Download as pdf or txt
You might also like
- Case Write Up-DengueDocument16 pagesCase Write Up-DengueSyafi'ie Syukri100% (1)
- Angio Displa SiaDocument4 pagesAngio Displa SiaBelaFawziaNo ratings yet
- Webb 2641Document12 pagesWebb 2641owcordal7297No ratings yet
- Spondilita Ankilozanta Cardio PulmonarDocument6 pagesSpondilita Ankilozanta Cardio PulmonarGiulia LungulescuNo ratings yet
- Section 5. Atherosclerotic Peripheral Vascular Disease and Aortic AneurysmDocument23 pagesSection 5. Atherosclerotic Peripheral Vascular Disease and Aortic AneurysmsidoniavidicanNo ratings yet
- An Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystDocument3 pagesAn Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystAgus PrimaNo ratings yet
- Colonic Ischemia - UpToDateDocument35 pagesColonic Ischemia - UpToDateWitor BelchiorNo ratings yet
- Valvular Disease in The Elderly: DavidDocument22 pagesValvular Disease in The Elderly: DavidThanh BinhNo ratings yet
- Uppergastrointestinalbleeding: Marcie Feinman,, Elliott R. HautDocument11 pagesUppergastrointestinalbleeding: Marcie Feinman,, Elliott R. HautjoseNo ratings yet
- Ascitis ImportanteDocument17 pagesAscitis Importantedanyescalerapumas24No ratings yet
- Guidelines: Management of Stable Angina PectorisDocument20 pagesGuidelines: Management of Stable Angina PectorisDelvina TandiariNo ratings yet
- Preprints202307 1050 v1Document12 pagesPreprints202307 1050 v1Mihai PopescuNo ratings yet
- Portal HypertensionDocument13 pagesPortal HypertensionCiprian BoesanNo ratings yet
- Diseases of The SmalllntestineDocument183 pagesDiseases of The SmalllntestineIgor CemortanNo ratings yet
- Lancet 2016 Valvulopatias Estenosis AórticaDocument12 pagesLancet 2016 Valvulopatias Estenosis AórticaSol LakosNo ratings yet
- Aortoiliac Occlusive DiseaseDocument37 pagesAortoiliac Occlusive Diseasewolff_512No ratings yet
- Cecum Dieulafoy's Lesion Presenting With Recurrent Lower Gastrointestinal Bleeding: Case ReportDocument5 pagesCecum Dieulafoy's Lesion Presenting With Recurrent Lower Gastrointestinal Bleeding: Case ReportSabrina JonesNo ratings yet
- Vasculitis PDFDocument4 pagesVasculitis PDFDiego Ariel Alarcón SeguelNo ratings yet
- Aortic Calcium Score and Vascular Atherosclerosis in Asymptomatic Individuals: Beyond The Coronary ArteriesDocument4 pagesAortic Calcium Score and Vascular Atherosclerosis in Asymptomatic Individuals: Beyond The Coronary ArteriesAdriana VasilicaNo ratings yet
- 97managementstable AnginaDocument20 pages97managementstable AnginaTambunta TariganNo ratings yet
- AscitesascitesDocument15 pagesAscitesascitesKevinJuliusTanadyNo ratings yet
- Mallory Weiss Syndrome - StatPearls - NCBI BookshelfDocument9 pagesMallory Weiss Syndrome - StatPearls - NCBI BookshelfDaniela EstradaNo ratings yet
- Guidelines: Management of Stable Angina PectorisDocument20 pagesGuidelines: Management of Stable Angina PectorisyudaNo ratings yet
- Cirrosis LANCET 2008Document14 pagesCirrosis LANCET 2008Natalia ElizabethNo ratings yet
- Seminar: Detlef Schuppan, Nezam H AfdhalDocument14 pagesSeminar: Detlef Schuppan, Nezam H AfdhalJonathan Arif PutraNo ratings yet
- Eisenmenger SyndromeDocument9 pagesEisenmenger SyndromesyifandikaNo ratings yet
- Chapter (2) Coronary Artery EctasiaDocument19 pagesChapter (2) Coronary Artery Ectasiahussien abd elwahedNo ratings yet
- Arterial Hypertension and Aortic Valve Stenosis: Shedding Light On A Common "Liaison"Document6 pagesArterial Hypertension and Aortic Valve Stenosis: Shedding Light On A Common "Liaison"Adriana VasilicaNo ratings yet
