
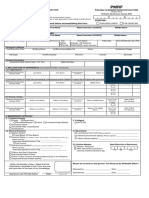
Claims Forms Mediplus Claim Intimation Form - PDF 225bfd110e PDF
Claims Forms Mediplus Claim Intimation Form - PDF 225bfd110e PDF
You might also like
- Zitra Personal Account FormDocument2 pagesZitra Personal Account FormUgo BenNo ratings yet
- Exercises/Problems:) R 1 (Ue Termnalval VCF) R 1 (VCF) R 1 (VCF) R 1 (VCF) R 1 (VCFDocument1 pageExercises/Problems:) R 1 (Ue Termnalval VCF) R 1 (VCF) R 1 (VCF) R 1 (VCF) R 1 (VCFIT manNo ratings yet
- Insular Life Insurance FormDocument2 pagesInsular Life Insurance FormEarl Cortez0% (1)
- PNB Customer Information Form IndividualDocument1 pagePNB Customer Information Form IndividualBrittaney BatoNo ratings yet
- Supply Chain ChallengesDocument2 pagesSupply Chain ChallengesAneek RasmomNo ratings yet
- HSP - ClaimForm - New AddressDocument3 pagesHSP - ClaimForm - New AddresssandeepNo ratings yet
- Patient InformationDocument1 pagePatient InformationsmartsportsNo ratings yet
- BM Umbrella Retirement Scheme Member Application Form-EDocument3 pagesBM Umbrella Retirement Scheme Member Application Form-ExeniaNo ratings yet
- Claim FormDocument4 pagesClaim Formsrirama.guttaNo ratings yet
- ALAT Account Customer Update FormDocument1 pageALAT Account Customer Update FormJamiu JabaruNo ratings yet
- Additional Applicant Form: Personal DetailsDocument2 pagesAdditional Applicant Form: Personal DetailsAlhassan EmmanuelNo ratings yet
- RBD - Common Retail Loan Application Form Co - ApplicantDocument2 pagesRBD - Common Retail Loan Application Form Co - Applicantr_awadhiyaNo ratings yet
- Individual Application Form For Registration of Dependants V302 20220302 InteractiveDocument8 pagesIndividual Application Form For Registration of Dependants V302 20220302 InteractiveTsundzuka KhosaNo ratings yet
- Nomination Form: (For Registering A Nominee or Cancelling An Existing Nomination)Document2 pagesNomination Form: (For Registering A Nominee or Cancelling An Existing Nomination)MailNo ratings yet
- Form For Nomination / Appointee Addition: General InformationDocument2 pagesForm For Nomination / Appointee Addition: General InformationSonu SinghNo ratings yet
- Common Retail Loan Application Form For GuarantorDocument2 pagesCommon Retail Loan Application Form For GuarantorNukamreddy Venkateswara ReddyNo ratings yet
- Home Loan Application FormDocument9 pagesHome Loan Application FormSachin KmNo ratings yet
- Revised - AL Form - Document - MITC PDFDocument10 pagesRevised - AL Form - Document - MITC PDFVijayNo ratings yet
- AL Form Document MITCDocument9 pagesAL Form Document MITCRamyaSathyanathanNo ratings yet
- D D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration FormDocument7 pagesD D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration Formdharam singhNo ratings yet
- Application For ServicesDocument4 pagesApplication For ServicesNermeen ElsayedNo ratings yet
- Application Form PDFDocument4 pagesApplication Form PDFTushar RathoreNo ratings yet
- Philhealth - Pag-Ibig MibDocument8 pagesPhilhealth - Pag-Ibig MibChino PaciaNo ratings yet
- Customer Information Update Form: Account DetailsDocument1 pageCustomer Information Update Form: Account DetailsDolapo OlukotunNo ratings yet
- Synchronized Predeployment & Operational Tracker (Spot) : Request For Letter of AuthorizationDocument1 pageSynchronized Predeployment & Operational Tracker (Spot) : Request For Letter of AuthorizationRham OnbenchNo ratings yet
