Download as pdf or txt
You might also like
- Acetic Acid Production ReportDocument15 pagesAcetic Acid Production ReportArya Lodha100% (1)
- A Family Guide 20 Easy Steps To Personal Environmental Health Now 508Document8 pagesA Family Guide 20 Easy Steps To Personal Environmental Health Now 508SaiKai54No ratings yet
- Safety Data Sheet: 1. IdentificationDocument15 pagesSafety Data Sheet: 1. IdentificationFelix Vejar ZepedaNo ratings yet
- Harmful Carcinogenic Ingredients in Skin CareDocument3 pagesHarmful Carcinogenic Ingredients in Skin CareDisha T100% (1)
- Causticingestionsand Foreignbodiesingestions InpediatricpatientsDocument18 pagesCausticingestionsand Foreignbodiesingestions InpediatricpatientsmacedovendezuNo ratings yet
- Household Chemicals: Management of Intoxication and AntidotesDocument2 pagesHousehold Chemicals: Management of Intoxication and AntidotesHamida MidaNo ratings yet
- Significado de ToxindromeDocument8 pagesSignificado de ToxindromeRene Alexis Rodriguez JoaquinNo ratings yet
- De La Torre-Ftd-Ppt-HealthDocument43 pagesDe La Torre-Ftd-Ppt-HealthJay -R ArmeroNo ratings yet
- 10.1007@978 3 7643 8338 110Document25 pages10.1007@978 3 7643 8338 110Hamida MidaNo ratings yet
- Body Care Ingredients To AvoidDocument4 pagesBody Care Ingredients To AvoidadriagNo ratings yet
- Cleaners Hall of ShameDocument9 pagesCleaners Hall of ShameteamballNo ratings yet
- A Consumerýs Dictionary of Household, Yard and Office Chemicals: Complete Information About Harmful and Desirable Chemicals Found in Everyday Home Products, Yard Poisons, and Office PollutersFrom EverandA Consumerýs Dictionary of Household, Yard and Office Chemicals: Complete Information About Harmful and Desirable Chemicals Found in Everyday Home Products, Yard Poisons, and Office PollutersNo ratings yet
- Laundry Detergent Capsules and Pediatric Poisoning: Child Health UpdateDocument2 pagesLaundry Detergent Capsules and Pediatric Poisoning: Child Health UpdateineNo ratings yet
- Water They Drink, and The Places Where They Live."Document14 pagesWater They Drink, and The Places Where They Live."Martina WestcottNo ratings yet
- R.P 5Document6 pagesR.P 5Poma PanezaiNo ratings yet
- Chem Final EssayDocument5 pagesChem Final Essayapi-249190933No ratings yet
- The SkullDocument14 pagesThe SkullChesca VerzNo ratings yet
- Ethanol Poisoning: Ethanol Poisoning Is Caused by Drinking Too Much AlcoholDocument11 pagesEthanol Poisoning: Ethanol Poisoning Is Caused by Drinking Too Much Alcohol0921pyNo ratings yet
- Potential Oral Health Effects of E-Cigarettes and Vaping: A Review and Case ReportsDocument5 pagesPotential Oral Health Effects of E-Cigarettes and Vaping: A Review and Case ReportsRares SuciaghiNo ratings yet
- 10 1093@jat@bkaa198Document11 pages10 1093@jat@bkaa198RaviTuduNo ratings yet
- Artificial Colors: ApprovedDocument2 pagesArtificial Colors: Approvedraviepic3No ratings yet
- Handsan-19 Gel MSDSDocument5 pagesHandsan-19 Gel MSDSpabianmarsNo ratings yet
- Household Cleaner Toxic ChemicalsDocument32 pagesHousehold Cleaner Toxic Chemicalsapi-264144691No ratings yet
- Usa Safety Data Sheet: LORD Corporation 111 LORD Drive Cary, NC 27511-7923 USADocument8 pagesUsa Safety Data Sheet: LORD Corporation 111 LORD Drive Cary, NC 27511-7923 USAJean Carlos MottaNo ratings yet
