Download as pdf or txt
You might also like
- PFC Matrix: Copo, Nico Angelo PDocument5 pagesPFC Matrix: Copo, Nico Angelo PUniperhels Cohealic67% (3)
- Phototherapy ChecklistDocument2 pagesPhototherapy ChecklistMA. JIZELLE (CELSO) SINFUEGO100% (2)
- 190 - Gestational Diabetes Mellitus AgogDocument16 pages190 - Gestational Diabetes Mellitus Agogjorge vergara100% (2)
- Annotated BibliographyDocument20 pagesAnnotated Bibliographyapi-347153077No ratings yet
- 17 Diagnostic Strategies For Gestational Diabetes MellitusreviewDocument10 pages17 Diagnostic Strategies For Gestational Diabetes MellitusreviewdianaNo ratings yet
- Temporary Changes in Clinical Guidelines of Gesta - 2020 - Diabetes - Metabolic PDFDocument4 pagesTemporary Changes in Clinical Guidelines of Gesta - 2020 - Diabetes - Metabolic PDFdianNo ratings yet
- Towards A Global Consensus On GDM Diagnosis Light at The End of The TunnelDocument5 pagesTowards A Global Consensus On GDM Diagnosis Light at The End of The TunnelYuliana NaviaNo ratings yet
- Prenatal Diagnosis - 2020 - Murray - Short and Long Term Outcomes of Gestational Diabetes and Its Treatment On FetalDocument7 pagesPrenatal Diagnosis - 2020 - Murray - Short and Long Term Outcomes of Gestational Diabetes and Its Treatment On FetalVicente Fasce OlmosNo ratings yet
- Gestational Diabetes Mellitus Update and Review of Literature 2161 038X.S2 008 PDFDocument6 pagesGestational Diabetes Mellitus Update and Review of Literature 2161 038X.S2 008 PDFBuluan Mps McadNo ratings yet
- Who PDFDocument23 pagesWho PDFMayra PereiraNo ratings yet
- Journal GAJOMSDocument6 pagesJournal GAJOMSmade dharmaNo ratings yet
- STATEMENTS ADIPS GDM Management GuidelinesDocument10 pagesSTATEMENTS ADIPS GDM Management Guidelineskitten garciaNo ratings yet
- Comparison of Glyburide and Insulin in The Man PDFDocument18 pagesComparison of Glyburide and Insulin in The Man PDFwinda istikhomahNo ratings yet
- Jurnal ObgynDocument8 pagesJurnal ObgynayuNo ratings yet
- Diabetes Gestacional Una Actualizacion 2022Document31 pagesDiabetes Gestacional Una Actualizacion 2022CARLOS MACHADONo ratings yet
- 2021 Diagnosis and Management of Gestational Diabetes Mellitus An Overview of National and International GuidelinesDocument15 pages2021 Diagnosis and Management of Gestational Diabetes Mellitus An Overview of National and International GuidelinesJuan Pablo Patiño SánchezNo ratings yet
- Gestational Diabetes Mellitus Acog CopDocument8 pagesGestational Diabetes Mellitus Acog CopAndrea Sandoval OteroNo ratings yet
- Womens Health Diabetes MellitusDocument17 pagesWomens Health Diabetes Mellitusshubham kumarNo ratings yet
- ACOG Practice Bulletin No137 PDFDocument11 pagesACOG Practice Bulletin No137 PDFRodrigo Pérez CuelloNo ratings yet
- Diabetes Acog 2017Document15 pagesDiabetes Acog 2017Holger Vicente Guerrero Guerrero100% (1)
- Maternal and Perinatal Outcome in Gestational Diabetes Mellitus Compared To Pregestational Diabetes MellitusDocument6 pagesMaternal and Perinatal Outcome in Gestational Diabetes Mellitus Compared To Pregestational Diabetes MellitusrischaNo ratings yet