- Individual Personal Accident Insurance Claim FormDocument3 pagesIndividual Personal Accident Insurance Claim FormSatyaNo ratings yet
- FOIA'd Police Report of Tara Durant's 911 CallDocument12 pagesFOIA'd Police Report of Tara Durant's 911 Calljen_benderyNo ratings yet
- Loan Application Form: Applicant Co-ApplicantDocument4 pagesLoan Application Form: Applicant Co-ApplicantStatus SambavanghalNo ratings yet
- Emp Bus SPC AirportsDocument1 pageEmp Bus SPC AirportsShami MudunkotuwaNo ratings yet
- Sbi Home Loans Application FormDocument5 pagesSbi Home Loans Application FormHimanshu AshwiniNo ratings yet
- IPA Claim FormDocument5 pagesIPA Claim FormVivek ChopraNo ratings yet
- Information Form: Maldives Islamic BankDocument5 pagesInformation Form: Maldives Islamic BankyrafeeuNo ratings yet
- MSME Loan Application Form - Partnership - 1 PagerDocument2 pagesMSME Loan Application Form - Partnership - 1 Pagernambi2rajanNo ratings yet
- Group Personal Accident-Claim FormDocument4 pagesGroup Personal Accident-Claim FormVipul SharmaNo ratings yet
- Adr 2Document2 pagesAdr 2ok2bwellNo ratings yet
- New Format Application Form CLRDocument8 pagesNew Format Application Form CLRtheonelNo ratings yet
- Tax Client QuestionaireDocument3 pagesTax Client QuestionaireCory100% (1)
- Position Applied For: Other Position(s) of Interest: Salary Expected: (Net/ Gross) Date Available To StartDocument4 pagesPosition Applied For: Other Position(s) of Interest: Salary Expected: (Net/ Gross) Date Available To StartalfathNo ratings yet
- Patient Demographics FormDocument1 pagePatient Demographics FormChynta Adilla AdillaNo ratings yet
- Congi Application FormDocument6 pagesCongi Application Formsharathkumarreddy2021No ratings yet
- Pis SignDocument1 pagePis SignJoshua RuizNo ratings yet
- (Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanDocument2 pages(Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanKristian Romeo NapiñasNo ratings yet
- Update Info FormDocument1 pageUpdate Info FormEsan BiolaNo ratings yet
- Personal Information (Amended)Document3 pagesPersonal Information (Amended)TANU SINGHNo ratings yet
- Agency/Person Information: OSS Amage EportDocument1 pageAgency/Person Information: OSS Amage EportClarenceJoy Ferrer Dela CruzNo ratings yet
- JMT HR - Form 003 v1 - New Employee Information FormDocument1 pageJMT HR - Form 003 v1 - New Employee Information FormMaral Inocencio AltarNo ratings yet
- FIR Form PunjabDocument1 pageFIR Form PunjabSanjiv KumarNo ratings yet
- PMRF RevisedDocument2 pagesPMRF RevisedDBVS GRAY MORTERANo ratings yet
- Public Liability Claim Form EngDocument1 pagePublic Liability Claim Form EngVeron AcNo ratings yet
- 18 Account Opening FormDocument11 pages18 Account Opening Formhl2225742No ratings yet
- Steps Forward Patient DemographicsDocument3 pagesSteps Forward Patient DemographicsdawnNo ratings yet
- Page Loan FormDocument2 pagesPage Loan FormChukwuemeka Great NwankwoNo ratings yet
- Home Loans Application: First National Bank Ghana Limited, A Subsidiary of Firstrand Group, South AfricaDocument12 pagesHome Loans Application: First National Bank Ghana Limited, A Subsidiary of Firstrand Group, South Africazirri23No ratings yet
- Nomination Form PLIDocument2 pagesNomination Form PLIGeethanjali RajanalaNo ratings yet
- TERC HR - Form 003 v1 - New Employee Information FormDocument1 pageTERC HR - Form 003 v1 - New Employee Information FormMaral Inocencio AltarNo ratings yet
- Employee Information Form 06Document3 pagesEmployee Information Form 06Dave PagaraNo ratings yet