- Efficiency of Ethyl Alcohol in Treating Fungi Growth in White CheeseDocument10 pagesEfficiency of Ethyl Alcohol in Treating Fungi Growth in White CheeseCamille BattungNo ratings yet
- The Cosmetic Conspiracy - The Shocking Truth About The Ingredients in Your Cosmetic Products.Document9 pagesThe Cosmetic Conspiracy - The Shocking Truth About The Ingredients in Your Cosmetic Products.Cisco Balbontin100% (1)
- Xenoestrogens: Hidden Dangers in Our Modern World: 22 AdvancesDocument3 pagesXenoestrogens: Hidden Dangers in Our Modern World: 22 AdvancesNedoiu PaulNo ratings yet
- Types of Chemicals: PhthalatesDocument5 pagesTypes of Chemicals: PhthalatesMyerz YambaoNo ratings yet
- Dangerous Beauty The Chemical Evils in Personal Care Product - Group 9Document44 pagesDangerous Beauty The Chemical Evils in Personal Care Product - Group 9nova indah nurmalaNo ratings yet
- Emergency Poisoning FinalDocument81 pagesEmergency Poisoning FinalMohammed Gazo100% (2)
- Question: What Is A Toxic Chemical?: MicrofluidicDocument10 pagesQuestion: What Is A Toxic Chemical?: MicrofluidicFionna TamaraNo ratings yet
- Material Safety Data Sheet: 1. Product and Company IdentificationDocument11 pagesMaterial Safety Data Sheet: 1. Product and Company IdentificationEdmundo JmzNo ratings yet
- MSDS EtanolDocument9 pagesMSDS EtanolwynneralphNo ratings yet
- Chemlok 205Document8 pagesChemlok 205edwinsk9No ratings yet
- Vale 2016Document3 pagesVale 2016Hamida MidaNo ratings yet
- A Practical Approach To The Intoxicated ChildDocument6 pagesA Practical Approach To The Intoxicated ChildNatalia AlejandreNo ratings yet
- Letters To The Editor: Hand Eczema Due To Hygiene and Antisepsis Products: Not Only An Irritative EtiologyDocument2 pagesLetters To The Editor: Hand Eczema Due To Hygiene and Antisepsis Products: Not Only An Irritative Etiologysaka wibawaNo ratings yet
- Public Health England 1,2DE - TranslateDocument3 pagesPublic Health England 1,2DE - TranslateBari Noor RahmanNo ratings yet
- Running Head: HOME IS WHERE 1Document18 pagesRunning Head: HOME IS WHERE 1api-360135445No ratings yet
- How Safe Are WeDocument6 pagesHow Safe Are Weraju.setiawan.jaya.12No ratings yet
- 5 Hauptman M Childhood Ingestions of Environmental Toxins Pediatr Ann 2017 Dec 1Document7 pages5 Hauptman M Childhood Ingestions of Environmental Toxins Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet
- Aniline: Division of Toxicology Toxfaqs April 2002Document2 pagesAniline: Division of Toxicology Toxfaqs April 2002kareemNo ratings yet
- 1 Lowry JA Pediatric Ingestions Pediatr Ann 2017 Dec 1Document2 pages1 Lowry JA Pediatric Ingestions Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet
- J.P. Morgan Ventures Energy Corp. New York, NY 10017: 1. Product and Company IdentificationDocument8 pagesJ.P. Morgan Ventures Energy Corp. New York, NY 10017: 1. Product and Company Identificationbani.vallejosNo ratings yet
- 10 Dangerous Eveyday ThingsDocument5 pages10 Dangerous Eveyday ThingsniaagaraNo ratings yet
- 65 249 1 PBDocument4 pages65 249 1 PBJatin SinghNo ratings yet
- PDF 20230129 100015 0000Document20 pagesPDF 20230129 100015 0000dharen montecilloNo ratings yet
- Implement The Zero Garbage System at Domestic LevelDocument5 pagesImplement The Zero Garbage System at Domestic Levelsamar karemoreNo ratings yet
