Professional Documents
Culture Documents
The Anterolateral Ligament of The Knee: MRI Appearance, Association With The Segond Fracture, and Historical Perspective
The Anterolateral Ligament of The Knee: MRI Appearance, Association With The Segond Fracture, and Historical Perspective
Uploaded by
Saifuddin HaswareOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
The Anterolateral Ligament of The Knee: MRI Appearance, Association With The Segond Fracture, and Historical Perspective
The Anterolateral Ligament of The Knee: MRI Appearance, Association With The Segond Fracture, and Historical Perspective
Uploaded by
Saifuddin HaswareCopyright:
Available Formats
Musculoskeletal Imaging • Original Research
Porrino, Jr. et al.
MRI of Anterolateral Ligament of the Knee
Musculoskeletal Imaging
Original Research
The Anterolateral Ligament of the
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
Knee: MRI Appearance, Association
With the Segond Fracture, and
Historical Perspective
Jack Porrino, Jr.1 OBJECTIVE. A recent publication has drawn attention to the anterolateral ligament, a
Ezekiel Maloney structure of the knee with which most radiologists are unfamiliar. We evaluate this structure
Michael Richardson on MRI; clarify its origin, insertion, meniscal relationship, and morphologic appearance; and
Hyojeong Mulcahy identify its relationship with the Segond fracture.
Alice Ha MATERIALS AND METHODS. A total of 53 routine knee MRI studies interpreted
as normal were reviewed to characterize the anterolateral ligament. A further 20 knee MRI
Felix S. Chew
studies with a Segond fracture were assessed to determine a relationship between the fracture
Porrino J Jr, Richardson M, Mulcahy H, and the anterolateral ligament.
Maloney E, Ha A, Chew FS RESULTS. In all 53 cases, a structure was present along the lateral knee connecting the
distal femur to the proximal tibia, with meniscofemoral and meniscotibial components. This
structure was somewhat ill defined and sheetlike, inseparable from the adjacent fibular col-
lateral ligament proximally and iliotibial band distally. Aside from one case limited by ana-
tomic distortion, all cases with a Segond fracture exhibited attachment of this structure to the
fracture fragment (19/20 cases).
CONCLUSION. An ill-defined sheetlike structure along the lateral knee exists attach-
ing the distal femur, body of lateral meniscus, and proximal tibia. This structure has been ref-
erenced in the literature dating back to Paul Segond’s original description of the Segond frac-
ture in 1879. The structure is identifiable on MRI and appears to be attached to the Segond
fracture fragment. For the radiologist, it may be best to forgo an attempt to separate this struc-
ture into discrete divisions, such as the anterolateral ligament, because these individual com-
ponents are inseparable on routine MRI.
A
natomy of the lateral aspect of Claes et al. [3] think that Dr. Paul Segond
the knee is complex, with numer- described this ligament in 1879 during his
ous structures providing stabili- initial description of the Segond avulsion
ty. Structures such as the iliotibi- fracture. In this description, the Segond frac-
al band, fibular collateral ligament, and ture occurs at the anterolateral proximal tib-
Keywords: anterolateral ligament, anterior oblique band biceps femoris tendon are readily apparent ia as a result of forced internal rotation at the
of fibular collateral ligament, capsuloosseous layer of on MRI and are easy to identify. Unlike knee. Segond described a “pearly, resistant,
iliotibial band, lateral capsular ligament, Segond fracture these more common structures that stabilize fibrous band which invariably showed ex-
DOI:10.2214/AJR.14.12693
the lateral knee, the anterolateral ligament treme amounts of tension during forced in-
does not appear in many common radiology ternal rotation (of the knee)” at the location
Received February 8, 2014; accepted after revision and gross anatomy texts [1, 2]. of the fracture [3].
May 9, 2014. Recently, there has been much excitement Since the Segond study, there have been
1
about the publication of an article by Claes numerous references to a structure along the
All authors: Department of Radiology, University of
Washington, Box 354755, 4245 Roosevelt Way NE,
et al. [3], in which they provided a detailed lateral aspect of the knee connecting the dis-
Seattle, WA 98105. Address correspondence to anatomic description of an anterolateral lig- tal femur to the tibia, many with claims that
J. Porrino, Jr. (jporrino@uw.edu). ament (Fig. 1). Although Claes et al. do not this structure is responsible for the Segond
claim that this ligament is a new discovery, fracture. Unfortunately, these articles show
AJR 2015; 204:367–373 they do suggest that it is nearly always appar- considerable variability in nomenclature and
0361–803X/15/2042–367
ent on gross anatomic dissection and likely morphologic description.
plays an important role in the pathophysio- The purpose of our study was to identi-
© American Roentgen Ray Society logy of the Segond fracture. fy the anterolateral ligament on MRI of the
AJR:204, February 2015 367
Porrino, Jr. et al.
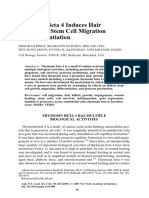
Fig. 1—Drawings modeled after
diagrammatic depiction of anterolateral
ligament (ALL) by Claes et al. [3].
(Adapted with permission from John
Wiley and Sons)
A and B, Axial (A) and lateral (B) views
of knee are shown. ALL is denoted in
relationship to surrounding structures,
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
including popliteus tendon (PT), fibular
or lateral collateral ligament (LCL),
iliotibial band (ITB), and Gerdy tubercle
(GT). Notably, multiple (n = 3) tissue
layers are depicted on axial view, from
superficial to deep, partly composed
of iliotibial band, lateral patellar
retinaculum anteriorly, and thin lateral
capsule (arrows, A) just anterior to ALL.
A B
knee; to clarify its proximal origin, distal in- ical Center using magnets with 3-T field strength which contrast agent was present, despite the PACS
sertion, meniscal relationship, and morpho- (two Ingenia magnets and one Achieva magnet, designation as an unenhanced examination, were
logic appearance; and to identify the rela- all from Philips Healthcare) between December discarded. This resulted in a total of 76 remaining
tionship between the anterolateral ligament 2011 and November 12, 2013. Images from these cases. Studies in which bone marrow abnormalities
and the Segond fracture fragment. magnets were chosen because of their superior were noted, such as small enchondroma or bone in-
field strength and spatial resolution. Reports from farct, were included for review because these find-
Materials and Methods these studies were reviewed, and only those stud- ings have no impact on the integrity of the sur-
This study was approved by the investigation- ies in which the final impression was normal, or the rounding ligamentous structures. Patients younger
al review board at the University of Washington. abnormality was limited to minor hyaline articu- than 18 years (n = 23) were excluded. As a result,
lar cartilage abnormalities or minor tendinosis of a total of 53 unenhanced normal knee MRI stud-
Healthy Subjects the extensor apparatus, were included for interpre- ies were reviewed to identify the anterolateral liga-
A total of 395 routine knee MRI studies were tation. In addition, those studies subject to artifact ment. The magnets used and the pulse sequences
performed at the University of Washington Med- limiting the quality of the examination, or cases in evaluated are listed in Table 1.
