Download as pdf or txt
You might also like
- Radiation Therapy of Benign DiseasesDocument355 pagesRadiation Therapy of Benign Diseasesyves2022sahaNo ratings yet
- Chapt 1 PeterDocument63 pagesChapt 1 PeterSamson PeterNo ratings yet
- Assignment On Occupational Health Hazards of Employees Working in Diagnostic Radiology DepartmentDocument15 pagesAssignment On Occupational Health Hazards of Employees Working in Diagnostic Radiology DepartmentkeerthanamsjNo ratings yet
- Health Risks From Exposure To Low Levels of Ionizing Radiation, Report in BriefDocument4 pagesHealth Risks From Exposure To Low Levels of Ionizing Radiation, Report in BriefNational Academies of Science, Engineering, and MedicineNo ratings yet
- Radiol 2021210665Document6 pagesRadiol 2021210665Camilo SotomayorNo ratings yet
- Misconceptions and Safety in Radiation OncologyDocument4 pagesMisconceptions and Safety in Radiation Oncologyapi-633248237No ratings yet
- Editorial: Breast Carcinogenesis: Risk of RadiationDocument3 pagesEditorial: Breast Carcinogenesis: Risk of RadiationGabriela Silva MartinsNo ratings yet
- Radiation-Related Risks of Imaging - UpToDateDocument28 pagesRadiation-Related Risks of Imaging - UpToDateCeleste MartinezNo ratings yet
- Effective Dose of Dental CBCT LudlowDocument25 pagesEffective Dose of Dental CBCT LudlowMaríaPazSalinasVillagraNo ratings yet
- Radiation Exposure and Cost Influence Physician Medical Image Decision MakingDocument5 pagesRadiation Exposure and Cost Influence Physician Medical Image Decision Makingكن صديقيNo ratings yet
- BJR 20219004Document4 pagesBJR 20219004Camilo SotomayorNo ratings yet
- Annotated BibliographyDocument10 pagesAnnotated BibliographyKrystal BowenNo ratings yet
- Radiation Saftey PaperDocument3 pagesRadiation Saftey Paperapi-692310570No ratings yet
- Jkms 31 S10Document14 pagesJkms 31 S10Aboalez NopliumNo ratings yet
- An Exploratory Analysis of Public Awareness and Perception To Ionzing RadiationDocument7 pagesAn Exploratory Analysis of Public Awareness and Perception To Ionzing RadiationD. IbanezNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptGeorge UngureanuNo ratings yet
- 1 s2.0 S1078817419301518 MainDocument6 pages1 s2.0 S1078817419301518 MainMiro SpiroNo ratings yet
- Radiation Safety Paper - Kristen DezellDocument4 pagesRadiation Safety Paper - Kristen Dezellapi-568316609No ratings yet
- Annotated 20bib 20app 20onc-2Document5 pagesAnnotated 20bib 20app 20onc-2api-309941992No ratings yet
- Projected Cancer Risks From Computed Tomographic Scans Performed in The United States in 2007Document7 pagesProjected Cancer Risks From Computed Tomographic Scans Performed in The United States in 2007CarlosNo ratings yet
- Articulo 1Document13 pagesArticulo 1Lucero BallesterosNo ratings yet
- App FDocument4 pagesApp Fmadhukara_raoNo ratings yet
- Cancers 13 05945Document16 pagesCancers 13 05945alfred31143No ratings yet
- Radiation Exposures in Medicine: Biological and Public Health SignificanceDocument13 pagesRadiation Exposures in Medicine: Biological and Public Health SignificanceFernando SperandioNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofIsmail Eko SaputraNo ratings yet
- NIH Public Access: Standardization and Optimization of Computed Tomography Protocols To Achieve Low-DoseDocument14 pagesNIH Public Access: Standardization and Optimization of Computed Tomography Protocols To Achieve Low-DoseMillerNo ratings yet
- Kei10344 FMDocument4 pagesKei10344 FMbbkanilNo ratings yet
- International Journal of Engineering Research and DevelopmentDocument8 pagesInternational Journal of Engineering Research and DevelopmentIJERDNo ratings yet
- Black Et Al 2024 The Role of Smoking Status in Making Risk Informed Diagnostic Decisions in The Lung Cancer Pathway ADocument11 pagesBlack Et Al 2024 The Role of Smoking Status in Making Risk Informed Diagnostic Decisions in The Lung Cancer Pathway AYulia Niswatul FauziyahNo ratings yet
- A 0240105Document5 pagesA 0240105International Organization of Scientific Research (IOSR)No ratings yet
