Download as pdf or txt
You might also like
- Job Hazard Analysis (HDD)Document7 pagesJob Hazard Analysis (HDD)jay R100% (1)
- AP Medical Council Renewal ApplicationDocument2 pagesAP Medical Council Renewal Applicationdrvaas73% (11)
- Application Form For Contract Medical Officer (Non - Citizens) PDFDocument19 pagesApplication Form For Contract Medical Officer (Non - Citizens) PDFHafiz IbrahimNo ratings yet
- Maturity Claim (Form No.3825)Document3 pagesMaturity Claim (Form No.3825)Ranjith KandimallaNo ratings yet
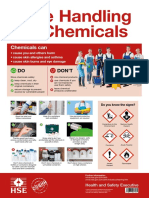
- Chemicals Can: Safe Handling of ChemicalsDocument1 pageChemicals Can: Safe Handling of ChemicalsQamar KhanNo ratings yet
- Eyesight Test Form and Certificate: Certifying Medical Practitioner / OphthalmologistDocument1 pageEyesight Test Form and Certificate: Certifying Medical Practitioner / OphthalmologistTatenda UyaNo ratings yet
- Provisional Reg FormDocument2 pagesProvisional Reg FormSamson MufayaNo ratings yet
- General Circular For MD October, 2022Document18 pagesGeneral Circular For MD October, 2022akhilNo ratings yet
- Application Form For RN 1Document13 pagesApplication Form For RN 1Ken Ehichoya UgieNo ratings yet
- BHPC Application Form For Penn Updated Jan 2019Document6 pagesBHPC Application Form For Penn Updated Jan 2019sosomiso234No ratings yet
- Direct Recruitment Form - NewDocument6 pagesDirect Recruitment Form - NewsunilhasnuNo ratings yet
- Application Form - Student IndexingDocument2 pagesApplication Form - Student IndexingBeenzu Briella SiamalubeNo ratings yet
- Advt No-01-2019 7feb2019Document5 pagesAdvt No-01-2019 7feb2019Swapnaneel BaishyaNo ratings yet
- Updating ProformaDocument2 pagesUpdating ProformaJme RNo ratings yet
- ClaimApplicalionFormGS EDocument4 pagesClaimApplicalionFormGS EeuacreationsNo ratings yet
- Sri Lanka Medical Council: Coloured Photograph Photo Size 3.5 X 4. 5 CMDocument3 pagesSri Lanka Medical Council: Coloured Photograph Photo Size 3.5 X 4. 5 CMmani50No ratings yet
- Ipmt FormDocument5 pagesIpmt FormTarinder SinghNo ratings yet
- SLMC Regitration 2020Document3 pagesSLMC Regitration 2020vihari.shashiNo ratings yet
- Application For Empanelment of Valuer Syndicate BankDocument3 pagesApplication For Empanelment of Valuer Syndicate BankNishkam GuptaNo ratings yet
- RMHF 4 FormDocument5 pagesRMHF 4 FormSimul MondalNo ratings yet
- Salary in Advance FormDocument1 pageSalary in Advance FormchelamercykorirNo ratings yet
- MOrth Application Form May 2021Document3 pagesMOrth Application Form May 2021MINA GERGISNo ratings yet
- Form 1Document1 pageForm 1Akash TamuliNo ratings yet
- Suza ApplicationDocument4 pagesSuza ApplicationRashid BumarwaNo ratings yet
- Po/Mt Cwe-V Documents Required For Completion of Pre-Employment FormalitiesDocument3 pagesPo/Mt Cwe-V Documents Required For Completion of Pre-Employment Formalitiesamanchandra21No ratings yet
- Admission Details of BSC 2024Document4 pagesAdmission Details of BSC 2024kallukhan7323No ratings yet
- Form4 Provisional MMCDocument3 pagesForm4 Provisional MMCminci sensei100% (2)
- NOC and Medical Certificate ProformaDocument2 pagesNOC and Medical Certificate ProformaKartikNo ratings yet
- Emmes Scholarship Application Form, 2018-19: Master of Public Health (MPH) ProgramDocument2 pagesEmmes Scholarship Application Form, 2018-19: Master of Public Health (MPH) ProgramSaurabh SumanNo ratings yet
- GA Claim Form PDF (6) (1) (2) (1) (2) - 1Document1 pageGA Claim Form PDF (6) (1) (2) (1) (2) - 1blessed talbot medical centre ltdNo ratings yet
- Provisional RegistrationDocument9 pagesProvisional RegistrationabuprettyNo ratings yet
- Section - 3 Medical Fitness CertificateDocument1 pageSection - 3 Medical Fitness CertificateireneNo ratings yet
