
Growth Anti-Myostatin
Growth Anti-Myostatin
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Blood Pressure Levels For Boys by Age and Height PercentileDocument4 pagesBlood Pressure Levels For Boys by Age and Height PercentileNuzla EmiraNo ratings yet
- BLS PDFDocument6 pagesBLS PDFAyesha JadoonNo ratings yet
- Let Me Break It Down For YouDocument119 pagesLet Me Break It Down For YouoscarnineNo ratings yet
- Electromagnetic Emission From Humans During Focused IntentDocument20 pagesElectromagnetic Emission From Humans During Focused IntentoscarnineNo ratings yet
- A Brief Summary of The DNA-derived Frequency TheoryDocument4 pagesA Brief Summary of The DNA-derived Frequency TheoryoscarnineNo ratings yet
- Electronics and Brain ControlDocument5 pagesElectronics and Brain ControloscarnineNo ratings yet
- Hypo-Magnetic StudyDocument51 pagesHypo-Magnetic StudyoscarnineNo ratings yet
- Phillips The Queen (No. 2) Court of Criminal Appeal: Burbury C.) ., Crawford and Nettlefold Nov. 9, 10, Dec. 22, 1971Document18 pagesPhillips The Queen (No. 2) Court of Criminal Appeal: Burbury C.) ., Crawford and Nettlefold Nov. 9, 10, Dec. 22, 1971oscarnineNo ratings yet
- Atoms Emit Radio WavesDocument10 pagesAtoms Emit Radio WavesoscarnineNo ratings yet
- Experiments in Mental SuggestionDocument3 pagesExperiments in Mental Suggestionoscarnine0% (1)
- HHS Public Access: Slowing Ageing by Design: The Rise of NAD and Sirtuin-Activating CompoundsDocument29 pagesHHS Public Access: Slowing Ageing by Design: The Rise of NAD and Sirtuin-Activating CompoundsoscarnineNo ratings yet
- Teleomere LengtheningDocument5 pagesTeleomere LengtheningoscarnineNo ratings yet
- Anti-Vaccine TestimonyDocument48 pagesAnti-Vaccine TestimonyoscarnineNo ratings yet
- Skills,: Perceptual AndmotorDocument27 pagesSkills,: Perceptual AndmotoroscarnineNo ratings yet
- Trial On IndictmentDocument74 pagesTrial On IndictmentoscarnineNo ratings yet
- EU Area Residents' Step-by-Step Guide To Escaping The Upcoming Bank Bail-Ins & Capital ControlsDocument55 pagesEU Area Residents' Step-by-Step Guide To Escaping The Upcoming Bank Bail-Ins & Capital ControlsoscarnineNo ratings yet
- Electronicsbehindv 2 KDocument17 pagesElectronicsbehindv 2 KoscarnineNo ratings yet
- Alternative Cancer TreatmentDocument2 pagesAlternative Cancer TreatmentoscarnineNo ratings yet
- The Biology of Emotions: Redirecting Self-Therapy (RST) For Anxiety and DepressionDocument4 pagesThe Biology of Emotions: Redirecting Self-Therapy (RST) For Anxiety and DepressionoscarnineNo ratings yet
- The Aggregation Problem: Implications For Ecological and Biophysical EconomicsDocument34 pagesThe Aggregation Problem: Implications For Ecological and Biophysical EconomicsoscarnineNo ratings yet
- .Dr. Thompson Sound Chair Specs - CNR 102 - W Audio Options - 01-17 PDFDocument1 page.Dr. Thompson Sound Chair Specs - CNR 102 - W Audio Options - 01-17 PDFoscarnineNo ratings yet
- Resonances and Planetary HarmonicsDocument124 pagesResonances and Planetary Harmonicsoscarnine100% (1)
- Antoine Priore - US Patent # 3,280,816, Method of Producing Radiations For Penetrating Living CellsDocument15 pagesAntoine Priore - US Patent # 3,280,816, Method of Producing Radiations For Penetrating Living CellsoscarnineNo ratings yet
- WWII TechnologyDocument48 pagesWWII TechnologyoscarnineNo ratings yet