Two fellowship-trained musculoskeletal radi-
TABLE 1: MRI Magnets and Pulse Sequences Used to Characterize the
ologists jointly interpreted each study and tabulat-
Anterolateral Ligament and Assess for an Association of the
ed their consensus opinion regarding the following
Anterolateral Ligament With the Segond Fracture
questions: First, with regard to the appearance of
Assessment, Magnets Used Pulse Sequences Evaluated the proximal aspect of the ligament, is there blend-
Characterization of the anterolateral ligament ing with the fibular collateral ligament at the prox-
imal femoral origin, as described in the study by
3-T Ingenia (Philips Healthcare) Axial T2-weighted spectral attenuated inversion
recovery Claes et al. [3], and is the structure easily separable
from the structure referred to by Claes et al. as the
3-T Achieva (Philips Healthcare) Coronal proton density spectral attenuated
lateral capsule? Second, are there discrete menisco-
inversion recovery
femoral and meniscotibial attachments, as Claes et
Evaluation for association of the anterolateral al. suggest, along the midportion of the structure?
ligament with the Segond fracture
Third, with regard to characterization of the distal
3-T Achieva (Philips Healthcare) Axial T2-weighted fat suppressed tibial insertion, is the tibial attachment cordlike, or
1.5-T Achieva (Philips Healthcare) Axial T2-weighted spectral attenuated inversion instead fanned as Claes et al. describe, and can the
recovery distal attachment be discriminated from the poste-
3-T Signa HDxt (GE Healthcare) Coronal T1-weighted rior fibers of the iliotibial band?
1.5-T Signa Excite (GE Healthcare) Coronal STIR
Subjects With Segond Fractures
Coronal proton density fat suppressed
zVision software (version 1.4.80, Clario) was
Coronal proton density spectral attenuated used to search the University of Washington
inversion recovery
PACS for routine knee MRI examinations per-
368 AJR:204, February 2015
MRI of Anterolateral Ligament of the Knee
formed within the University of Washington sys- A total of 20 MRI studies with a readi- fibular collateral ligament. The anterolater-
tem between November 1, 2005, and November ly apparent Segond fracture were evaluated al ligament has a strong connection with the
12, 2013, that included the word “Segond” in the to determine an association of the anterolat- periphery of the body of the lateral menis-
finalized report. A total of 48 studies performed eral ligament with this avulsion injury. This cus by way of its meniscofemoral and menis-
on a combination of 1.5- and 3-T magnets were included 17 men and three women, with 12 cotibial components. Distally, the ligament
identified. Each study was reviewed to confirm right knees and eight left knees. In 19 of the inserts midway between the Gerdy tuber-
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
the presence of an MRI-apparent Segond fracture, 20 cases, there was clear insertion of the tib- cle and the fibular head, with distal flaring
and those without a discernible Segond fracture ial component of the anterolateral ligament clearly apparent (Fig. 1). There is no connec-
fragment on MRI (n = 14) were excluded. In ad- onto the Segond fracture (Figs. 4 and 5). In tion of the ligament with the lateral capsule
dition, patients younger than 18 years (n = 1), pa- the lone remaining case, anatomic distortion proximally or with the iliotibial band distal-
tients with an incomplete examination (n = 1), and limited assessment of a ligamentous attach- ly. The authors suggested, on the basis of the
those with suboptimal imaging such as that seen ment to the fragment. close association of the femoral origins of
with hardware or patient motion (n = 12) were ex- the fibular collateral ligament and anterolat-
cluded from the study. This resulted in a total of Discussion eral ligament, that the fibular collateral lig-
20 unenhanced MRI studies of Segond fracture in In the article by Claes et al. [3], the antero- ament and anterolateral ligament collective-
this arm of our study (Table 1). These studies were lateral ligament is described as arising from ly be referred to as one structure, the lateral
reviewed during the same session by the same two the lateral femoral epicondyle, proximal and collateral ligament complex. On the basis of
fellowship-trained musculoskeletal radiologists to posterior to the popliteus tendon, and with the anatomic location of the anterolateral lig-
establish a relationship between the anterolateral posterior fibers blending with the proximal ament, the authors suggested that the struc-
ligament and the Segond fracture fragment. Final
results were tabulated.
Results
A total of 53 normal knee MRI studies
were evaluated (35 women and 18 men; 29
right and 24 left knees). Patient age ranged
from 18 to 59 years old. In all 53 cases, a
structure was present along the lateral as-
pect of the knee that connects the distal fe-
mur with the proximal tibia. We were able to
visualize this structure throughout its entire
course, in both the axial and coronal plane.
Proximally (at the level of the distal fe-
mur), this structure is inseparable from the
adjacent fibular collateral ligament at their
femoral attachment site. In fact, a discrete A
proximal origin of the ligament is difficult
to discern. Instead, just below the epicondy-
lar origin of the fibular collateral ligament,
a long (in anteroposterior dimension) but
thin and somewhat ill-defined meniscofem-
oral attachment is present that runs deep to
the iliotibial band and anterior to the fibu-
lar collateral ligament. There is no reliable
division of this structure at this level to al-
low separation of an anterolateral ligament
from an adjacent and more anterior lateral
capsule. As this structure continues distally,
there is a more distinct meniscotibial com-
ponent that blends in a broad-based fashion
onto the proximal tibia, below the level of the
tibial plateau and midway between the Gerdy B
tubercle and the fibular head. This distal in- Fig. 2—29-year-old man. T2-weighted spectral attenuated inversion recovery MR images of knee (sequentially
sertion is inseparable anteriorly from the through knee, from proximal to distal) are shown. Solid white lines represent corresponding slice levels
posterior fibers of the iliotibial band. The between axial and coronal images.
structure’s intimate relationship with the A, Axial (left) and coronal (right) images show femoral origin of fibular collateral ligament (FCL). Anterolateral
ligament (ALL) is not yet appreciated at this level. ITB = iliotibial band.
body of the lateral meniscus is best appreci- B, Axial (left) and coronal (right) images show ALL arising anterior to FCL, deep to ITB, and proximal to lateral
ated in the coronal plane (Figs. 2 and 3). meniscus. Coronal image denotes meniscofemoral component, merging with body of lateral meniscus.