- Core PT 1 2014Document10 pagesCore PT 1 2014DigitalGeeksNo ratings yet
- Corona Seminar Mona EldesoukyDocument57 pagesCorona Seminar Mona Eldesoukykhaled eissaNo ratings yet
- Honey and LemonDocument7 pagesHoney and LemontangxiaomeimayNo ratings yet
- Presented by Malar Kodi. S M.SC (N) Ii Year DR - Syamala Reedy College of NursingDocument40 pagesPresented by Malar Kodi. S M.SC (N) Ii Year DR - Syamala Reedy College of NursingamulaathiNo ratings yet
- Personal Care ProductsDocument22 pagesPersonal Care ProductsalbinutaNo ratings yet
- 1017 12545 2 PBDocument8 pages1017 12545 2 PBmwnpvskgmbNo ratings yet
- Ethyl Alcohol vs. Isopropyl Alcohol - Uses and EffectivenessDocument13 pagesEthyl Alcohol vs. Isopropyl Alcohol - Uses and Effectivenessali rezaeiNo ratings yet
- 6 AntisepticsDocument22 pages6 AntisepticsDavid MharkNo ratings yet
- Material Safety Data Sheet: 1. Product and Company IdentificationDocument9 pagesMaterial Safety Data Sheet: 1. Product and Company IdentificationwjawichNo ratings yet
- Alcohol in CologneDocument5 pagesAlcohol in CologneKriserla Paula dela RosaNo ratings yet
- Msds - Di Ethylene GlycolDocument7 pagesMsds - Di Ethylene Glycolsales putrariNo ratings yet
- Chapter 1 To 5Document80 pagesChapter 1 To 5Patricia Belle LorenzoNo ratings yet
- Evaluación Cardiopulmonar Rápida PDFDocument83 pagesEvaluación Cardiopulmonar Rápida PDFDaniela JaramilloNo ratings yet
- Resuscitation Council - OVACEDocument12 pagesResuscitation Council - OVACEDaniela JaramilloNo ratings yet
- 5 Hauptman M Childhood Ingestions of Environmental Toxins Pediatr Ann 2017 Dec 1Document7 pages5 Hauptman M Childhood Ingestions of Environmental Toxins Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet
- 3 Quaal E Pediatric Poisonings - The Risk of Over-The-Counter Pharmaceuticals Pediatr Ann 2017 Dec 1Document6 pages3 Quaal E Pediatric Poisonings - The Risk of Over-The-Counter Pharmaceuticals Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet
- 4 Lowry JA Pediatric Pharmaceutical Ingestions Pediatr Ann 2017 Dec 1Document8 pages4 Lowry JA Pediatric Pharmaceutical Ingestions Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet
- 1 Lowry JA Pediatric Ingestions Pediatr Ann 2017 Dec 1Document2 pages1 Lowry JA Pediatric Ingestions Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet
- Insights Into The Thermo Mechanical Treatment of Brewers' Spent Grain As A Potential Filler For Polymer CompositesDocument18 pagesInsights Into The Thermo Mechanical Treatment of Brewers' Spent Grain As A Potential Filler For Polymer CompositesMaialen Espinal ViguriNo ratings yet
- Pentair Vessel and Skid RentalsDocument2 pagesPentair Vessel and Skid RentalsDian Purwa Dewa (Babeh)No ratings yet
- UploadFile 5041Document57 pagesUploadFile 5041Luiz Gustavo Santos AlbertoNo ratings yet
- الدليل الارشادي للنظافةDocument14 pagesالدليل الارشادي للنظافةKâtēbhÃłwešâbÿNo ratings yet
- Equilibrium and Le Chatelier'S Principle: Chemistry For Engineers - Laboratory Activity 6Document4 pagesEquilibrium and Le Chatelier'S Principle: Chemistry For Engineers - Laboratory Activity 6Moguri OwowNo ratings yet
- Supercritical Uid Extraction: Recent Advances and ApplicationsDocument17 pagesSupercritical Uid Extraction: Recent Advances and ApplicationsDAVID VLADIMIR ARRATEA PILLCONo ratings yet