- Presentation On Success Story of Yamaha and SonyDocument12 pagesPresentation On Success Story of Yamaha and SonyAchyuta AngadiNo ratings yet
- Transferring Between Bed and ChairDocument3 pagesTransferring Between Bed and ChairKceey Cruz100% (1)
- Q Bank Chem MCD Viii 2019Document19 pagesQ Bank Chem MCD Viii 2019hgbv tttbNo ratings yet
- Sonia Research ProposalDocument59 pagesSonia Research Proposalmullamuskaan95No ratings yet
- LOROFF, Nicole - Gender and Sexuality in Nazi Germany PDFDocument13 pagesLOROFF, Nicole - Gender and Sexuality in Nazi Germany PDFClara LimaNo ratings yet
- Asnt Ut Q&aDocument63 pagesAsnt Ut Q&axia100% (3)
- RS 232 Repeater KFD2-FF-Ex2.RS232: FunctionDocument4 pagesRS 232 Repeater KFD2-FF-Ex2.RS232: FunctionEder AlexandreNo ratings yet
- Valuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDocument4 pagesValuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDinesh Babu PugalenthiNo ratings yet
- Solomon Islands Position PaperDocument2 pagesSolomon Islands Position PaperAJ Ammons0% (1)
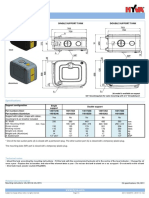
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- Winkler, W & Pelosi - 2022 - Understanding Breast CancerDocument76 pagesWinkler, W & Pelosi - 2022 - Understanding Breast CancerJordan KopongNo ratings yet
- Surfactant FloodingDocument13 pagesSurfactant FloodingVlassis SarantinosNo ratings yet
- Charity and Gift Giving (Choi)Document28 pagesCharity and Gift Giving (Choi)ROGEL SONo ratings yet
- Transport ProcessesDocument81 pagesTransport ProcessesKukre BertNo ratings yet
- Topic 5 AC To AC ConverterDocument53 pagesTopic 5 AC To AC ConverterNorain ZakariaNo ratings yet
- PCAR Contractors ManualDocument219 pagesPCAR Contractors ManualDefendAChildNo ratings yet
- Chlorine Dosing PumpDocument24 pagesChlorine Dosing PumpByron HisseyNo ratings yet
- Social and Self Control TheoryDocument2 pagesSocial and Self Control TheoryKarl Amiel EspirituNo ratings yet
- Silicic Acid Agro Technology: DescriptionDocument1 pageSilicic Acid Agro Technology: DescriptionKeniel BarrettNo ratings yet
- Funding Proposal: WebsiteDocument8 pagesFunding Proposal: Websitemajiamal99No ratings yet
- (II) Misadventure Is Mischance, Accident or Disaster. It Is of Three TypesDocument3 pages(II) Misadventure Is Mischance, Accident or Disaster. It Is of Three TypesSandeep BansalNo ratings yet
- Suzumar Boat Engine PackagesDocument7 pagesSuzumar Boat Engine PackagesmarkoNo ratings yet
- Recruitment MSCDocument40 pagesRecruitment MSCViji MNo ratings yet
- Company Profile Kalgen Innolab Innobiogram - 2022Document12 pagesCompany Profile Kalgen Innolab Innobiogram - 2022asmadi arrumNo ratings yet
- Unfuck Your Anilingus - How To Keep Your Oral Butt Sex Classy - Faith G Harper - 2022 - Microcosm Publishing - 9781648411618 - Anna's ArchiveDocument28 pagesUnfuck Your Anilingus - How To Keep Your Oral Butt Sex Classy - Faith G Harper - 2022 - Microcosm Publishing - 9781648411618 - Anna's Archiverhy4kjgqx6No ratings yet
- Petroleum Refining Notes 1Document5 pagesPetroleum Refining Notes 1api-304149645No ratings yet
- Coevolution of Hosts and ParasitesDocument5 pagesCoevolution of Hosts and ParasitesAshok KoyiNo ratings yet
- Divergent Plate BoundaryDocument4 pagesDivergent Plate BoundaryGreg ManNo ratings yet



























