- Chapter OneDocument7 pagesChapter OneJerome WunujiNo ratings yet
- CBCT Dosimetry: Orthodontic ConsiderationsDocument5 pagesCBCT Dosimetry: Orthodontic Considerationsgriffone1No ratings yet
- European Journal of Radiology: M Kiani, A ChaparianDocument7 pagesEuropean Journal of Radiology: M Kiani, A ChaparianHamza ArjahNo ratings yet
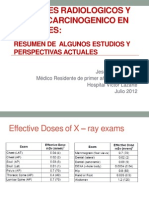
- Examenes Radiologicos y Riesgo de Cancer en PacientesDocument27 pagesExamenes Radiologicos y Riesgo de Cancer en PacientesMaría Isabel Clara Aponte OrtizNo ratings yet
- 19-109 Putri Amalia CSS Radiologi PDFDocument20 pages19-109 Putri Amalia CSS Radiologi PDFPutri AmaliaNo ratings yet
- Current Issues and Actions in Radiation Protection of PatientsDocument5 pagesCurrent Issues and Actions in Radiation Protection of PatientsSusryandini NovraswindaNo ratings yet
- Nuclear Medicine Therapy: Principles and Clinical ApplicationsFrom EverandNuclear Medicine Therapy: Principles and Clinical ApplicationsNo ratings yet
- Tugas Ibu RetinoblastomaDocument7 pagesTugas Ibu RetinoblastomamalaNo ratings yet
- BJR 20210389Document10 pagesBJR 20210389Camilo SotomayorNo ratings yet
- CBCT Dosimetry Orthodontic ConsiderationsDocument5 pagesCBCT Dosimetry Orthodontic ConsiderationsElzaMMartinsNo ratings yet
- Radiation Benefit and Risk Assessment: Risk Observable Health Effect SafeDocument7 pagesRadiation Benefit and Risk Assessment: Risk Observable Health Effect SafeLancerNo ratings yet
- Epidemiologic Studies of Carcinogenesis by Ionizing RadiationDocument43 pagesEpidemiologic Studies of Carcinogenesis by Ionizing RadiationTroy LivingstonNo ratings yet
- Jurnal Prognosis Radiologi 1Document9 pagesJurnal Prognosis Radiologi 1Henry WijayaNo ratings yet
- Health Effects From Exposure To Dental Diagnostic X-Ray: Environmental Health and ToxicologyDocument6 pagesHealth Effects From Exposure To Dental Diagnostic X-Ray: Environmental Health and ToxicologyhelmysiswantoNo ratings yet
- Solar Radiation and The Incidence and Mortality of Leading Invasive Cancers in The United StatesDocument7 pagesSolar Radiation and The Incidence and Mortality of Leading Invasive Cancers in The United StatesMBNo ratings yet
- Protection From RadiationDocument8 pagesProtection From Radiationapi-270822363No ratings yet
- Tecnicas Imagenelogicas CancerDocument8 pagesTecnicas Imagenelogicas CancerFranNo ratings yet
- 6 - Cancer Risk in 680 000 People Exposed To Computed Tomography Scans in Childhood or Adolescence - Data Linkage Study of 11 Million AustraliansDocument18 pages6 - Cancer Risk in 680 000 People Exposed To Computed Tomography Scans in Childhood or Adolescence - Data Linkage Study of 11 Million AustraliansEdis DjedovicNo ratings yet
- The Safe Use of RadiationDocument5 pagesThe Safe Use of Radiationapi-710804215No ratings yet
- NexusDocument6 pagesNexusAzmi FarhadiNo ratings yet
- Analysis of Cancer Risks in Populations Near Nuclear FacilitiesDocument4 pagesAnalysis of Cancer Risks in Populations Near Nuclear FacilitiesNational Academies of Science, Engineering, and MedicineNo ratings yet
- A Tutorial On Diagnostic Benefit and Radiation Risk in Videofluoroscopic Swallowing StudiesDocument26 pagesA Tutorial On Diagnostic Benefit and Radiation Risk in Videofluoroscopic Swallowing StudiesMarcia Peña SilvaNo ratings yet
- Rad EyesDocument5 pagesRad Eyeshi_landsNo ratings yet
- Soal No 2Document9 pagesSoal No 2Muhammad Syaifuddin FuadNo ratings yet
- Safety of Radiographic Imaging During Pregnancy - American Family PhysicianDocument7 pagesSafety of Radiographic Imaging During Pregnancy - American Family PhysicianDuddy Ari HardiantoNo ratings yet
- Lit Review DraftDocument6 pagesLit Review DraftKrystal BowenNo ratings yet
- Relationship Between Radiation Exposure and Study Habits Among Grade 12 Stem StudentsDocument22 pagesRelationship Between Radiation Exposure and Study Habits Among Grade 12 Stem StudentsAaron Francis LumayagNo ratings yet
- Neuroimaging in Pregnant WomenDocument12 pagesNeuroimaging in Pregnant WomenInes StrenjaNo ratings yet