- Peripheral Arterial Disease: AbnetDocument142 pagesPeripheral Arterial Disease: AbnetAbnet WondimuNo ratings yet
- Aneurysmal Disease - Thoracic AortaDocument18 pagesAneurysmal Disease - Thoracic AortaEmmanuel BarriosNo ratings yet
- Vascular Disease of The BowelDocument28 pagesVascular Disease of The BowelOlga GoryachevaNo ratings yet
- Leg UlcersDocument14 pagesLeg UlcersNovi Y'uZzmanNo ratings yet
- Lower Gastrointestinal BleedingDocument18 pagesLower Gastrointestinal Bleedingosama nawaysehNo ratings yet
- 4.1 Bicuspid Aortic ValveDocument33 pages4.1 Bicuspid Aortic ValveAbnet WondimuNo ratings yet
- Aortic StenosisDocument134 pagesAortic StenosisAbnet WondimuNo ratings yet
- WJG 13 2693Document4 pagesWJG 13 2693aalmadasalazarNo ratings yet
- Me DCL Inn Avarice Al BleedingDocument24 pagesMe DCL Inn Avarice Al BleedingKarina WibowoNo ratings yet
- VASCULITIS by Dr. AJ. 1Document34 pagesVASCULITIS by Dr. AJ. 1Abira KhanNo ratings yet
- Robertson 2017Document10 pagesRobertson 2017tnsourceNo ratings yet
- Varices: Esophageal, Gastric, and RectalDocument18 pagesVarices: Esophageal, Gastric, and RectalHưng Nguyễn KiềuNo ratings yet
- Acute GI BleedingDocument13 pagesAcute GI BleedingDavid RyanNo ratings yet
- Brief: Hemolytic Uremic SyndromeDocument5 pagesBrief: Hemolytic Uremic SyndromeMaria Esther JimenezNo ratings yet
- 1 s2.0 S1365182X15303518 MainDocument14 pages1 s2.0 S1365182X15303518 Mainprasanna1047No ratings yet
- Diagnosis and Management of Splanchnic Ischemia: Ioannis E Koutroubakis, MD, PHD, Assistant Professor of MedicineDocument12 pagesDiagnosis and Management of Splanchnic Ischemia: Ioannis E Koutroubakis, MD, PHD, Assistant Professor of MedicineIgorCotagaNo ratings yet
- Management of Chronic Venous Disease: 7th Annual Women's Heart & Vascular SymposiumDocument3 pagesManagement of Chronic Venous Disease: 7th Annual Women's Heart & Vascular Symposiumatika5No ratings yet
- Jurnal 5Document6 pagesJurnal 5Siti rahmi AbukhaerNo ratings yet
- PMR and TADocument11 pagesPMR and TAハルァン ファ烏山No ratings yet
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocument9 pages2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluNo ratings yet
- Journal of Cardiac Surgery - 2022 - Kayali - Coronary Artery Involvement in Type A Aortic Dissection Fate of TheDocument10 pagesJournal of Cardiac Surgery - 2022 - Kayali - Coronary Artery Involvement in Type A Aortic Dissection Fate of Theandus007No ratings yet
- Sickle Cell Disease: A Paradigm For Venous Thrombosis PathophysiologyDocument20 pagesSickle Cell Disease: A Paradigm For Venous Thrombosis PathophysiologyMuhammad SaeedNo ratings yet
- Colitis Isquemica PDFDocument7 pagesColitis Isquemica PDFWaldo ReyesNo ratings yet
- A SC Ites: Diagnosis Andmanagement: Wei Hou,, Arun J. SanyalDocument17 pagesA SC Ites: Diagnosis Andmanagement: Wei Hou,, Arun J. SanyalNicole Zavaleta VelásquezNo ratings yet
- Upper Gastrointestinal Bleeding (UGIB) : Practice EssentialsDocument52 pagesUpper Gastrointestinal Bleeding (UGIB) : Practice EssentialsrishaNo ratings yet
- Esophageal Varices - Part I: Pathophysiology, Diagnostics, Conservative Treatment and Prevention of BleedingDocument8 pagesEsophageal Varices - Part I: Pathophysiology, Diagnostics, Conservative Treatment and Prevention of BleedingSesilia RosaNo ratings yet
- Vasculer Anomly of IntestineDocument38 pagesVasculer Anomly of Intestineعبد الله مازن موسى عبدNo ratings yet
- Cho 2002Document7 pagesCho 2002DanteNo ratings yet