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Blood Pressure Levels For Boys by Age and Height PercentileDocument4 pagesBlood Pressure Levels For Boys by Age and Height PercentileNuzla EmiraNo ratings yet
- BLS PDFDocument6 pagesBLS PDFAyesha JadoonNo ratings yet
- Let Me Break It Down For YouDocument119 pagesLet Me Break It Down For YouoscarnineNo ratings yet
- Electromagnetic Emission From Humans During Focused IntentDocument20 pagesElectromagnetic Emission From Humans During Focused IntentoscarnineNo ratings yet
- A Brief Summary of The DNA-derived Frequency TheoryDocument4 pagesA Brief Summary of The DNA-derived Frequency TheoryoscarnineNo ratings yet
- Electronics and Brain ControlDocument5 pagesElectronics and Brain ControloscarnineNo ratings yet
- Hypo-Magnetic StudyDocument51 pagesHypo-Magnetic StudyoscarnineNo ratings yet
- Phillips The Queen (No. 2) Court of Criminal Appeal: Burbury C.) ., Crawford and Nettlefold Nov. 9, 10, Dec. 22, 1971Document18 pagesPhillips The Queen (No. 2) Court of Criminal Appeal: Burbury C.) ., Crawford and Nettlefold Nov. 9, 10, Dec. 22, 1971oscarnineNo ratings yet
- Atoms Emit Radio WavesDocument10 pagesAtoms Emit Radio WavesoscarnineNo ratings yet
- Experiments in Mental SuggestionDocument3 pagesExperiments in Mental Suggestionoscarnine0% (1)
- HHS Public Access: Slowing Ageing by Design: The Rise of NAD and Sirtuin-Activating CompoundsDocument29 pagesHHS Public Access: Slowing Ageing by Design: The Rise of NAD and Sirtuin-Activating CompoundsoscarnineNo ratings yet
- Teleomere LengtheningDocument5 pagesTeleomere LengtheningoscarnineNo ratings yet
- Anti-Vaccine TestimonyDocument48 pagesAnti-Vaccine TestimonyoscarnineNo ratings yet
- Skills,: Perceptual AndmotorDocument27 pagesSkills,: Perceptual AndmotoroscarnineNo ratings yet
- Trial On IndictmentDocument74 pagesTrial On IndictmentoscarnineNo ratings yet
- EU Area Residents' Step-by-Step Guide To Escaping The Upcoming Bank Bail-Ins & Capital ControlsDocument55 pagesEU Area Residents' Step-by-Step Guide To Escaping The Upcoming Bank Bail-Ins & Capital ControlsoscarnineNo ratings yet
- Electronicsbehindv 2 KDocument17 pagesElectronicsbehindv 2 KoscarnineNo ratings yet
- Alternative Cancer TreatmentDocument2 pagesAlternative Cancer TreatmentoscarnineNo ratings yet
- The Biology of Emotions: Redirecting Self-Therapy (RST) For Anxiety and DepressionDocument4 pagesThe Biology of Emotions: Redirecting Self-Therapy (RST) For Anxiety and DepressionoscarnineNo ratings yet
- The Aggregation Problem: Implications For Ecological and Biophysical EconomicsDocument34 pagesThe Aggregation Problem: Implications For Ecological and Biophysical EconomicsoscarnineNo ratings yet
- .Dr. Thompson Sound Chair Specs - CNR 102 - W Audio Options - 01-17 PDFDocument1 page.Dr. Thompson Sound Chair Specs - CNR 102 - W Audio Options - 01-17 PDFoscarnineNo ratings yet
- Resonances and Planetary HarmonicsDocument124 pagesResonances and Planetary Harmonicsoscarnine100% (1)
- Antoine Priore - US Patent # 3,280,816, Method of Producing Radiations For Penetrating Living CellsDocument15 pagesAntoine Priore - US Patent # 3,280,816, Method of Producing Radiations For Penetrating Living CellsoscarnineNo ratings yet