- List of Documents Prescribed by The University To Be Submitted at The Respective Training Center(s)Document4 pagesList of Documents Prescribed by The University To Be Submitted at The Respective Training Center(s)raval anil.uNo ratings yet
- FORM 18 With Instructions and Additional FormDocument4 pagesFORM 18 With Instructions and Additional Formsathiya81No ratings yet
- Kempegowda Institute of Medical SciencesDocument3 pagesKempegowda Institute of Medical SciencesalishNo ratings yet
- Membership Form For New Members: PF NoDocument4 pagesMembership Form For New Members: PF NoAbhilash BaranwalNo ratings yet
- Bond Cum Agreement MBBSDocument6 pagesBond Cum Agreement MBBSﻓﺮﻳﺢ ﺑﻨﺖ ﺁﺯﺍﺩNo ratings yet
- Andhra Pradesh Medical Council: See Section-15C of A.P Medical Practitioners Registration (Amendment) Act, 2013Document3 pagesAndhra Pradesh Medical Council: See Section-15C of A.P Medical Practitioners Registration (Amendment) Act, 2013kirank_11No ratings yet
- CGHSDocument3 pagesCGHSVishal KumarNo ratings yet
- SBI FASTag Full KYC Application FormDocument4 pagesSBI FASTag Full KYC Application FormYogant BhureNo ratings yet
- Detailed Instructions For Candidates Attending Personality Test Board in Respect of Combined Medical Services Examination, 2017Document2 pagesDetailed Instructions For Candidates Attending Personality Test Board in Respect of Combined Medical Services Examination, 2017Diwakesh C BNo ratings yet
- ASC Centre (South) 2 ATC Form OldDocument5 pagesASC Centre (South) 2 ATC Form Oldamit vermaNo ratings yet
- Kenya KCA CollegeDocument3 pagesKenya KCA CollegePulsmade MalawiNo ratings yet
- Application For Student Registration: Institute of Certified Management Accountants of Sri LankaDocument4 pagesApplication For Student Registration: Institute of Certified Management Accountants of Sri LankaKinGsly Warshamana100% (1)
- Application Form 2020 2021Document3 pagesApplication Form 2020 2021babu rsNo ratings yet
- Application For Cghs CardDocument3 pagesApplication For Cghs CardManpreetNo ratings yet
- Membership Form Latest 12.01.2023Document2 pagesMembership Form Latest 12.01.2023Shrutik AshiyaniNo ratings yet
- Letter of Offer: Recruitment in Clerical Cadre Registration NoDocument6 pagesLetter of Offer: Recruitment in Clerical Cadre Registration NoDevdutt MishraNo ratings yet
- Fresher Application FormDocument2 pagesFresher Application FormveersinglaNo ratings yet
- Format of CertificatesDocument12 pagesFormat of CertificatesrowdysinghNo ratings yet
- Notification For Selection of Managing Director Chief Executive OfficerDocument7 pagesNotification For Selection of Managing Director Chief Executive OfficerKrishna MyakalaNo ratings yet
- SBI FASTag Application Form - IndividualDocument4 pagesSBI FASTag Application Form - Individualpp ddNo ratings yet
- SBI FASTag Application Form - Individual - FULL-KYC-minDocument3 pagesSBI FASTag Application Form - Individual - FULL-KYC-minSaravanan SNo ratings yet
- FASTag CAF Individual Full KYCDocument8 pagesFASTag CAF Individual Full KYCpgsbeNo ratings yet
- Eligibility Application Form Migration 100122Document4 pagesEligibility Application Form Migration 100122swati agarwalNo ratings yet
- Application For New CGHS CardDocument2 pagesApplication For New CGHS CardrandomNo ratings yet
- Youth Enterprise Revolving Fund Company Directors Form: (Finance and Audit Act No.18 of 1967, & YERF Regulations, 2009)Document2 pagesYouth Enterprise Revolving Fund Company Directors Form: (Finance and Audit Act No.18 of 1967, & YERF Regulations, 2009)OCTANE PLANT ENGINEERINGNo ratings yet
- Exam 24470Document3 pagesExam 24470JAGJIT PRASAD SINGHNo ratings yet
- Registration FormDocument2 pagesRegistration FormMtech2019 StructuresNo ratings yet
- Msacco Consent DocumementsDocument3 pagesMsacco Consent DocumementsIvan ManogaNo ratings yet
