral Impression TechniquesDiego LopezNo ratings yet
- Accuracy of Impressions For Multiple Implants A ComparativeDocument7 pagesAccuracy of Impressions For Multiple Implants A Comparativewaf51No ratings yet
- Cise Ozal 2021Document12 pagesCise Ozal 2021Smrithi N SNo ratings yet
- Accuracy of Different SurgicalDocument8 pagesAccuracy of Different SurgicalVõHoàngThủyTiênNo ratings yet
- Document Primescan Accuracy In-Vitro EnderDocument9 pagesDocument Primescan Accuracy In-Vitro Enderelbanuswatri1980No ratings yet
- Mehl ArticleDocument9 pagesMehl ArticleMaría Fernanda Montealegre ZuluagaNo ratings yet
- S - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryDocument7 pagesS - 2019 - Influence of Implant Macrodesign and Insertion Connection Technology On The Accuracy of Static Computer-Assisted Implant SurgeryVõHoàngThủyTiênNo ratings yet
- Digital Work Flow of Custom AbutmentDocument10 pagesDigital Work Flow of Custom AbutmentmustafaNo ratings yet
- Guided Surgery in Dental ImplantologyDocument5 pagesGuided Surgery in Dental Implantologynarendra singhNo ratings yet
- Accuracy of Computer-Aided Template-Guided Oral Implant Placement A Prospective Clinical StudyDocument10 pagesAccuracy of Computer-Aided Template-Guided Oral Implant Placement A Prospective Clinical StudyMário LúcioNo ratings yet
- Efficacy of Implant Placement With Surgical Guides in T 2022 Advances in OraDocument6 pagesEfficacy of Implant Placement With Surgical Guides in T 2022 Advances in OraГне ДзжNo ratings yet
- Impacto de Los Scan BodiesDocument6 pagesImpacto de Los Scan Bodiesjuanandresro93No ratings yet
- EPA Consensus Project Paper Accuracy of Photogrammetry Devices Intraoral Scanners and Conventional Techniques For The Full Arch Implant Impressions A Systematic ReviewDocument12 pagesEPA Consensus Project Paper Accuracy of Photogrammetry Devices Intraoral Scanners and Conventional Techniques For The Full Arch Implant Impressions A Systematic Reviewcasto.carpetasmiaNo ratings yet
- Novellino 2013Document6 pagesNovellino 2013Glais FerrariNo ratings yet
- Boeddinghaus 2015Document8 pagesBoeddinghaus 2015wellington_cmlNo ratings yet
- CJDR 2022 03 s0215Document8 pagesCJDR 2022 03 s0215Hernández López Nubia HedherNo ratings yet
- 2019 - Yeung Et Al - Accuracy and Precision of 3d-Printed Implant Surgical Guideswith Different Implant Systems An in Vitro StudyDocument8 pages2019 - Yeung Et Al - Accuracy and Precision of 3d-Printed Implant Surgical Guideswith Different Implant Systems An in Vitro StudyRafael FedaltoNo ratings yet
- Avrampou COIR 2013Document8 pagesAvrampou COIR 2013jose luis delgadilloNo ratings yet
- Comparison of The Clinical Accuracy of Digital and Conventional Dental Implant ImpressionsDocument9 pagesComparison of The Clinical Accuracy of Digital and Conventional Dental Implant ImpressionsCaroline AngoneseNo ratings yet
- 10 1016@j Prosdent 2019 05 027Document8 pages10 1016@j Prosdent 2019 05 027OctavioJose DuarteFrenkyNo ratings yet
- Uso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaDocument7 pagesUso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaPaola Alexandra LaguadoNo ratings yet
- Final Article JopDocument6 pagesFinal Article JopNaina TalwarNo ratings yet
- Comparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Document7 pagesComparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Alex BurdeNo ratings yet
- 2023JP - Papaspyridakos - Reverse Scan Body A Complete Digital Workflow For Prosthesis PrototypeDocument6 pages2023JP - Papaspyridakos - Reverse Scan Body A Complete Digital Workflow For Prosthesis PrototypedrjonduNo ratings yet
- Digital Dentures A Protocol Based On Intraoral SCDocument6 pagesDigital Dentures A Protocol Based On Intraoral SCirfan dNo ratings yet
- Journal of Prosthodontics - 2023 - Marshaha - Evaluation of The Trueness and Precision of Conventional Impressions VersusDocument9 pagesJournal of Prosthodontics - 2023 - Marshaha - Evaluation of The Trueness and Precision of Conventional Impressions VersusraulguerragoesNo ratings yet