- Beyond Pregnancy Understanding The Long-Term Implications of Gestational Diabetes MellitusDocument9 pagesBeyond Pregnancy Understanding The Long-Term Implications of Gestational Diabetes MellitusKIU PUBLICATION AND EXTENSIONNo ratings yet
- Gestational Diabetes Mellitus (GDM)Document33 pagesGestational Diabetes Mellitus (GDM)Sri WahyuniNo ratings yet
- 11 ORATILE. P. ROBERTO OLMOSTrat. Con Dieta y EjercicoDocument8 pages11 ORATILE. P. ROBERTO OLMOSTrat. Con Dieta y Ejercicoiriartenela14No ratings yet
- ACOG Tech BullitinDocument20 pagesACOG Tech BullitinJosephNo ratings yet
- 10 1097aog 0000000000002159Document15 pages10 1097aog 0000000000002159Kathleen Cherrepano AguirreNo ratings yet
- Guide Who Hyperglycaemia PregnancyDocument44 pagesGuide Who Hyperglycaemia PregnancyThinzar NweNo ratings yet
- Screening and DiagnosisDocument25 pagesScreening and DiagnosisM AbhiNo ratings yet
- WHo GDSDocument62 pagesWHo GDSM Fathur Arief KurniawanNo ratings yet
- Gestational Diabetes Mellitus: New Diagnostic CriteriaDocument7 pagesGestational Diabetes Mellitus: New Diagnostic CriteriaRambuNo ratings yet
- Thesis TopicDocument17 pagesThesis Topicreamer27100% (1)
- Literature Review of Gestational Diabetes MellitusDocument7 pagesLiterature Review of Gestational Diabetes Mellitusc5rc7ppr100% (1)
- The Elusive Diagnosis of Gestational Diabetes: Guest EditorialDocument4 pagesThe Elusive Diagnosis of Gestational Diabetes: Guest EditorialSarly FebrianaNo ratings yet
- Repub 103040-OaDocument8 pagesRepub 103040-OaEmma Lyn SantosNo ratings yet
- The Risk of Overt Diabetes Mellitus AmonDocument7 pagesThe Risk of Overt Diabetes Mellitus AmonΛΟΥΚΙΑ ΣΠΑΝΟΥNo ratings yet
- Diabetes Mellitus GestationalDocument19 pagesDiabetes Mellitus GestationalYosefin RatnaningtyasNo ratings yet
- Local Versus International Criteria in Predicting Gestational Diabetes Mellitus Related Pregnancy OutcomesDocument10 pagesLocal Versus International Criteria in Predicting Gestational Diabetes Mellitus Related Pregnancy OutcomesCj CCNo ratings yet
- Single-Step DIPSI 75g Glucose Tolerance Test-For Diagnosis of Gestational Diabetes MellitusDocument7 pagesSingle-Step DIPSI 75g Glucose Tolerance Test-For Diagnosis of Gestational Diabetes MellitusEditor ERWEJNo ratings yet
- Gestationaldiabetes Mellitus: Emily D. Szmuilowicz,, Jami L. Josefson,, Boyd E. MetzgerDocument15 pagesGestationaldiabetes Mellitus: Emily D. Szmuilowicz,, Jami L. Josefson,, Boyd E. Metzgerjose ricardo escalante perezNo ratings yet
- Antenatal Screening PIT POGI 2023Document62 pagesAntenatal Screening PIT POGI 2023Rachmat HasanNo ratings yet
- Cost-Effectiveness of Controlling Gestational Diabetes Mellitus: A Systematic ReviewDocument11 pagesCost-Effectiveness of Controlling Gestational Diabetes Mellitus: A Systematic ReviewjunifitrahNo ratings yet
- Gestational Diabetes Mellitus Where Are We NowDocument7 pagesGestational Diabetes Mellitus Where Are We NowjohnturpoNo ratings yet