- Peak Blue Diesel Exhaust Fluid (Def)Document2 pagesPeak Blue Diesel Exhaust Fluid (Def)Erick VargasNo ratings yet
- I. Photosynthesis (Light and Dark Reaction) : Quarter 2 / Semester 1, Week 2Document6 pagesI. Photosynthesis (Light and Dark Reaction) : Quarter 2 / Semester 1, Week 2Monica SolomonNo ratings yet
- 2020 10th Edition 10.0 Volume 2 EDocument1,329 pages2020 10th Edition 10.0 Volume 2 Edeepanmb007No ratings yet
- 2 25 Intermediate BondingDocument6 pages2 25 Intermediate BondingAliya RahmanNo ratings yet
- 4 Hour Fire Protection & Blast Protection SystemsDocument20 pages4 Hour Fire Protection & Blast Protection SystemssechooNo ratings yet
- 25 Zi-Chem 6320Document1 page25 Zi-Chem 6320Sigit SuryaNo ratings yet
- Catalytic Beds Protection: Procatalyse Catalysts & AdsorbentsDocument1 pageCatalytic Beds Protection: Procatalyse Catalysts & Adsorbentsmohsen ranjbarNo ratings yet
- Construction and Building Materials: E. Adamopoulou, P. Pipilikaki, M.S. Katsiotis, M. Chaniotakis, M. KatsiotiDocument8 pagesConstruction and Building Materials: E. Adamopoulou, P. Pipilikaki, M.S. Katsiotis, M. Chaniotakis, M. KatsiotiYane CoutinhoNo ratings yet
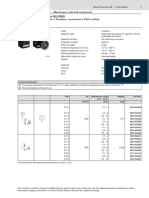
- Pressure Regulator, Series NL2-RGSDocument3 pagesPressure Regulator, Series NL2-RGSHuynh Duc TriNo ratings yet
- The National Academies PressDocument231 pagesThe National Academies PressCatalin SfatNo ratings yet
- Day 6 Welding Process, Electrode - FCAW, GTAW & SAWDocument65 pagesDay 6 Welding Process, Electrode - FCAW, GTAW & SAWRohit Kamble100% (1)
- The Composition of Jerusalem Artichoke (Helianthus Tuberosus L.) Spirits Obtained From Fermentation With Bacteria and YeastsDocument4 pagesThe Composition of Jerusalem Artichoke (Helianthus Tuberosus L.) Spirits Obtained From Fermentation With Bacteria and YeastsIoanaAndreeaNo ratings yet
- Lecture1 CH317 2020 Fall Statistics Part4 GGclasssDocument21 pagesLecture1 CH317 2020 Fall Statistics Part4 GGclasssshanicejames7867No ratings yet
- Gypsum ProductsDocument79 pagesGypsum ProductsSwati Pawar100% (1)
- How To Make Amrut JalDocument3 pagesHow To Make Amrut JalgreengrassglassNo ratings yet
- Engineered Regeneration: Tiffany Kim, Carmine Wang See, Xiaochun Li, Donghui ZhuDocument13 pagesEngineered Regeneration: Tiffany Kim, Carmine Wang See, Xiaochun Li, Donghui ZhuDamaris SoileNo ratings yet
- Polymers AssignmentDocument3 pagesPolymers AssignmentHari KotagiriNo ratings yet
- Laundry BasicsDocument16 pagesLaundry Basicsapi-494587938No ratings yet
- 3 Novec™ 1230 Fire Protection Fluid Data SheetDocument4 pages3 Novec™ 1230 Fire Protection Fluid Data SheetL ONo ratings yet
- APURBA - BISWASQuantitative Inorganic Practical2019-09-24SEM-1 - G - Practical Format - A.B SirDocument13 pagesAPURBA - BISWASQuantitative Inorganic Practical2019-09-24SEM-1 - G - Practical Format - A.B SirBernard ShamNo ratings yet
- Binders For: Architectural CoatingsDocument8 pagesBinders For: Architectural CoatingsAPEX SON100% (1)
- ICHEMDocument4 pagesICHEMAnthon ToledanoNo ratings yet
- Aspects of Lead Acid Battery Technology 6 Designing For Capacity PDFDocument43 pagesAspects of Lead Acid Battery Technology 6 Designing For Capacity PDFtjkiddNo ratings yet