(Fig. 2 continues on next page)
AJR:204, February 2015 369
Porrino, Jr. et al.
eral capsular ligament). Others include a
description of an anterior oblique band of
the fibular collateral ligament. In addition,
the relationship of the iliotibial band with
this structure is quite confusing on the ba-
sis of prior reports. A chronologic and sys-
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
tematic review of the literature in regard to
this structure, as well as that of the Segond
fracture, shows these inconsistencies.
Literature Review of the
Anterolateral Ligament
Lateral Capsular Ligament
In a two-part landmark study performed
in 1976 pertaining to the classification of
knee ligament instabilities, Hughston et al.
C [4, 5] divided the lateral compartment liga-
ments of the knee into three anatomic divi-
sions. The middle third, composed of the il-
iotibial band and deep capsular ligaments,
extends posterior to the level of the fibular
collateral ligament. Within this middle di-
vision, the lateral capsular ligament attach-
es proximally to the lateral epicondyle of the
femur and distally to the tibial joint margin,
with attachments to the meniscus divided
into meniscofemoral and meniscotibial por-
tions. Those articles provided the blueprint
for the detailed anatomy that comprises the
lateral aspect of the knee used by many au-
thors thereafter [4, 5].
In a 2000 review of the MRI appear-
D ance of structures that comprise the post-
Fig. 2 (continued)—29-year-old man. T2-weighted spectral attenuated inversion recovery MR images of knee erolateral knee, LaPrade et al. [6] described
(sequentially through knee, from proximal to distal) are shown. Solid white lines represent corresponding slice the mid third lateral capsular ligament as a
levels between axial and coronal images. thickening of the lateral capsule of the knee,
C, Axial (left) and coronal (right) images show meniscotibial component of ALL just distal to body of lateral
meniscus on axial slice, whereas both meniscofemoral and meniscotibial components are denoted on coronal
attaching to the femur in the region of the
slice, merging with body of lateral meniscus. lateral epicondyle, with capsular attach-
D, Axial (left) and coronal (right) images show ALL at tibial insertion site, midway between Gerdy tubercle and ments to the lateral meniscus and insertion
fibular head. Coronal image highlights meniscotibial component. onto the tibia posterior to the Gerdy tubercle
ture may be an important stabilizer for inter- discrepancies may well be the result of lim- and anterior to the popliteal hiatus. They di-
nal rotation and that avulsion may account itations in the spatial resolution of MRI vided this structure into meniscotibial and
for the Segond fracture [3]. when compared with that of direct gross an- meniscofemoral ligament subcomponents.
We found the MRI appearance of the an- atomic dissection. This anatomic description is in accordance
terolateral ligament to be similar to that Nevertheless, there is clearly a lateral with the studies by Hughston et al. [4, 5].
described by Claes et al. [3], although we structure readily apparent on MRI connect- Bone avulsion of the meniscotibial ligament
found certain exceptions. Most discordant, ing the distal femur, the body of the later- portion of the mid third lateral capsular liga-
there was no reliable visualized plane sepa- al meniscus, and the proximal tibia, exhib- ment is termed a Segond fracture according
rating an anterolateral ligament and an im- iting a strong association with the Segond to these authors [6].
mediately adjacent lateral capsule, as Claes fracture. Much of the confusion stems from Haims et al. [7] reviewed MRI anatomy
et al. described. This results in a single thin the lack of standardized nomenclature and of the lateral knee in 2003. In that study, the
and somewhat ill-defined structure, as op- the seemingly overwhelming tendency mid third lateral capsular ligament is depict-
posed to a discrete cordlike structure (an- within the literature to divide this structure ed and described. This ligament runs verti-
terolateral ligament) and adjacent thin cap- into multiple individual fascicles. Some au- cally from the distal femur to the mid third
sular structure (lateral capsule). In addition, thors reference a single structure respon- lateral tibia on both diagrams and per their
at the distal tibial insertion, there is no reli- sible for attachment of the lateral distal description. However, the ligament lacks an
able plane separating this structure from the femur with the adjacent tibia (i.e., the lat- obvious femoral insertion on the provided
posterior fibers of the iliotibial band. These eral capsular ligament or middle-third lat- imaging. In their discussion, bony avulsion
370 AJR:204, February 2015
MRI of Anterolateral Ligament of the Knee
of this structure is responsible for the Segond
fracture [7].
In an anatomic and biomechanical re-
view of the posterolateral corner of the knee,
Moorman et al. [8] in 2005 described the
mid third lateral capsular ligament as the
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
portion of the capsule that attaches to the fe-
mur and courses down to the tibia, at the site
of the Segond avulsion fracture [8].
Anterior Oblique Band of the Fibular
Collateral Ligament
In 1987, Irvine et al. [9] divided the fibu-
lar collateral ligament into two components
A B
while examining the Segond fracture. The
fibular collateral ligament was divided into
a straight band that courses from the distal
femur to the fibular head, as well as an ante-
rior oblique band that inserts onto the lateral
tibial rim. In that study, results indicated that
the Segond fracture may be avulsed by the
anterior oblique band. [9]
In 2001, Campos et al. [10] provided a
detailed review of the pathogenesis of the
Segond fracture with both gross anatomic
dissection and MRI. A description of the an-
terior oblique band of the fibular collateral
ligament was provided—a firm band of tis-
sue arising from the fibular collateral liga- C D
ment in an oblique fashion, inserting at the Fig. 3—Line drawings derived from axial and coronal MR images of knee. (Drawings by Maloney E)
lateral midportion of the tibia and blending A, Drawing shows anterolateral ligament (ALL) arising anterior and immediately adjacent to fibular collateral
with the posterior fibers of the iliotibial tract. ligament (FCL), deep to iliotibial band (ITB), and proximal to body of lateral meniscus. This structure is thin,
without clear demarcation from immediately adjacent and anterior lateral joint capsule on MRI.