- Children Policy ProposalDocument4 pagesChildren Policy ProposalNitin KumarNo ratings yet
- ERISA/Non-ERISA - Change of Beneficiary/ Spousal Consent: SECTION 1: Participant InformationDocument5 pagesERISA/Non-ERISA - Change of Beneficiary/ Spousal Consent: SECTION 1: Participant InformationandryNo ratings yet
- Prepaid Card Application Form: 1. Personal InformationDocument9 pagesPrepaid Card Application Form: 1. Personal InformationcharmainejalaNo ratings yet
- Patient Intatke FormsDocument3 pagesPatient Intatke FormsBryan KiddNo ratings yet
- Please Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeDocument2 pagesPlease Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeMosses BryanNo ratings yet
- CamScanner 10-17-2020 16.26.25 PDFDocument9 pagesCamScanner 10-17-2020 16.26.25 PDFNamasteNo ratings yet
- Claims Forms Auto Secure Private Car Twowheeler - PDF 42898fa34f PDFDocument2 pagesClaims Forms Auto Secure Private Car Twowheeler - PDF 42898fa34f PDFNamasteNo ratings yet
- Tesla Case Study: Submitted byDocument21 pagesTesla Case Study: Submitted byNamasteNo ratings yet
- Chapter-1: Management Accounting - AnDocument20 pagesChapter-1: Management Accounting - AnNamasteNo ratings yet
- Marketing Management-I CP (2019-20)Document7 pagesMarketing Management-I CP (2019-20)NamasteNo ratings yet
- Payslip PDFDocument1 pagePayslip PDFNamasteNo ratings yet
- AD - Portfolio - Equity - and - Debt - Final - 300919Document78 pagesAD - Portfolio - Equity - and - Debt - Final - 300919NamasteNo ratings yet
- APAR User Manual For Ratee Officer PDFDocument25 pagesAPAR User Manual For Ratee Officer PDFNamasteNo ratings yet
- Green Toys Inc - tcm18-229912Document12 pagesGreen Toys Inc - tcm18-229912NamasteNo ratings yet
- Data Driven Decision Making - Course 3 Week 1 Linking Data & Data Modelling Retail WorkbookDocument20 pagesData Driven Decision Making - Course 3 Week 1 Linking Data & Data Modelling Retail WorkbookUdaiveer SinghNo ratings yet
- Collaborating Lawfully To Perform Architectural Consultancy Services in MalaysiaDocument2 pagesCollaborating Lawfully To Perform Architectural Consultancy Services in MalaysiaRidha Razak100% (1)
- Going To University Is More Important Than Ever For Young People - All Must Have DegreesDocument8 pagesGoing To University Is More Important Than Ever For Young People - All Must Have Degreessebastyan_v5466No ratings yet
- Free LancingDocument6 pagesFree LancingArslan HussainNo ratings yet
- Cópia de OECD International Influencer Income and Tax Treaties IBFDDocument18 pagesCópia de OECD International Influencer Income and Tax Treaties IBFDEduarda ManossoNo ratings yet
- Membership: AgreementDocument6 pagesMembership: AgreementMichael KennedyNo ratings yet
- Hull OFOD11 e Solutions CH 30Document6 pagesHull OFOD11 e Solutions CH 30Park GeunhyeNo ratings yet
- Accounting Research PaperDocument8 pagesAccounting Research PaperEsther MpyisiNo ratings yet
- Forensic Audit Report of BKR Foods Pvt. LTDDocument7 pagesForensic Audit Report of BKR Foods Pvt. LTDA Kumar LegacyNo ratings yet
- BrexitDocument8 pagesBrexitKomal RaniNo ratings yet
- India Localization in Enterprise ReleaseDocument11 pagesIndia Localization in Enterprise Releasesandipsen1986No ratings yet
- Chapter 2Document45 pagesChapter 2Dark HunterNo ratings yet
- MAS-03 WorksheetDocument32 pagesMAS-03 WorksheetPaupauNo ratings yet
- 08L0767 Fy18-19 Kyc Aml CFT Fatca CRSDocument13 pages08L0767 Fy18-19 Kyc Aml CFT Fatca CRSabhi646son5124No ratings yet