- ClaimApplicalionFormGS EDocument5 pagesClaimApplicalionFormGS ERavi JanakaNo ratings yet
- Indian VisaDocument1 pageIndian Visaroem036430No ratings yet
- Joerns - HoyerSlingChart GRUA DE PACIENTES JOERNS HOYER CHLA2Document7 pagesJoerns - HoyerSlingChart GRUA DE PACIENTES JOERNS HOYER CHLA2pabloNo ratings yet
- Checklist Exam of EarDocument4 pagesChecklist Exam of EarCes Melisse DNo ratings yet
- JURNALDocument10 pagesJURNALRendi KurniawanNo ratings yet
- Method Statement For Panel InstallationDocument8 pagesMethod Statement For Panel InstallationveksNo ratings yet
- Ceilcote-380 Primer - Vinyl EsterDocument4 pagesCeilcote-380 Primer - Vinyl EsterEspie SualogNo ratings yet
- B. Estudiantes. Listening Test - Health CentersDocument9 pagesB. Estudiantes. Listening Test - Health CentersAna Maria CuartasNo ratings yet
- Job Safety Analysis Sheet: Mechanical ExcavationDocument1 pageJob Safety Analysis Sheet: Mechanical ExcavationjoshuaNo ratings yet
- Indian Case Study Flowrence Dental ClinicDocument7 pagesIndian Case Study Flowrence Dental ClinicMalavika LovelNo ratings yet
- Influencer Email FlowDocument4 pagesInfluencer Email Flowapi-438812931No ratings yet
- Lpe2301 Academic Interaction and Presentation SCL Worksheet 1 Week 2 (Opening A Discussion and Phonetic Symbols)Document3 pagesLpe2301 Academic Interaction and Presentation SCL Worksheet 1 Week 2 (Opening A Discussion and Phonetic Symbols)ZHENG MENGJIENo ratings yet
- Bonded Retainer Informed ConsentDocument1 pageBonded Retainer Informed ConsentHusam AlsamiaNo ratings yet
- Pengaruh Pengetahuan Dan Motivasi Kerja Dokter Spesialis Terhadap Pengisian Rekam Medis Rawat Inap Di Rumah Sakit Santa Elisabeth MedanDocument9 pagesPengaruh Pengetahuan Dan Motivasi Kerja Dokter Spesialis Terhadap Pengisian Rekam Medis Rawat Inap Di Rumah Sakit Santa Elisabeth MedanAbdul HadiNo ratings yet
- Table: 5.1-Overcoming Bias in Language Gender Bias Examples Unacceptable PreferableDocument4 pagesTable: 5.1-Overcoming Bias in Language Gender Bias Examples Unacceptable PreferableTasnim JuhiNo ratings yet
- BDC Audit SGLGBDocument77 pagesBDC Audit SGLGBDILG LUPONNo ratings yet
- SR DenasriDocument284 pagesSR DenasriDjie GuerrNo ratings yet
- The Gold Legged Frog by Khamsing Srinawk PaperDocument2 pagesThe Gold Legged Frog by Khamsing Srinawk PaperDaniyalChatthaNo ratings yet
- H2 BlockersDocument3 pagesH2 BlockersDhayu Mart Hindrasyah PandiaNo ratings yet
- NEC Art 500Document2 pagesNEC Art 500Kranthi Kumar0% (1)
- Plan of ActivitiesDocument3 pagesPlan of ActivitiesLiiza G-GsprNo ratings yet
- Single Pages - alliANCE Membership Directory.6.24.21.PRINTABLEDocument16 pagesSingle Pages - alliANCE Membership Directory.6.24.21.PRINTABLELeslie HammondNo ratings yet
- Mental Health Life HacksDocument13 pagesMental Health Life HacksmoodyredheadNo ratings yet
- Certification Tolega NorteDocument5 pagesCertification Tolega NorteGerome Bautista VInluanNo ratings yet
- Code Registration Number Strength Presentation Form AgentDocument30 pagesCode Registration Number Strength Presentation Form AgentA GhNo ratings yet
- Jobs Safety Analysis (JSA) : JOB/ACTIVITY NAME: Scaffolding Erection, Dismantling Work, Work at Height, Welding WorkDocument4 pagesJobs Safety Analysis (JSA) : JOB/ACTIVITY NAME: Scaffolding Erection, Dismantling Work, Work at Height, Welding Workuttam mishraNo ratings yet
- Ceir Form-Bikal BHS 2021Document2 pagesCeir Form-Bikal BHS 2021Mark Jake RodriguezNo ratings yet
- Advisory: Clarification On Konsulta Providers and Its ImplementationDocument1 pageAdvisory: Clarification On Konsulta Providers and Its ImplementationMox LexNo ratings yet
- Presentasi Hsse Performance 2020 To PepDocument14 pagesPresentasi Hsse Performance 2020 To PepArief HutasuhutNo ratings yet