The lateral capsular ligament was described B, Drawing shows ALL at level of body of lateral meniscus.
as a separate structure—a delicate thicken- C, ALL is inserting onto tibia, midway between Gerdy tubercle and fibular head, inseparable from adjacent
ing of the lateral capsule at its midpoint, with fibers of ITB.
D, Coronal representation of ALL shows meniscotibial and meniscofemoral components of structure.
a vertical orientation. The iliotibial tract, an-
terior oblique band, and lateral capsular liga- tified on MRI in a coronal oblique plane only Anterolateral Ligament
ment exhibited attachments to each other, as when marked preemptively with gadopen- In a description of anatomy of the iliopatel-
well as attachment to the lateral tibia. The tetate dimeglumine–filled tubes. There was lar band and iliotibial tract in 1986, Terry et
anterior oblique band was identified on MRI a frequent attachment of the iliotibial tract al. [11] referred to the capsuloosseous layer of
in the axial plane in all six cadavers studied. and the anterior oblique band to the avulsed the iliotibial tract as the anterolateral ligament
The lateral capsular ligament could be iden- Segond fracture fragment [10]. because of this structure’s contribution to an-
Fig. 4—28-year-old man with Segond
fracture after motorcycle crash.
A, In coronal proton density–weighted
fat-suppressed image, meniscotibial
component of anterolateral ligament
(ALL) can be seen attaching to Segond
fracture fragment. ITB = iliotibial band.
B, Corresponding frontal radiograph
shows nearly imperceptible displaced
fracture fragment (arrow) adjacent to
lateral tibial plateau.
A B
AJR:204, February 2015 371
Porrino, Jr. et al.
terolateral stability of the knee. In this de-
scription, the capsuloosseous layer is formed
proximally by a coalescence of fascia overly-
ing the plantaris and lateral gastrocnemius to
which it is intimately applied. Furthermore, at
the lateral gastrocnemius, it becomes a trian-
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
gular ligament attaching posterior distally to
the fibula and anterior distally to the lateral
tibial tuberosity. The distal tibial insertion is
specifically described as being just posterior
to the Gerdy tubercle, on the lateral tibial tu-
berosity. It should be noted that in that study,
there is specific reference to an additional lat-
eral structure about the knee referred to as the
mid third capsular ligament. [11]
In a detailed anatomic study of the iliotib-
ial tract by Vieira et al. in 2007 [12], the au-
thors referenced the original description by A B
Terry et al. [11] of the anterolateral ligament.
They described this portion of the iliotibial
tract as having a well-defined ligamentous
appearance, arising from the lateral supra-
epicondylar region of the femur, bordering
the lateral edge of the lateral epicondyle, and
inserting laterally to the Gerdy tubercle of
the proximal tibia [12].
In 2012, in an anatomic and histologic
study of those undergoing total knee arthro-
plasty and in cadaveric dissections, Vincent
et al. [13] described a structure that links the
lateral femoral condyle, lateral meniscus, and
lateral tibial plateau and referred to it as the
anterolateral ligament. This structure arose
from the lateral femoral condyle in the major-
ity of cases, except for a case originating from
the popliteus tendon just before its insertion. C D
In each case, the structure was closely relat- Fig. 5—19-year-old woman who experienced direct blow to knee while playing soccer
ed to the lateral meniscus and always insert- A–C, Sequential coronal STIR images of knee show Segond fracture and its relationship with anterolateral
ed onto the proximal anterolateral tibia. His- ligament (ALL), iliotibial band (ITB), and fibular collateral ligament (FCL). First image (A) shows knee at level of
ITB. In second image (B), just posterior to first image (A), meniscotibial component of ALL is seen attaching to
tologically, this structure exhibited the same Segond fracture fragment. Third image (C), just posterior to second image (B), shows FCL.
type of collagen orientation as that seen with D, Corresponding frontal radiograph shows Segond fracture (arrow).
tendons and ligaments and reflected fibrous
tissue distinct from the lateral capsule. Vin- association with tears of the anterior cruci- nal description by Hughston et al. in 1976 [4,
cent et al. stated that this structure is synony- ate ligament and menisci, as well as resultant 5]. Woods et al. provided a brief description
mous with the one described by Terry et al. anterolateral rotary instability. The avulsed of their operative approach to repair. They re-
[11] and later Vieira et al. [12] (capsuloosse- fragment is often readily apparent on an an- ferred to the radiographic finding as the lat-
ous layer of the iliotibial tract), LaPrade et al. teroposterior view of the knee, although the eral capsular sign as a result of the aforemen-
[6] (mid-third lateral capsular ligament), and fracture fragment is far more difficult to tioned anatomic description [18].
Campos et al. [10] (lateral capsular ligament). identify on MRI [10, 14–18]. Dietz et al. [14] in 1986 performed a ra-
In 1979, Woods et al. [18] suggested that diographic review of the Segond tibial con-
Literature Review of the the Segond fracture reflects a fracture frag- dyle fracture. The fracture was differentiated
Segond Fracture ment superior and posterior to the Gerdy tu- from avulsion of the Gerdy tubercle. The au-
The Segond fracture is a cortical avul- bercle, related to avulsion of the menisco- thors explained the Segond fracture as being
sion fracture of the proximal tibia, located tibial portion of the middle one-third of the related to avulsion of the lateral capsular liga-
just below the level of the lateral plateau and lateral capsular ligament. The middle one- ment, with reference to the anatomic descrip-
superior and posterior to the Gerdy tubercle. third of the lateral capsular ligament is di- tion provided by Hughston et al. in 1976 [4, 5].