- BMP6036 - Assigment-2 - Nguyen-Ngoc-Han-2240147 - June-192023-1 2Document21 pagesBMP6036 - Assigment-2 - Nguyen-Ngoc-Han-2240147 - June-192023-1 2HƯƠNG THƠM NguyenNo ratings yet
- Definition and Importance of Lean ManagementDocument2 pagesDefinition and Importance of Lean Managementprakhar guptaNo ratings yet
- R80 Brief For InvestorDocument16 pagesR80 Brief For Investorihsan daniNo ratings yet
- Future of Retail BankingDocument23 pagesFuture of Retail BankingpchresearchNo ratings yet
- Lit Review - Wandana FernandoDocument10 pagesLit Review - Wandana FernandoWandana FernandoNo ratings yet
- Dot 65841 DS1Document234 pagesDot 65841 DS1soghraNo ratings yet
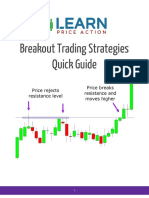
- Breakout Trading Strategies Quick GuideDocument10 pagesBreakout Trading Strategies Quick GuideAdam ChoNo ratings yet
- Why Do They Do ItDocument5 pagesWhy Do They Do Itenzo.rojasaliaga97No ratings yet
- CV Jiaxuan YeDocument2 pagesCV Jiaxuan Yeapi-572237590No ratings yet
- Claims Automation InfographicDocument1 pageClaims Automation InfographicHavoc2003No ratings yet
- SS02 Handouts 2Document2 pagesSS02 Handouts 2RonibeMalinginNo ratings yet
- 05 - Chapter 2Document24 pages05 - Chapter 2annetteNo ratings yet
- Order Book 19.12.2020Document1,065 pagesOrder Book 19.12.2020bikramNo ratings yet
- Why We Study ManagmentDocument6 pagesWhy We Study ManagmentAgumas AlehegnNo ratings yet
































































































Download as pdf or txt
You might also like
- Zitra Personal Account FormDocument2 pagesZitra Personal Account FormUgo BenNo ratings yet
- Exercises/Problems:) R 1 (Ue Termnalval VCF) R 1 (VCF) R 1 (VCF) R 1 (VCF) R 1 (VCFDocument1 pageExercises/Problems:) R 1 (Ue Termnalval VCF) R 1 (VCF) R 1 (VCF) R 1 (VCF) R 1 (VCFIT manNo ratings yet
- Insular Life Insurance FormDocument2 pagesInsular Life Insurance FormEarl Cortez0% (1)
- PNB Customer Information Form IndividualDocument1 pagePNB Customer Information Form IndividualBrittaney BatoNo ratings yet
- Supply Chain ChallengesDocument2 pagesSupply Chain ChallengesAneek RasmomNo ratings yet
- HSP - ClaimForm - New AddressDocument3 pagesHSP - ClaimForm - New AddresssandeepNo ratings yet
- Patient InformationDocument1 pagePatient InformationsmartsportsNo ratings yet
- BM Umbrella Retirement Scheme Member Application Form-EDocument3 pagesBM Umbrella Retirement Scheme Member Application Form-ExeniaNo ratings yet
- Claim FormDocument4 pagesClaim Formsrirama.guttaNo ratings yet
- ALAT Account Customer Update FormDocument1 pageALAT Account Customer Update FormJamiu JabaruNo ratings yet
- Additional Applicant Form: Personal DetailsDocument2 pagesAdditional Applicant Form: Personal DetailsAlhassan EmmanuelNo ratings yet
- RBD - Common Retail Loan Application Form Co - ApplicantDocument2 pagesRBD - Common Retail Loan Application Form Co - Applicantr_awadhiyaNo ratings yet
- Individual Application Form For Registration of Dependants V302 20220302 InteractiveDocument8 pagesIndividual Application Form For Registration of Dependants V302 20220302 InteractiveTsundzuka KhosaNo ratings yet
- Nomination Form: (For Registering A Nominee or Cancelling An Existing Nomination)Document2 pagesNomination Form: (For Registering A Nominee or Cancelling An Existing Nomination)MailNo ratings yet
- Form For Nomination / Appointee Addition: General InformationDocument2 pagesForm For Nomination / Appointee Addition: General InformationSonu SinghNo ratings yet