- Haemostatic Alterations and Management of HaemostaDocument15 pagesHaemostatic Alterations and Management of HaemostaCláudia SilvaNo ratings yet
- Aortic Stenosis: History & ExamDocument36 pagesAortic Stenosis: History & ExamMicija CucuNo ratings yet
- Endothelium-Mediated Coronary Blood Flow Modulation in Humans. Effects of Age, Atherosclerosis, Hypercholesterolemia, and HypertensionDocument12 pagesEndothelium-Mediated Coronary Blood Flow Modulation in Humans. Effects of Age, Atherosclerosis, Hypercholesterolemia, and HypertensionAnis RanisNo ratings yet
- Comprehensive Insights into Acute Arterial Occlusion: Pathways, Prevention, and Holistic CareFrom EverandComprehensive Insights into Acute Arterial Occlusion: Pathways, Prevention, and Holistic CareNo ratings yet
- Advancements in Acute Aortic Syndrome: From Pathophysiology to Personalized TherapeuticsFrom EverandAdvancements in Acute Aortic Syndrome: From Pathophysiology to Personalized TherapeuticsNo ratings yet
- A Scoring System For Prediction and Risk Stratification of Co2 Narcosis 216Document5 pagesA Scoring System For Prediction and Risk Stratification of Co2 Narcosis 216Abdi KebedeNo ratings yet
- Paediatric Respiratory Medicine: Key PointsDocument8 pagesPaediatric Respiratory Medicine: Key PointsAbdi KebedeNo ratings yet
- Good Luck: Addis Ababa University, Medical Faculty, Dept. of SurgeryDocument21 pagesGood Luck: Addis Ababa University, Medical Faculty, Dept. of SurgeryAbdi KebedeNo ratings yet
- Unique Features of Infective Endocarditis in Childhood: AHA Scientific StatementDocument13 pagesUnique Features of Infective Endocarditis in Childhood: AHA Scientific StatementAbdi KebedeNo ratings yet
- Grand Rounds: Indications For LP Following 1st Febrile Seizure ReconsideredDocument3 pagesGrand Rounds: Indications For LP Following 1st Febrile Seizure ReconsideredAbdi KebedeNo ratings yet
- Recommendations For Term and Late Preterm Infants at Risk For Perinatal Bacterial InfectionDocument5 pagesRecommendations For Term and Late Preterm Infants at Risk For Perinatal Bacterial InfectionAbdi KebedeNo ratings yet
- Strong Children'S Research Center: Name: Andrew Duffy School: University of Rochester Mentor: Heidi Connolly, M.DDocument1 pageStrong Children'S Research Center: Name: Andrew Duffy School: University of Rochester Mentor: Heidi Connolly, M.DAbdi KebedeNo ratings yet
- 2017 Hinkle AbstractDocument1 page2017 Hinkle AbstractAbdi KebedeNo ratings yet
- ISPAD Clinical Practice Consensus Guidelines 2018: Management of Children and Adolescents With Diabetes Requiring SurgeryDocument10 pagesISPAD Clinical Practice Consensus Guidelines 2018: Management of Children and Adolescents With Diabetes Requiring SurgeryAbdi KebedeNo ratings yet
- October 2017 Ed Infant Fever 29-60 DaysDocument4 pagesOctober 2017 Ed Infant Fever 29-60 DaysAbdi KebedeNo ratings yet
- 2018 Article 3382Document6 pages2018 Article 3382Abdi KebedeNo ratings yet
- The Insect State: Development, Politics and Capital in African Desert Locust ControlDocument3 pagesThe Insect State: Development, Politics and Capital in African Desert Locust ControlAbdi KebedeNo ratings yet
- B-Cell Function and Thyroid Dysfunction: A Cross-Sectional StudyDocument8 pagesB-Cell Function and Thyroid Dysfunction: A Cross-Sectional StudyAbdi KebedeNo ratings yet
- Abdi Seminar On Updates of SAMDocument74 pagesAbdi Seminar On Updates of SAMAbdi KebedeNo ratings yet
- Injury Biomechanics: AAMIR SOHAIL - Student ID 163101039 - December 16, 2016Document12 pagesInjury Biomechanics: AAMIR SOHAIL - Student ID 163101039 - December 16, 2016Aamir SohailNo ratings yet