- Prevalence of Gestational Diabetes Mellitus and Associated Factors Among Women Attending Antenatal Care at Gondar Town Public Health FacilitiesDocument12 pagesPrevalence of Gestational Diabetes Mellitus and Associated Factors Among Women Attending Antenatal Care at Gondar Town Public Health FacilitieswuhemosesNo ratings yet
- The Pathophysiology of Gestational Diabetes MellitusDocument35 pagesThe Pathophysiology of Gestational Diabetes MellituscalliemozartNo ratings yet
- GDM DefinitionDocument3 pagesGDM Definitionsheryl yangNo ratings yet
- Review of Literature Related To Gestational Diabetes MellitusDocument9 pagesReview of Literature Related To Gestational Diabetes MellituscdkxbcrifNo ratings yet
- Gestational Diabetes Mellitus, Diagnostic Approaches and Maternal Offspring ComplicationsDocument12 pagesGestational Diabetes Mellitus, Diagnostic Approaches and Maternal Offspring ComplicationsSaraid RuizNo ratings yet
- Benhalima Katrien Management of Type 1 Diabetes inDocument19 pagesBenhalima Katrien Management of Type 1 Diabetes inPASMOXNo ratings yet
- Gestational Diabetes Mellitus ThesisDocument4 pagesGestational Diabetes Mellitus Thesisbseb81xq100% (2)
- Prevalence of Gestational Diabetes Mellitus Evaluated by Universal Screening With A 75-g, 2 - Hour Oral Glucose Tolerance Test and IADPSG CriteriaDocument4 pagesPrevalence of Gestational Diabetes Mellitus Evaluated by Universal Screening With A 75-g, 2 - Hour Oral Glucose Tolerance Test and IADPSG CriteriaCamila Alicia López AndradeNo ratings yet
- Aisyah GDM ArticleDocument18 pagesAisyah GDM ArticleBesari Md DaudNo ratings yet
- Gestational Diabetes Mellitus Screening and Outcomes: Original Investigation 25Document5 pagesGestational Diabetes Mellitus Screening and Outcomes: Original Investigation 25Eduardo SasintuñaNo ratings yet
- Medi 102 E33898Document7 pagesMedi 102 E33898ade lydia br.siregarNo ratings yet
- Diabetes Gestacional Revision 2019Document15 pagesDiabetes Gestacional Revision 2019zaaaidaNo ratings yet
- 4 Gestational Diabetes MellitusDocument12 pages4 Gestational Diabetes MellitusAnonymous tgLZ9uvXsNo ratings yet
- DIPSI GuidelinesDocument7 pagesDIPSI GuidelinesvinaypharmNo ratings yet
- Screening and Diagnosis GDMDocument3 pagesScreening and Diagnosis GDMAkarapon SugandhanandaNo ratings yet
- Screening For Biomarkers Predictive of Gestational Diabetes MellitusDocument9 pagesScreening For Biomarkers Predictive of Gestational Diabetes MellitusTomNo ratings yet
- Diabetes Gestacional HapoDocument16 pagesDiabetes Gestacional HapoFelipe Cortés VegaNo ratings yet
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalFrom EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalNo ratings yet
- Semaglutide Unveiled: A Comprehensive Guide to Diabetes Treatment and Weight ManagementFrom EverandSemaglutide Unveiled: A Comprehensive Guide to Diabetes Treatment and Weight ManagementNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Determinants of Vitamin B12 Deficiency in Patients With Type-2 Diabetes Mellitus - A Primary-Care Retrospective Cohort StudyDocument16 pagesDeterminants of Vitamin B12 Deficiency in Patients With Type-2 Diabetes Mellitus - A Primary-Care Retrospective Cohort StudyM AbhiNo ratings yet