- Implant Planning and Placement Using Optical Scanning and Cone Beam CT TechnologyDocument6 pagesImplant Planning and Placement Using Optical Scanning and Cone Beam CT TechnologyPraveen Raj ThakurNo ratings yet
- Accuracy of Implant Placement With A Esterolitografia PDFDocument8 pagesAccuracy of Implant Placement With A Esterolitografia PDFSamuel Flores CalderonNo ratings yet
- Implant Positioning Errors in Freehand and Computeraided Placement Methods A Singleblind Clinical Comparative StudyDocument15 pagesImplant Positioning Errors in Freehand and Computeraided Placement Methods A Singleblind Clinical Comparative StudyDenisa CorneaNo ratings yet
- Using Intraoral Scanning To Fabricate Complete Dentures: First ExperiencesDocument5 pagesUsing Intraoral Scanning To Fabricate Complete Dentures: First ExperiencesgermanpuigNo ratings yet
- Jeong 2016Document5 pagesJeong 2016francisco EscorciaNo ratings yet
- Precision of Intraoral Digital Dental Impressions With ITero and Extraoral Digitization With The ITero and A Model ScannerDocument8 pagesPrecision of Intraoral Digital Dental Impressions With ITero and Extraoral Digitization With The ITero and A Model ScannerAlex BurdeNo ratings yet
- Jced 13 E487Document6 pagesJced 13 E487Rafaela VillamaguaNo ratings yet
- Prosthetic Rehabilitation of An Edentulous Patient With Microstomia Using Both Digital and Conventional Techniques: A Clinical ReportDocument5 pagesProsthetic Rehabilitation of An Edentulous Patient With Microstomia Using Both Digital and Conventional Techniques: A Clinical ReportDwi Isti NadiarohNo ratings yet
- Clinical Oral Implants Res - 2018 - Tahmaseb - The Accuracy of Static Computer Aided Implant Surgery A Systematic ReviewDocument20 pagesClinical Oral Implants Res - 2018 - Tahmaseb - The Accuracy of Static Computer Aided Implant Surgery A Systematic ReviewOctavioJose DuarteFrenkyNo ratings yet
- Comparative Evaluation of Vertical and Lateral Gingival Displacement Produced by MecDocument8 pagesComparative Evaluation of Vertical and Lateral Gingival Displacement Produced by MecInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Accuracy of Intraoral Scans An in Vivo Study of DiDocument7 pagesAccuracy of Intraoral Scans An in Vivo Study of DiRaul Alfonsin SanchezNo ratings yet
- 10 1002@jemt 23503Document6 pages10 1002@jemt 23503Guilherme AndradeNo ratings yet
- 10 1016@j Prosdent 2020 02 011Document6 pages10 1016@j Prosdent 2020 02 011ahm nNo ratings yet
- Comparison of The Clinical Accuracy of DDocument9 pagesComparison of The Clinical Accuracy of DDoctor JackNo ratings yet
- Three-Dimensional Maxillary Virtual Patient Creation by Convolutional Neural Network-Based Segmentation On Cone-Beam Computed Tomography ImagesDocument9 pagesThree-Dimensional Maxillary Virtual Patient Creation by Convolutional Neural Network-Based Segmentation On Cone-Beam Computed Tomography Imagesnerminmorgan2020No ratings yet
- 2004 - Navigation Surgery For Dental Implants Assessment of Accuracy of The Image Guided Implantology SystemDocument4 pages2004 - Navigation Surgery For Dental Implants Assessment of Accuracy of The Image Guided Implantology SystemVõHoàngThủyTiênNo ratings yet
- 65 - JPR - D - 20 - 00169 - 1Document7 pages65 - JPR - D - 20 - 00169 - 1Gt SolarcNo ratings yet
- Pubb 1 BDJ The Accuracy of Intral Oral Scanners FinalDocument13 pagesPubb 1 BDJ The Accuracy of Intral Oral Scanners Finalmarcofriuli2No ratings yet
- Content ServerDocument8 pagesContent ServerJuan Carlos MeloNo ratings yet
- Boltons Analysis Using A Photogrammetric Method oDocument7 pagesBoltons Analysis Using A Photogrammetric Method oSarah Ariefah SantriNo ratings yet
- Running Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Document16 pagesRunning Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Roja AllampallyNo ratings yet