The fracture is the result of excessive inter- vided into meniscofemoral and meniscotibial In 1988, Goldman et al. [15] performed a
nal rotation and varus stress and has a high portions. This is in accordance with the origi- retrospective review of double-contrast ar-
372 AJR:204, February 2015
MRI of Anterolateral Ligament of the Knee
thrograms that revealed a Segond fracture [3], have been describing, at times, different 4. Hughston JC, Andrews JR, Cross MJ, Moschi A.
to describe the clinical and radiographic fea- components of the same collective structure. Classification of knee ligament instabilities. Part
tures as well as associated soft-tissue injuries. Although the drawings published by Claes et I. The medial compartment and cruciate liga-
Those authors described the fracture as be- al. depict a discrete anterolateral ligament, ments. J Bone Joint Surg Am 1976; 58:159–172
ing the result of avulsion of the meniscotibi- we could not reliably see either a discrete 5. Hughston JC, Andrews JR, Cross MJ, Moschi A.
al attachment of the middle third of the later- structure or even a consistent focal thicken- Classification of knee ligament instabilities. Part
Downloaded from www.ajronline.org by 182.48.199.164 on 09/30/20 from IP address 182.48.199.164. Copyright ARRS. For personal use only; all rights reserved
al capsular ligament. Again, the fracture was ing of the lateral capsule in this area. For the II. The lateral compartment. J Bone Joint Surg
differentiated from an avulsion of the Gerdy radiologist, it may be best to forgo an attempt Am 1976; 58:173–179
tubercle at the insertion site of the iliotibial to separate this lateral structure into multi- 6. LaPrade RF, Gilbert TJ, Bollom TS, Wentorf F,
band. Diagrammatically, the lateral capsular ple components, such as the anterolateral lig- Chaljub G. The magnetic resonance imaging ap-
ligament was depicted as a large broad-based ament, capsuloosseous layer of the iliotibial pearance of individual structures of the postero-
structure running from the distal lateral femur tract, or anterior oblique band of the fibular lateral knee: a prospective study of normal knees
to the proximal lateral tibia [15]. collateral ligament, because these structures and knees with surgically verified grade III inju-
MRI characteristics of the Segond frac- are not reliably discriminated on routine ries. Am J Sports Med 2000; 28:191–199
ture were described by Weber et al. in 1991 MRI. Perhaps it would be most appropriate 7. Haims AH, Medvecky MJ, Pavlovich R Jr, Katz
[17]. The authors described the Segond frac- to give credit to Hughston and colleagues [4, LD. MR imaging of the anatomy of and injuries to
ture as a cortical avulsion of the meniscotib- 5] for their detailed description of this struc- the lateral and posterolateral aspects of the knee.
ial portion of the middle third of the lateral ture in 1976 and continue to refer to this por- AJR 2003; 180:647–653
capsular ligament of the knee. The avulsed tion of the lateral knee stabilizers as the lat- 8. Moorman CT 3rd, LaPrade RF. Anatomy and bio-
fracture fragment was seen on MRI in only eral capsular ligament. mechanics of the posterolateral corner of the
four of the 12 patients in the series and was Our study is limited by a lack of gross knee. J Knee Surg 2005; 18:137–145
seen on a single coronal image only. Howev- anatomic correlation, which could in theo- 9. Irvine GB, Dias JJ, Finlay DB. Segond fractures
er, abnormal bone marrow signal at the tibial ry provide a greater understanding of those of the lateral tibial condyle: brief report. J Bone
insertion of the capsular ligament and irreg- authors who referenced the structure un- Joint Surg Br 1987; 69:613–614
ularity and edema of the capsule and para- der investigation in the past. In addition, 10. Campos JC, Chung CB, Lektrakul N, et al. Patho-
capsular connective tissues were present on a more detailed depiction of the structure genesis of the Segond fracture: anatomic and MR
all cases. Although there was no MRI de- could have potentially been made if knee imaging evidence of an iliotibial tract or anterior
scription of injury to the middle third of the MRI studies were performed in partial oblique band avulsion. Radiology 2001; 219:381–386
lateral capsular ligament in that study, sur- flexion with internal rotation, a position in 11. Terry GC, Hughston JC, Norwood LA. The anat-
gical reports described complete avulsion of which this structure has been described as omy of the iliopatellar band and iliotibial tract.
the lateral capsular ligament from the later- being under stress in previous articles. Al- Am J Sports Med 1986; 14:39–45
al tibial plateau (four patients) or stretching though anatomic studies often use such op- 12. Vieira EL, Vieira EA, da Silva RT, Berlfein PA,
and fraying of this ligament (three patients) timized pulse sequences acquired in unique Abdalla RJ, Cohen M. An anatomic study of the
in over 50% of the patients [17]. planes at high resolution, the purpose of our iliotibial tract. Arthroscopy 2007; 23:269–274
Finally, a 1994 retrospective review by study is not to recapitulate the gross ana- 13.
Vincent JP, Magnussen RA, Gezmez F, et
Hess et al. [16] examined the relationship tomic work of Claes et al. [3] through the al. The anterolateral ligament of the human knee:
of the Segond fracture with concomitant use of MRI and prove that an anterolater- an anatomic and histologic study. Knee Surg
tear of the anterior cruciate ligament, and al ligament exists, but instead to provide Sports Traumatol Arthrosc 2012; 20:147–152
the Segond fracture was described as corre- an understanding of what the routine knee 14. Dietz GW, Wilcox DM, Montgomery JB. Segond
sponding to the distal insertion point of the MRI shows pertaining to that structure. Fi- tibial condyle fracture: lateral, capsular ligament
lateral capsular ligament or lateral menisco- nally, a more comprehensive assessment of avulsion. Radiology 1986; 159:467–469
tibial ligament. The authors described this the cause of the Segond avulsion fracture 15. Goldman AB, Pavlov H, Rubenstein D. The
as a component of the middle of the lateral would require the incorporation of cadav- Segond fracture of the proximal tibia: a small
joint capsule. As with prior reports, this le- eric specimens and systematic mechanical avulsion that reflects major ligamentous damage.
sion was differentiated from avulsion of the data, which is beyond the scope of our study AJR 1988; 151:1163–1167
Gerdy tubercle. Notably, their diagrammat- but a consideration for future research. 16. Hess T, Rupp S, Hopf T, Gleitz M, Liebler J. Lat-
ic illustration of the lateral capsular ligament eral tibial avulsion fractures and disruptions to the
depicted a thin ligamentous structure arising References anterior cruciate ligament: a clinical study of their
just anterior to the fibular collateral ligament 1. Manaster BJ. Knee section VI. In: Manaster BJ, incidence and correlation. Clin Orthop Relat Res
at the femoral insertion point and inserting Roberts RC, Andrews CL, et al., eds. Diagnostic 1994; 303:193–197
onto the lateral proximal tibia in a cordlike and surgical imaging anatomy musculoskeletal. 17. Weber WN, Neumann CH, Barakos JA, Petersen
fashion. In their series of 14 patients with Salt Lake City, UT: Amirsys, 2006:20–33 SA, Steinbach LS, Genant HK. Lateral tibial rim
Segond fractures, only two exhibited an ad- 2. Netter FH. Atlas of human anatomy, 5th ed. Phil- (Segond) fractures: MR imaging characteristics.