- Special Considerations in Treating Bipolar Disorder in WomenDocument12 pagesSpecial Considerations in Treating Bipolar Disorder in WomenM AbhiNo ratings yet
- Fogsi Statement On Covid Vaccination in Pregnancy and BFDocument16 pagesFogsi Statement On Covid Vaccination in Pregnancy and BFM AbhiNo ratings yet
- Vyapti Infrabuild PVT - LTD.: Duvf - U QHN (Document2 pagesVyapti Infrabuild PVT - LTD.: Duvf - U QHN (M AbhiNo ratings yet
- Vyapti Infrabuild PVT - LTD.: Duvf - U QHN (Document2 pagesVyapti Infrabuild PVT - LTD.: Duvf - U QHN (M AbhiNo ratings yet
- Impact of Antibiotic Policy On Antibiotic Consumption in A Neonatal Intensive Care Unit in IndiaDocument3 pagesImpact of Antibiotic Policy On Antibiotic Consumption in A Neonatal Intensive Care Unit in IndiaM AbhiNo ratings yet
- A Step Closer in The Management of Uncontrolled Neuropathic Pain: Gabapentin-Nortriptyline CombinationDocument6 pagesA Step Closer in The Management of Uncontrolled Neuropathic Pain: Gabapentin-Nortriptyline CombinationM AbhiNo ratings yet
- Rizatriptan Tablet Versus Wafer: Patient PreferenceDocument2 pagesRizatriptan Tablet Versus Wafer: Patient PreferenceM AbhiNo ratings yet
- Screening and DiagnosisDocument25 pagesScreening and DiagnosisM AbhiNo ratings yet
- Vitamin D Depression 2020Document12 pagesVitamin D Depression 2020M AbhiNo ratings yet
- Indian ScenarioDocument10 pagesIndian ScenarioM AbhiNo ratings yet
- Accepted Manuscript: Clinics in DermatologyDocument30 pagesAccepted Manuscript: Clinics in DermatologyM AbhiNo ratings yet
- Efficacy of Terlipressin in Upper Gi Bleeding Due To Liver CirrhosisDocument3 pagesEfficacy of Terlipressin in Upper Gi Bleeding Due To Liver CirrhosisM AbhiNo ratings yet
- First Trimester BiomarkersDocument10 pagesFirst Trimester BiomarkersM AbhiNo ratings yet
- Upa Study PDFDocument17 pagesUpa Study PDFM AbhiNo ratings yet
- Towards A European Consensus On Gestational Diabetes Mellitus: A Pragmatic Guide For Diagnosis, Management, and CareDocument4 pagesTowards A European Consensus On Gestational Diabetes Mellitus: A Pragmatic Guide For Diagnosis, Management, and CareM AbhiNo ratings yet
- Middle East Fertility Society Journal: Maryam Eftekhar, Elham Naghshineh, Nosrat Neghab, Robabe HosseinisadatDocument4 pagesMiddle East Fertility Society Journal: Maryam Eftekhar, Elham Naghshineh, Nosrat Neghab, Robabe HosseinisadatM AbhiNo ratings yet
- Recombinant Versus Urinary Follicle Stimulating Hormone For Ovarian Stimulation in Assisted ReproductionDocument9 pagesRecombinant Versus Urinary Follicle Stimulating Hormone For Ovarian Stimulation in Assisted ReproductionM AbhiNo ratings yet
- Saving The Zone of Stasis: Is Glutathione Effective?Document5 pagesSaving The Zone of Stasis: Is Glutathione Effective?M AbhiNo ratings yet
- Partnership For Cause Smart Fecal Management: SankoyaDocument14 pagesPartnership For Cause Smart Fecal Management: SankoyaKarthikeyan ArumugathandavanNo ratings yet
- Tablet Coamoxiclave (Amoxicillin +clavulanic Acid) Indications and DosDocument2 pagesTablet Coamoxiclave (Amoxicillin +clavulanic Acid) Indications and DosShumaila Iftikhar Iftikhar AhmadNo ratings yet