- WWII TechnologyDocument48 pagesWWII TechnologyoscarnineNo ratings yet
- Presentation On Success Story of Yamaha and SonyDocument12 pagesPresentation On Success Story of Yamaha and SonyAchyuta AngadiNo ratings yet
- Transferring Between Bed and ChairDocument3 pagesTransferring Between Bed and ChairKceey Cruz100% (1)
- Q Bank Chem MCD Viii 2019Document19 pagesQ Bank Chem MCD Viii 2019hgbv tttbNo ratings yet
- Sonia Research ProposalDocument59 pagesSonia Research Proposalmullamuskaan95No ratings yet
- LOROFF, Nicole - Gender and Sexuality in Nazi Germany PDFDocument13 pagesLOROFF, Nicole - Gender and Sexuality in Nazi Germany PDFClara LimaNo ratings yet
- Asnt Ut Q&aDocument63 pagesAsnt Ut Q&axia100% (3)
- RS 232 Repeater KFD2-FF-Ex2.RS232: FunctionDocument4 pagesRS 232 Repeater KFD2-FF-Ex2.RS232: FunctionEder AlexandreNo ratings yet
- Valuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDocument4 pagesValuing The Suitable Agro-Industrial Wastes For Cultivation of P. Platypus and P. EousDinesh Babu PugalenthiNo ratings yet
- Solomon Islands Position PaperDocument2 pagesSolomon Islands Position PaperAJ Ammons0% (1)
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- Winkler, W & Pelosi - 2022 - Understanding Breast CancerDocument76 pagesWinkler, W & Pelosi - 2022 - Understanding Breast CancerJordan KopongNo ratings yet
- Surfactant FloodingDocument13 pagesSurfactant FloodingVlassis SarantinosNo ratings yet
- Charity and Gift Giving (Choi)Document28 pagesCharity and Gift Giving (Choi)ROGEL SONo ratings yet
- Transport ProcessesDocument81 pagesTransport ProcessesKukre BertNo ratings yet
- Topic 5 AC To AC ConverterDocument53 pagesTopic 5 AC To AC ConverterNorain ZakariaNo ratings yet
- PCAR Contractors ManualDocument219 pagesPCAR Contractors ManualDefendAChildNo ratings yet
- Chlorine Dosing PumpDocument24 pagesChlorine Dosing PumpByron HisseyNo ratings yet
- Social and Self Control TheoryDocument2 pagesSocial and Self Control TheoryKarl Amiel EspirituNo ratings yet
- Silicic Acid Agro Technology: DescriptionDocument1 pageSilicic Acid Agro Technology: DescriptionKeniel BarrettNo ratings yet
- Funding Proposal: WebsiteDocument8 pagesFunding Proposal: Websitemajiamal99No ratings yet
- (II) Misadventure Is Mischance, Accident or Disaster. It Is of Three TypesDocument3 pages(II) Misadventure Is Mischance, Accident or Disaster. It Is of Three TypesSandeep BansalNo ratings yet
- Suzumar Boat Engine PackagesDocument7 pagesSuzumar Boat Engine PackagesmarkoNo ratings yet
- Recruitment MSCDocument40 pagesRecruitment MSCViji MNo ratings yet
- Company Profile Kalgen Innolab Innobiogram - 2022Document12 pagesCompany Profile Kalgen Innolab Innobiogram - 2022asmadi arrumNo ratings yet
- Unfuck Your Anilingus - How To Keep Your Oral Butt Sex Classy - Faith G Harper - 2022 - Microcosm Publishing - 9781648411618 - Anna's ArchiveDocument28 pagesUnfuck Your Anilingus - How To Keep Your Oral Butt Sex Classy - Faith G Harper - 2022 - Microcosm Publishing - 9781648411618 - Anna's Archiverhy4kjgqx6No ratings yet
- Petroleum Refining Notes 1Document5 pagesPetroleum Refining Notes 1api-304149645No ratings yet
- Coevolution of Hosts and ParasitesDocument5 pagesCoevolution of Hosts and ParasitesAshok KoyiNo ratings yet
- Divergent Plate BoundaryDocument4 pagesDivergent Plate BoundaryGreg ManNo ratings yet