ditional injury to the lateral ligament struc- adelphia, PA: Saunders, 2011:472–476. Radiology 1991; 180:731–734
ture intraoperatively [16]. 3. Claes S, Vereecke E, Maes M, Victor J, Verdonk 18. Woods GW, Stanley RF, Tullos HS. Lateral cap-
In summary, it would appear that the P, Bellemans J. Anatomy of the anterolateral liga- sular sign: x-ray clue to a significant knee instabil-
works reviewed here, including Claes et al. ment of the knee. J Anat 2013; 223:321–328 ity. Am J Sports Med 1979; 7:27–33
AJR:204, February 2015 373
You might also like
- Muscle Coloring BookDocument9 pagesMuscle Coloring Bookjeaves14No ratings yet
- Matt and MariaDocument4 pagesMatt and MariaJanelle05110% (1)
- BBB Month 24 Workout LogDocument8 pagesBBB Month 24 Workout LogGeraldyneNo ratings yet
- Herniation of Cartilaginous Endplates in The Lumbar Spine MRI FindingsDocument7 pagesHerniation of Cartilaginous Endplates in The Lumbar Spine MRI FindingsOtong Zam ZamyNo ratings yet
- Dejesus 2009Document7 pagesDejesus 2009YassineNo ratings yet
- Advances in Magnetic Resonance Imaging Of.5Document10 pagesAdvances in Magnetic Resonance Imaging Of.5cooperorthopaedicsNo ratings yet
- Ligaments of The Transverse Tarsal Joint Complex: MRI-Anatomic Correlation in CadaversDocument10 pagesLigaments of The Transverse Tarsal Joint Complex: MRI-Anatomic Correlation in CadaversSaifuddin HaswareNo ratings yet
- Ajr 14 14266Document5 pagesAjr 14 14266Jorge Alberto GCNo ratings yet
- Ankle Ligaments On MRI: Appearance of Normal and Injured LigamentsDocument9 pagesAnkle Ligaments On MRI: Appearance of Normal and Injured Ligamentspjanu86No ratings yet
- Uas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDocument6 pagesUas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDwi Ajeng Risqy HasanahSyamNo ratings yet
- MRI of Spinal Bone Marro Part 1 Techniques and Normal Age-Related AppearancesDocument11 pagesMRI of Spinal Bone Marro Part 1 Techniques and Normal Age-Related AppearancesAyşe BanuNo ratings yet
- Lokasi Tulang PanjangDocument10 pagesLokasi Tulang PanjangTenri3232No ratings yet
- Imaging Evaluation of Developmental Hip Dysplasia in The Young AdultDocument12 pagesImaging Evaluation of Developmental Hip Dysplasia in The Young AdultHasna A KhairunisaNo ratings yet
- Irm Denervation ÉpauleDocument7 pagesIrm Denervation ÉpaulenessimNo ratings yet
- Effect of Posterior Malleolus Fracture On.10Document6 pagesEffect of Posterior Malleolus Fracture On.10Charlie KorbaNo ratings yet
- Skeletal Development of The Proximal Humerus in The Pediatric Population: MRI FeaturesDocument10 pagesSkeletal Development of The Proximal Humerus in The Pediatric Population: MRI Featuresahmed doweidarNo ratings yet
- Lephart - J Shouler and Elbow - Proprioceptio of ShoulderDocument10 pagesLephart - J Shouler and Elbow - Proprioceptio of ShoulderMateus HenriqueNo ratings yet
- The Clinical Correlation of A New Practical MRI Method For Grading Cervical Neural Foraminal Stenosis Based On Oblique Sagittal ImagesDocument6 pagesThe Clinical Correlation of A New Practical MRI Method For Grading Cervical Neural Foraminal Stenosis Based On Oblique Sagittal ImagesThiago Astil RizzettoNo ratings yet
- Covey JBJS PCL InjuriesDocument11 pagesCovey JBJS PCL InjuriesGirish HNo ratings yet
- Regla Convexa - ConcavaDocument4 pagesRegla Convexa - ConcavaFernando Saad Magariños SelaiveNo ratings yet
- Magnetic Resonance Imaging - 2010 - Jordanov - Minute Amounts of Intraarticular Gas Mimicking Torn Discoid Lateral MenisciDocument5 pagesMagnetic Resonance Imaging - 2010 - Jordanov - Minute Amounts of Intraarticular Gas Mimicking Torn Discoid Lateral Meniscinessim zouariNo ratings yet
- Halo Clinical Evidence PapersDocument5 pagesHalo Clinical Evidence PapersCalugareanu MadalinaNo ratings yet
- Anatomy and Function of The Temporomandib-Ular Joint: Michael M. Helland, Ma, PTDocument9 pagesAnatomy and Function of The Temporomandib-Ular Joint: Michael M. Helland, Ma, PTMelvin JamesNo ratings yet
- The Early Management of Open Joint Injuries. A Prospective Study of One Hundred and Forty PatientsDocument8 pagesThe Early Management of Open Joint Injuries. A Prospective Study of One Hundred and Forty PatientsLuigi Paolo Zapata DelgadoNo ratings yet
- Implant Related Fractures of The Femur Following.4Document7 pagesImplant Related Fractures of The Femur Following.4ANA MARIA ROCIO HURTADO ORTEGANo ratings yet
- Kwong Et Al 2014 Skeletal Development of The Proximal Humerus in The Pediatric Population Mri FeaturesDocument8 pagesKwong Et Al 2014 Skeletal Development of The Proximal Humerus in The Pediatric Population Mri FeaturesMessah V DianaNo ratings yet
- Oarsi 2Document3 pagesOarsi 2Mohd Yusof BaharuddinNo ratings yet
- Sonography of The Neonatal Spine: Part 2, Spinal Disorders: Lisa H. Lowe Andrew J. Johanek Charlotte W. MooreDocument6 pagesSonography of The Neonatal Spine: Part 2, Spinal Disorders: Lisa H. Lowe Andrew J. Johanek Charlotte W. MooredrmateensiddiquiNo ratings yet
- Silverstein 2009Document28 pagesSilverstein 2009tratrNo ratings yet
- Bone Marrow Signal Alteration in The Spine and Sacrum: ResidentsDocument23 pagesBone Marrow Signal Alteration in The Spine and Sacrum: ResidentsTestNo ratings yet
- Connie C So Imaging of The Pubic Symphysis Anatomy andDocument2 pagesConnie C So Imaging of The Pubic Symphysis Anatomy andLevi PNo ratings yet