- Tugas 1 Wrap (Mencari 3 Jurnal Internasional) : Kristal Puan Bazukarno - 1603190013Document7 pagesTugas 1 Wrap (Mencari 3 Jurnal Internasional) : Kristal Puan Bazukarno - 1603190013Kristal PuanNo ratings yet
- Risk, Toxicology, and Human HealthDocument51 pagesRisk, Toxicology, and Human Healtharief muhammadNo ratings yet
- Hospital Disaster Preparedness: Making Disaster Resilient Hospitals .Document18 pagesHospital Disaster Preparedness: Making Disaster Resilient Hospitals .Tarun BhandariNo ratings yet
- AIDS NB 2009 Annual ReportDocument12 pagesAIDS NB 2009 Annual ReportAIDSNBNo ratings yet
- Collector MeetingDocument56 pagesCollector MeetingPorkodi SengodanNo ratings yet
- Family Planning: Natural MethodDocument5 pagesFamily Planning: Natural MethodAngelaNo ratings yet
- 1180 Project ReportDocument62 pages1180 Project Reportkarthikeyan01No ratings yet
- Primary Health CareDocument54 pagesPrimary Health CareAretecode777No ratings yet
- Unit 7 - Construction SafetyDocument2 pagesUnit 7 - Construction SafetyEmanErNo ratings yet
- NGCP 3yearsDocument19 pagesNGCP 3yearsMyra Leah AguilaNo ratings yet
- PCB Annexes A1-A5Document7 pagesPCB Annexes A1-A5Kleen Castro100% (4)
- ANTIBIOTICSDocument14 pagesANTIBIOTICSAll NewtNo ratings yet
- Makerere University College of HealthsciencesDocument43 pagesMakerere University College of HealthscienceskazulamaNo ratings yet
- ArciagaDocument5 pagesArciagaJerecho Ramon R. ArciagaNo ratings yet
- 5165 Scaling Up Primary Health Care in The Philippines Lessons From A Systematic Review of Experiences of Community Based Health ProgramsDocument9 pages5165 Scaling Up Primary Health Care in The Philippines Lessons From A Systematic Review of Experiences of Community Based Health ProgramsHanako Sasaki AranillaNo ratings yet
- FFamily Case Study Compilation 2Document501 pagesFFamily Case Study Compilation 2Trisha Anne WacasNo ratings yet
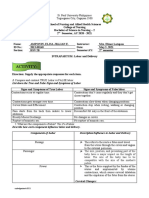
- Amponin, Elisa Jillian E. - Intrapartum Labor and Delivery Activity SheetDocument7 pagesAmponin, Elisa Jillian E. - Intrapartum Labor and Delivery Activity SheetJillian AmponinNo ratings yet
- Postpartum ComplicationsDocument15 pagesPostpartum Complicationspadmja4purohitNo ratings yet
- World Health Days Excel UpdatedDocument6 pagesWorld Health Days Excel UpdatedSuneeth Nedunoori (Chintu)No ratings yet
- Helpful and Harmful Microorganisms (Autosaved)Document10 pagesHelpful and Harmful Microorganisms (Autosaved)SIDUNo ratings yet
- Background: Amniotomy For Shortening Spontaneous LabourDocument3 pagesBackground: Amniotomy For Shortening Spontaneous Labourdewi lilisNo ratings yet
- CoparDocument51 pagesCoparGregg PalabricaNo ratings yet
- 1683personalhygiene WorksheetDocument6 pages1683personalhygiene Worksheetramzan aliNo ratings yet
- Imojev - Product InformationDocument14 pagesImojev - Product InformationwalkrogNo ratings yet
- 4.2b Erdos, China - An Eco-Town Pilot ProjectDocument10 pages4.2b Erdos, China - An Eco-Town Pilot ProjectAakarsh GoyalNo ratings yet
- Final Drug Study - PediaDocument2 pagesFinal Drug Study - PediaMae Estillore100% (1)