- An Evaluation of Impression Techniques For Multiple Internal Connection Implant ProsthesesDocument7 pagesAn Evaluation of Impression Techniques For Multiple Internal Connection Implant Prosthesesalmastar officeNo ratings yet
- 50Document3 pages50Lais AmandaNo ratings yet
- The Accuracy of Different Dental Impression Techniques For Implant-Supported Dental Prostheses: A Systematic Review and Meta - AnalysisDocument19 pagesThe Accuracy of Different Dental Impression Techniques For Implant-Supported Dental Prostheses: A Systematic Review and Meta - AnalysisAnonymous AyxIccS4aXNo ratings yet
- Accuracy of Implant Placement With Computer-Guided SurgeryDocument15 pagesAccuracy of Implant Placement With Computer-Guided SurgerydentureNo ratings yet
- Evaluation of The Effect of Implant Scan Body MateDocument15 pagesEvaluation of The Effect of Implant Scan Body MatePhạm CườngNo ratings yet
- 10.1016@j.prosdent.2016.01.004.PdfAdaptation of An Interim Partial Removable Dental Prosthesis As A Radiographic Template For Implant PlacementDocument2 pages10.1016@j.prosdent.2016.01.004.PdfAdaptation of An Interim Partial Removable Dental Prosthesis As A Radiographic Template For Implant PlacementdentureNo ratings yet
- Thanasrisuebwong - Influence of The Residual Ridge Widths and Implant Thread Designs OnDocument7 pagesThanasrisuebwong - Influence of The Residual Ridge Widths and Implant Thread Designs OnGustavo IsmaelNo ratings yet
- Zygomatic Implants: Optimization and InnovationFrom EverandZygomatic Implants: Optimization and InnovationJames ChowNo ratings yet
- 8TH Reference ThesisDocument8 pages8TH Reference ThesisSkAliHassanNo ratings yet
- OICL AO 2017 Prelims Previous Year PaperDocument67 pagesOICL AO 2017 Prelims Previous Year PaperSkAliHassanNo ratings yet
- J Prosdent 2020 05 035Document3 pagesJ Prosdent 2020 05 035SkAliHassanNo ratings yet
- 35 Ref ThesisDocument7 pages35 Ref ThesisSkAliHassanNo ratings yet
- BBBFDocument3 pagesBBBFSkAliHassanNo ratings yet
- Informed Consent Form For General Dental Procedures2Document3 pagesInformed Consent Form For General Dental Procedures2SkAliHassanNo ratings yet
- A Neutral Zone Concept - An Overview: Dr. Anagha R. Dafade, Dr. Alhad I. GiradkarDocument5 pagesA Neutral Zone Concept - An Overview: Dr. Anagha R. Dafade, Dr. Alhad I. GiradkarSkAliHassanNo ratings yet
- JioMart Invoice 16501052870178594A 1Document1 pageJioMart Invoice 16501052870178594A 1SkAliHassanNo ratings yet
- Porcelain Laminate Veneers 978-3-659-38967-2 Laminate VeneersDocument2 pagesPorcelain Laminate Veneers 978-3-659-38967-2 Laminate VeneersSkAliHassanNo ratings yet
- Provisional Restorations in Restorative Dentistry: University After M. Heratsi Yerevan, ArmeniaDocument7 pagesProvisional Restorations in Restorative Dentistry: University After M. Heratsi Yerevan, ArmeniaSkAliHassanNo ratings yet
- DownloadDocument4 pagesDownloadSkAliHassanNo ratings yet
- EffectofpositioningDocument7 pagesEffectofpositioningSkAliHassanNo ratings yet
- Zone - 1 - LIST OF CANDIDATES NOT ELIGIBLE FOR THE POST OF MLHPDocument32 pagesZone - 1 - LIST OF CANDIDATES NOT ELIGIBLE FOR THE POST OF MLHPSkAliHassanNo ratings yet
- FMR OcclusionDocument10 pagesFMR OcclusionSkAliHassanNo ratings yet
- The Split Denture: A New Technique For Artificial Saliva Reservoirs in Mandibular DenturesDocument5 pagesThe Split Denture: A New Technique For Artificial Saliva Reservoirs in Mandibular DenturesSkAliHassanNo ratings yet
- Application of Artificial Intelligence inDocument4 pagesApplication of Artificial Intelligence inSkAliHassanNo ratings yet
- Direct Fiber-Reinforced Composite Bridges - Dentistry TodayDocument12 pagesDirect Fiber-Reinforced Composite Bridges - Dentistry TodaySkAliHassanNo ratings yet
- Biomedical Waste Management in Dental Office-A Review: January 2018Document6 pagesBiomedical Waste Management in Dental Office-A Review: January 2018SkAliHassanNo ratings yet