- Imaging in Pediatric OncologyFrom EverandImaging in Pediatric OncologyStephan D. VossNo ratings yet
- Predicting Creativity: Interactive Effects of Openness To Experience and Emotion Regulation AbilityDocument8 pagesPredicting Creativity: Interactive Effects of Openness To Experience and Emotion Regulation Abilitynoah0firthNo ratings yet
- VAC Form 1Document1 pageVAC Form 1Angela TabudlongNo ratings yet
- Developmental AssessmentDocument5 pagesDevelopmental AssessmentSamwel KangyNo ratings yet
- Shoulder DystociaDocument3 pagesShoulder Dystociakarl de guzmanNo ratings yet
- HorribleWounds PosterDocument1 pageHorribleWounds PosterNfikf100% (1)
- Medical SpecialistDocument9 pagesMedical SpecialistDhiya MaralinNo ratings yet
- COVID 19 Risk Assessment Form Restaurants Offering Takeaway or Delivery June 2020Document4 pagesCOVID 19 Risk Assessment Form Restaurants Offering Takeaway or Delivery June 2020muhammad sandriyanNo ratings yet
- Pollution Prevention Management Plan MajorDocument30 pagesPollution Prevention Management Plan MajorAlbatool ElsayedNo ratings yet
- Project On Analysis of Attitude of Pregnant Mother Towards Antenatal Care ServiceDocument50 pagesProject On Analysis of Attitude of Pregnant Mother Towards Antenatal Care ServiceYUSUF AMINUNo ratings yet
- 40 Series Tractor ServiceDocument51 pages40 Series Tractor ServiceAllanaDm50% (2)
- Version Structures and Functions of Living Organisms 8.L.1.1Document28 pagesVersion Structures and Functions of Living Organisms 8.L.1.1Marianna HernandezNo ratings yet
- Psychedelics, Technology, Psychedelics: Bernard S. Aaronson and Humphrey OsmondDocument8 pagesPsychedelics, Technology, Psychedelics: Bernard S. Aaronson and Humphrey OsmondJuan ScuroNo ratings yet
- Thyroid QuizDocument3 pagesThyroid QuizĐặng Quỳnh ANNo ratings yet
- Metabolic and Complicated Cataract: DR - Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS, RishikeshDocument31 pagesMetabolic and Complicated Cataract: DR - Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS, Rishikeshsai shantanu100% (1)
- Neurourology and Urodynamics - 2023 - Demirci - Which Type of Female Urinary Incontinence Has More Impact On Pelvic FloorDocument8 pagesNeurourology and Urodynamics - 2023 - Demirci - Which Type of Female Urinary Incontinence Has More Impact On Pelvic FloorYo MeNo ratings yet
- Air Water Land Noise Pollution Information and PicsDocument10 pagesAir Water Land Noise Pollution Information and PicsHarendra Yadav100% (3)
- Malunggay With MagnetDocument13 pagesMalunggay With MagnetMarlon Sta. CatalinaNo ratings yet
- Larvicidal Activity of Anacardium Occidental Against Aedes Aegypti FINALDocument5 pagesLarvicidal Activity of Anacardium Occidental Against Aedes Aegypti FINALVernice OrtegaNo ratings yet
- Principles of Fixed Implant ProsthodonticsDocument6 pagesPrinciples of Fixed Implant ProsthodonticsManar Abu ShadyNo ratings yet
- Shallow and Flat Anterior ChamberDocument8 pagesShallow and Flat Anterior Chamberjudah samuelNo ratings yet
- Mindfulness For Exams by Ashley LodgeDocument2 pagesMindfulness For Exams by Ashley Lodgepetit_19794618No ratings yet
- Women's Era TP August 2021Document116 pagesWomen's Era TP August 2021NancyShahNo ratings yet
- Weekly Activity Report: Number of AttendeesDocument7 pagesWeekly Activity Report: Number of AttendeestabilinNo ratings yet
- Binge Anxiety Killer Cheat Sheet: InstructionsDocument4 pagesBinge Anxiety Killer Cheat Sheet: Instructionsdoppler_No ratings yet
- PHS809 Social MedicineDocument153 pagesPHS809 Social MedicineMiyNo ratings yet
- Price List September 2022Document61 pagesPrice List September 2022Ade IrawanNo ratings yet
- ACC Social Media Hashtag Reference GuideDocument12 pagesACC Social Media Hashtag Reference Guidealfredomeli2008No ratings yet
- Maskote WB Zinc Stop-OffDocument7 pagesMaskote WB Zinc Stop-OffbondsivamaniNo ratings yet
- Guideline On Drug Registration Application in Myanmar - 2014Document51 pagesGuideline On Drug Registration Application in Myanmar - 2014Kush MukherjiNo ratings yet
- Cloud NineDocument6 pagesCloud NineJunjun CaoliNo ratings yet