- Patterns of Premature Physeal Arrest:: MR Imaging of 111 ChildrenDocument6 pagesPatterns of Premature Physeal Arrest:: MR Imaging of 111 Childrenjose pablo reyes ortizNo ratings yet
- Knee Pain H and P PDFDocument6 pagesKnee Pain H and P PDFKKNo ratings yet
- MRI of The Peritoneum: Spectrum of AbnormalitiesDocument12 pagesMRI of The Peritoneum: Spectrum of AbnormalitiesasfwegereNo ratings yet
- Imaging of Blunt Thoracic TraumaDocument24 pagesImaging of Blunt Thoracic TraumaZai RojasNo ratings yet
- Ajr 09 2712Document10 pagesAjr 09 2712CuauhtémocNo ratings yet
- Patrones de LesionDocument6 pagesPatrones de LesionMathias TaritolayNo ratings yet
- Ajr 11 7440Document6 pagesAjr 11 7440khadesakshi55No ratings yet
- Bone Marrow T1-W DifferentialDocument17 pagesBone Marrow T1-W DifferentialStancu Oana RuxandraNo ratings yet
- Dental Occlusion and Body Posture: A Surface EMG Study: Cranio®Document9 pagesDental Occlusion and Body Posture: A Surface EMG Study: Cranio®Kiss KatalinNo ratings yet
- Intramedullary Nailing of Pediatric Femoral Shaft FractureDocument10 pagesIntramedullary Nailing of Pediatric Femoral Shaft FractureJayNo ratings yet
- Osteochondral Lesions of The Knee Differentiating The Most Common Entities at MRI ODLICNODocument18 pagesOsteochondral Lesions of The Knee Differentiating The Most Common Entities at MRI ODLICNOdrbane123No ratings yet
- Biomechanics of Craniofacial Sutures Orthopedic ImplicationsDocument8 pagesBiomechanics of Craniofacial Sutures Orthopedic ImplicationsMuhammad FahmyNo ratings yet
- Articular Cartilage and Osteoarthritis: Henry J. Mankin, MD Alan J. Grodzinsky, SCD Joseph A. Buckwalter, MD, MsDocument14 pagesArticular Cartilage and Osteoarthritis: Henry J. Mankin, MD Alan J. Grodzinsky, SCD Joseph A. Buckwalter, MD, MsIkre19No ratings yet
- MRI of Spinal Bone Marrow Part 2 T1-Weighted Imaging-Based Differential DiagnosisDocument13 pagesMRI of Spinal Bone Marrow Part 2 T1-Weighted Imaging-Based Differential DiagnosisAyşe BanuNo ratings yet
- Three-Dimensional Cephalometric Analysis The Changes in Condylar Position Pre - and Post-Orthognathic Surgery With Skeletal Class III MalocclusionDocument6 pagesThree-Dimensional Cephalometric Analysis The Changes in Condylar Position Pre - and Post-Orthognathic Surgery With Skeletal Class III MalocclusionPhachara SiripraphonrojNo ratings yet
- Imaging Analyses of Bone Tumors JBJSDocument11 pagesImaging Analyses of Bone Tumors JBJSVera VeraNo ratings yet
- Ankle and Foot Injuries:: Analysis of MDCT FindingsDocument8 pagesAnkle and Foot Injuries:: Analysis of MDCT FindingsraditNo ratings yet
- Lee2003 Article ArcuateSignOfPosterolateralKneDocument9 pagesLee2003 Article ArcuateSignOfPosterolateralKneMaddy WolsmenNo ratings yet
- Thirty Years Later: What Has Craniofacial Distraction Osteogenesis Surgery Replaced?Document16 pagesThirty Years Later: What Has Craniofacial Distraction Osteogenesis Surgery Replaced?varelarmNo ratings yet
- Fracture of The Distal Radius: Epidemiology and Premanagement Radiographic CharacterizationDocument9 pagesFracture of The Distal Radius: Epidemiology and Premanagement Radiographic CharacterizationodivarNo ratings yet
- Jospt 2014 5523Document9 pagesJospt 2014 5523杨钦杰No ratings yet
- Ajr 12 8488Document5 pagesAjr 12 8488Belen CoronaNo ratings yet
- 1 s2.0 S0021929012002801 MainDocument6 pages1 s2.0 S0021929012002801 MainCarlos De la cruzNo ratings yet
- Ajr 12 10083Document9 pagesAjr 12 10083odivarNo ratings yet
- Daffa Gemineo Dheona - 31102000017 - Literature ReviewDocument2 pagesDaffa Gemineo Dheona - 31102000017 - Literature ReviewRahmadhani AtmiantoNo ratings yet
- Unilateral Locked Facet in Cervical Spine Injuries: Anatomy of Apophyseal JointsDocument4 pagesUnilateral Locked Facet in Cervical Spine Injuries: Anatomy of Apophyseal JointsMikael AngelooNo ratings yet
- Modal Analysis of Femur Bone Using Finite Element Method For Healthcare SystemDocument5 pagesModal Analysis of Femur Bone Using Finite Element Method For Healthcare Systemimen mehriNo ratings yet
- Harish Chandra Saurabh - 22mt0145Document11 pagesHarish Chandra Saurabh - 22mt0145dr r r dasNo ratings yet
- 498 MRI of Anterior Cruciate LigamentDocument7 pages498 MRI of Anterior Cruciate LigamentChinmay SalunkeNo ratings yet
- Patient-Specific Medial Unicompartmental Knee Arthroplasty Has A Greater Protective Effect On Articular Cartilage in The Lateral CompartmentDocument8 pagesPatient-Specific Medial Unicompartmental Knee Arthroplasty Has A Greater Protective Effect On Articular Cartilage in The Lateral CompartmentSAM IMNo ratings yet
- Oculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsFrom EverandOculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNo ratings yet
- SDJ 2018-05 ResearchDocument11 pagesSDJ 2018-05 ResearchSaifuddin HaswareNo ratings yet
- Chapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartDocument53 pagesChapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartSaifuddin HaswareNo ratings yet
- Oral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot StudyDocument7 pagesOral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot StudySaifuddin HaswareNo ratings yet
- JCDP 20 444Document5 pagesJCDP 20 444Saifuddin HaswareNo ratings yet
- Capture of Hair Geometry From Multiple ImagesDocument8 pagesCapture of Hair Geometry From Multiple ImagesSaifuddin HaswareNo ratings yet
- Adenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceDocument7 pagesAdenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceSaifuddin HaswareNo ratings yet
- Mono99 17Document160 pagesMono99 17Saifuddin HaswareNo ratings yet
- Crisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Document12 pagesCrisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Saifuddin HaswareNo ratings yet
- Psoriasis and Cardiovascular Disease: Where Is The Risk?: CommentaryDocument4 pagesPsoriasis and Cardiovascular Disease: Where Is The Risk?: CommentarySaifuddin HaswareNo ratings yet
- Cheng JARODocument15 pagesCheng JAROSaifuddin HaswareNo ratings yet
- Splenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapyDocument9 pagesSplenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapySaifuddin HaswareNo ratings yet
- 286 FullDocument8 pages286 FullSaifuddin HaswareNo ratings yet
- Variations of Hair Follicle Size and Distribution in Different Body SitesDocument6 pagesVariations of Hair Follicle Size and Distribution in Different Body SitesSaifuddin HaswareNo ratings yet
- Uncombable Hair SyndromeDocument3 pagesUncombable Hair SyndromeSaifuddin HaswareNo ratings yet
- September 2013 BourlandDocument38 pagesSeptember 2013 BourlandSaifuddin HaswareNo ratings yet
- Hair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsDocument15 pagesHair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsSaifuddin HaswareNo ratings yet
- Inexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishDocument7 pagesInexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishSaifuddin HaswareNo ratings yet
- Thymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationDocument9 pagesThymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationSaifuddin HaswareNo ratings yet
- Noise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKDocument14 pagesNoise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKSaifuddin HaswareNo ratings yet
- Root Hair Mutants of BarleyDocument6 pagesRoot Hair Mutants of BarleySaifuddin HaswareNo ratings yet
- 16th Master Course AgendaDocument2 pages16th Master Course AgendaSuvodipBhattacharyaNo ratings yet
- OSTEOLOGY Lower Limb 3 and 4Document5 pagesOSTEOLOGY Lower Limb 3 and 4Famela Anne GOmez MadambaNo ratings yet
- Biomechanics of Common Sports InjuriesDocument74 pagesBiomechanics of Common Sports InjuriesAnuruddha100% (3)
- Lesson #8: Nervous Tissue AND Bones & Muscles of The Lower LimbDocument15 pagesLesson #8: Nervous Tissue AND Bones & Muscles of The Lower LimbMaria GarciaNo ratings yet
- 1.1 Plantar Foot Pressure 1.1.1 Plantar SurfaceDocument5 pages1.1 Plantar Foot Pressure 1.1.1 Plantar SurfaceNivethitha DevarajNo ratings yet
- 006 KAFO - Biomechanics LECTURE-1Document23 pages006 KAFO - Biomechanics LECTURE-1Alfred JacksonNo ratings yet
- American Board of Orthopaedic Surgery: Acceptable CPT Codes For Orthopaedic Sports Medicine Subspecialty Case ListDocument13 pagesAmerican Board of Orthopaedic Surgery: Acceptable CPT Codes For Orthopaedic Sports Medicine Subspecialty Case ListKrishna KumarNo ratings yet
- INTOEINGDocument1 pageINTOEINGJoanne AngelicaNo ratings yet
- The Trigger Point Referred Pain Guide Interactive 1Document439 pagesThe Trigger Point Referred Pain Guide Interactive 1eloganbyman91% (11)
- 10 1007@s00068-mfjrbtDocument14 pages10 1007@s00068-mfjrbtJGunar VasquezNo ratings yet
- v1 500197 Reva Navio 7 All Knees Surgical Technique 06.19Document52 pagesv1 500197 Reva Navio 7 All Knees Surgical Technique 06.19febyan yohanesNo ratings yet
- Ankle Foot Exam PDFDocument2 pagesAnkle Foot Exam PDFZeeshan SiddiquiNo ratings yet
- Club Foot-Dr J SahooDocument9 pagesClub Foot-Dr J SahooSheel Gupta100% (1)
- Warmup BadmintonDocument2 pagesWarmup Badmintonapi-345720435No ratings yet
- Chapter 11 NotesDocument12 pagesChapter 11 NotesAzwar Arsyad S SiNo ratings yet
- ACL Reconstruction History and Current Concepts: Sean Hazzard, PA-C Massachusetts General Hospital Boston, MADocument7 pagesACL Reconstruction History and Current Concepts: Sean Hazzard, PA-C Massachusetts General Hospital Boston, MAana starcevicNo ratings yet
- 1pages From The Anatomy of Stretching, Seco - Walker, BradDocument6 pages1pages From The Anatomy of Stretching, Seco - Walker, BradFatimah SalsabilaNo ratings yet
- Correction of Foot Deformities With Ilizarov Methodology. Nuno Craveiro LopesDocument50 pagesCorrection of Foot Deformities With Ilizarov Methodology. Nuno Craveiro LopesNuno Craveiro LopesNo ratings yet
- GastrocnemiusDocument3 pagesGastrocnemiustuhinsinghNo ratings yet
- 16-Front of ThighDocument27 pages16-Front of ThighLaiba FaysalNo ratings yet
- Normal Gait Mechanics: Weight UnloadingDocument3 pagesNormal Gait Mechanics: Weight UnloadingequalbenNo ratings yet
- Lower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyDocument56 pagesLower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyKavya Mittal100% (2)
- Lecture 12 Skeletal System Lower Limb (Surface Anatomy)Document29 pagesLecture 12 Skeletal System Lower Limb (Surface Anatomy)hafiz patahNo ratings yet
- Basic Knee Arthroscopy Part 3Document3 pagesBasic Knee Arthroscopy Part 3Diego BellingNo ratings yet
- Knee FlexionDocument4 pagesKnee FlexionJeg1No ratings yet
- Atp500 Stretch Strap GuideDocument2 pagesAtp500 Stretch Strap Guidevandananayar7578No ratings yet
- Plantar Fasciitis Ebook GuideDocument29 pagesPlantar Fasciitis Ebook GuideIkshitNo ratings yet