- A170566 Study Report BodyDocument79 pagesA170566 Study Report BodyAnonymous yqRB5cVMeNo ratings yet
- Table Tennis Lesson PlanDocument3 pagesTable Tennis Lesson Planapi-216084231No ratings yet
- Bod+cod Statistici MARSDocument16 pagesBod+cod Statistici MARSandreiNo ratings yet
- Clamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)Document5 pagesClamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)rizwan900No ratings yet
- Omonigbehin Emmanuel AdedayoDocument12 pagesOmonigbehin Emmanuel AdedayoAriel GhieNo ratings yet
- IELTS Writing Task 2 Samples (WWW - Luckyielts.com) PDFDocument648 pagesIELTS Writing Task 2 Samples (WWW - Luckyielts.com) PDFMinh NgọcNo ratings yet
- Humanitarians in The Face of Atrocities: Case Studies: Syria and CARDocument19 pagesHumanitarians in The Face of Atrocities: Case Studies: Syria and CARMigs MontrealNo ratings yet
- Phenotypic and Molecular Characterizations OF: Salmonella Species in EthiopiaDocument194 pagesPhenotypic and Molecular Characterizations OF: Salmonella Species in EthiopiaAmid CapmariNo ratings yet
- Readings On Human Development of NepalDocument310 pagesReadings On Human Development of NepalBirkha B PunNo ratings yet
- Daftar Obat %pareto Dan Ven 15Document200 pagesDaftar Obat %pareto Dan Ven 15sofia nofiantiNo ratings yet
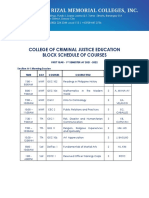
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- Qdoc - Tips - Prometric Practice Exam For Nurses Test 1Document6 pagesQdoc - Tips - Prometric Practice Exam For Nurses Test 1Ponnudev100% (1)
- Which of The Following Is NOT True About Dust?Document3 pagesWhich of The Following Is NOT True About Dust?lucel palaca100% (1)
- ANALISIS PENERAPAN SISTEM LOCKOUTTAGOUT (LOTO) PADA BAGIAN OPERASI DAN PEMELIHARAAN DI PT. X TANJUNG EMAS KOTA SEMARANG (Berdasarkan Standar OSHA 29 CFR Part 1910.147 Dan Part 1910.333) PDFDocument11 pagesANALISIS PENERAPAN SISTEM LOCKOUTTAGOUT (LOTO) PADA BAGIAN OPERASI DAN PEMELIHARAAN DI PT. X TANJUNG EMAS KOTA SEMARANG (Berdasarkan Standar OSHA 29 CFR Part 1910.147 Dan Part 1910.333) PDFAfif Fayadh VictoryNo ratings yet
- Bilal Ahmad Khan CVDocument2 pagesBilal Ahmad Khan CVfr.faisal8265No ratings yet
- Sydenham's ChoreaDocument11 pagesSydenham's ChoreaKosi UdohNo ratings yet
- Mutagenèse Et Cancérogenèse: Gwenaëlle IarmarcovaiDocument10 pagesMutagenèse Et Cancérogenèse: Gwenaëlle Iarmarcovaibouchakour meryemNo ratings yet
- Manual CabinaDocument20 pagesManual CabinaCintexNo ratings yet
- Chun-Hung Chen Kun-Cheng ChouDocument38 pagesChun-Hung Chen Kun-Cheng ChoutwnationNo ratings yet
- Vocabulary Set 28 - TAX ON FAST FOODDocument4 pagesVocabulary Set 28 - TAX ON FAST FOODchung hieuNo ratings yet
- ACTIVITY Psychological First Aid PFADocument25 pagesACTIVITY Psychological First Aid PFAChristine DianeNo ratings yet
- Jsa For Radiography WorkDocument2 pagesJsa For Radiography WorkVipul ShankarNo ratings yet
- The Microskills ApproachDocument2 pagesThe Microskills ApproachTatiana Buianina0% (1)
- Dental MaterialsDocument11 pagesDental MaterialsShweta RangharNo ratings yet
- Manifesting Generators - Resources For LifeDocument3 pagesManifesting Generators - Resources For LifeIrem YitmenNo ratings yet
- Language Disorders - 5Document27 pagesLanguage Disorders - 5Marta Sampedro GonzalezNo ratings yet
- Alcohal DependenceDocument17 pagesAlcohal DependenceViky SinghNo ratings yet
- Isolated Third Nerve PalsyDocument4 pagesIsolated Third Nerve PalsySora KerovaNo ratings yet