- Occlusal Forms and Philosophies in Full Mouth Rehabilitation: A Literature ReviewDocument5 pagesOcclusal Forms and Philosophies in Full Mouth Rehabilitation: A Literature ReviewSkAliHassanNo ratings yet
- Ce Artificial Using Dentures Partial Removable DesigningDocument4 pagesCe Artificial Using Dentures Partial Removable DesigningSkAliHassanNo ratings yet
- Catch It Right - A Case Report On Occlusal SplintDocument6 pagesCatch It Right - A Case Report On Occlusal SplintSkAliHassanNo ratings yet
- Alloys in ProsthodonticsDocument4 pagesAlloys in ProsthodonticsSkAliHassanNo ratings yet
- Mathematics: Quarter 1 - Module 8: Division of Whole Numbers by Decimals Up To 2 Decimal PlacesDocument34 pagesMathematics: Quarter 1 - Module 8: Division of Whole Numbers by Decimals Up To 2 Decimal PlacesJohn Thomas Satimbre100% (1)
- ACDC - Lucina - DatasheetDocument1 pageACDC - Lucina - Datasheetwincad_sgNo ratings yet
- 1 s2.0 S096098221730708X MainDocument5 pages1 s2.0 S096098221730708X Mainrotinda bilekNo ratings yet
- Nimble Number Logic Puzzle II QuizDocument1 pageNimble Number Logic Puzzle II QuizpikNo ratings yet
- Allen Bradley 160 C SeriesDocument28 pagesAllen Bradley 160 C SeriesTihomir Matulić100% (1)
- Selection Post IX Graduation 08-02-2022 EngDocument156 pagesSelection Post IX Graduation 08-02-2022 EngVijay singh TomarNo ratings yet
- Month + Teaching Days Unit Total Teaching Periods: Vibgyor High Grade - 2 English Literature Year Plan (AY 2020 - 2021)Document65 pagesMonth + Teaching Days Unit Total Teaching Periods: Vibgyor High Grade - 2 English Literature Year Plan (AY 2020 - 2021)TAPASsenguptaNo ratings yet
- Comm 1100 Info Speech (Tolentino, Nirelle V.)Document5 pagesComm 1100 Info Speech (Tolentino, Nirelle V.)Nirelle TolentinoNo ratings yet
- Exercise Oracle Forms 6i TrainingDocument5 pagesExercise Oracle Forms 6i TrainingFarooq Shahid100% (1)
- WINPROPDocument296 pagesWINPROPEfrain Ramirez Chavez100% (2)
- 3 Generations of Human RightsDocument1 page3 Generations of Human RightsDzenan HakalovicNo ratings yet
- Detailed Lesson Plan in ICT ExcelDocument5 pagesDetailed Lesson Plan in ICT ExcelColleen Vender100% (3)
- 12B TB Book PDF-1 PDFDocument113 pages12B TB Book PDF-1 PDFامل العودة طالب100% (1)
- Business Freedom: An Animated Powerpoint TemplateDocument19 pagesBusiness Freedom: An Animated Powerpoint TemplateKevin LpsNo ratings yet
- Soal Quizziz Buat Sendiri Kelas Xii TTG News ItemDocument6 pagesSoal Quizziz Buat Sendiri Kelas Xii TTG News ItemJorus RukuNo ratings yet
- Application Form For Initial Review: Section A - Basic InformationDocument33 pagesApplication Form For Initial Review: Section A - Basic Informationsaptarshi DasNo ratings yet
- The Preschooler and The SchoolerDocument16 pagesThe Preschooler and The Schoolerquidditch07No ratings yet
- Performance: Task in Math 8 House Floor PlanDocument10 pagesPerformance: Task in Math 8 House Floor PlanJoshua Emmanuel LedesmaNo ratings yet
- Oxford Thesis CollectionDocument5 pagesOxford Thesis Collectionkimberlybundypittsburgh100% (2)
- Staff Data Format-AUCDocument1 pageStaff Data Format-AUCSenthil KumarNo ratings yet
- Linear Programming TheoryDocument104 pagesLinear Programming Theorykostas_ntougias5453No ratings yet
- Proposal Nur Azizah 2315059 R1Document34 pagesProposal Nur Azizah 2315059 R1zizieNo ratings yet
- Front Wheel Assy. DrumDocument2 pagesFront Wheel Assy. DrumSoroj BiswasNo ratings yet
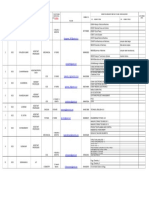
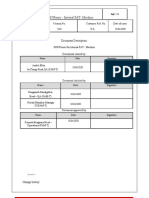
- SOP - Internal FAT-MachineDocument12 pagesSOP - Internal FAT-MachineSarvesh DaradeNo ratings yet
- Chapter 9: TidesDocument40 pagesChapter 9: TidesCarol GirottoNo ratings yet
- F101-1 Client Information Form and ApprovalDocument4 pagesF101-1 Client Information Form and ApprovalgoyalpramodNo ratings yet
- Futures - Tiempos Futuros BBDocument10 pagesFutures - Tiempos Futuros BBLuz DuranteNo ratings yet