- Common Retail Loan Application Form For GuarantorDocument2 pagesCommon Retail Loan Application Form For GuarantorNukamreddy Venkateswara ReddyNo ratings yet
- Home Loan Application FormDocument9 pagesHome Loan Application FormSachin KmNo ratings yet
- Revised - AL Form - Document - MITC PDFDocument10 pagesRevised - AL Form - Document - MITC PDFVijayNo ratings yet
- AL Form Document MITCDocument9 pagesAL Form Document MITCRamyaSathyanathanNo ratings yet
- D D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration FormDocument7 pagesD D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration Formdharam singhNo ratings yet
- Application For ServicesDocument4 pagesApplication For ServicesNermeen ElsayedNo ratings yet
- Application Form PDFDocument4 pagesApplication Form PDFTushar RathoreNo ratings yet
- Philhealth - Pag-Ibig MibDocument8 pagesPhilhealth - Pag-Ibig MibChino PaciaNo ratings yet
- Customer Information Update Form: Account DetailsDocument1 pageCustomer Information Update Form: Account DetailsDolapo OlukotunNo ratings yet
- Synchronized Predeployment & Operational Tracker (Spot) : Request For Letter of AuthorizationDocument1 pageSynchronized Predeployment & Operational Tracker (Spot) : Request For Letter of AuthorizationRham OnbenchNo ratings yet
- Individual Personal Accident Insurance Claim FormDocument3 pagesIndividual Personal Accident Insurance Claim FormSatyaNo ratings yet
- FOIA'd Police Report of Tara Durant's 911 CallDocument12 pagesFOIA'd Police Report of Tara Durant's 911 Calljen_benderyNo ratings yet
- Loan Application Form: Applicant Co-ApplicantDocument4 pagesLoan Application Form: Applicant Co-ApplicantStatus SambavanghalNo ratings yet
- Emp Bus SPC AirportsDocument1 pageEmp Bus SPC AirportsShami MudunkotuwaNo ratings yet
- Sbi Home Loans Application FormDocument5 pagesSbi Home Loans Application FormHimanshu AshwiniNo ratings yet
- IPA Claim FormDocument5 pagesIPA Claim FormVivek ChopraNo ratings yet
- Information Form: Maldives Islamic BankDocument5 pagesInformation Form: Maldives Islamic BankyrafeeuNo ratings yet
- MSME Loan Application Form - Partnership - 1 PagerDocument2 pagesMSME Loan Application Form - Partnership - 1 Pagernambi2rajanNo ratings yet
- Group Personal Accident-Claim FormDocument4 pagesGroup Personal Accident-Claim FormVipul SharmaNo ratings yet
- Adr 2Document2 pagesAdr 2ok2bwellNo ratings yet
- New Format Application Form CLRDocument8 pagesNew Format Application Form CLRtheonelNo ratings yet
- Tax Client QuestionaireDocument3 pagesTax Client QuestionaireCory100% (1)
- Position Applied For: Other Position(s) of Interest: Salary Expected: (Net/ Gross) Date Available To StartDocument4 pagesPosition Applied For: Other Position(s) of Interest: Salary Expected: (Net/ Gross) Date Available To StartalfathNo ratings yet
- Patient Demographics FormDocument1 pagePatient Demographics FormChynta Adilla AdillaNo ratings yet
- Congi Application FormDocument6 pagesCongi Application Formsharathkumarreddy2021No ratings yet
- Pis SignDocument1 pagePis SignJoshua RuizNo ratings yet
- (Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanDocument2 pages(Please Send This Back To Corporate Accounts Division) : Application For Group Insurance PlanKristian Romeo NapiñasNo ratings yet
- Update Info FormDocument1 pageUpdate Info FormEsan BiolaNo ratings yet
- Personal Information (Amended)Document3 pagesPersonal Information (Amended)TANU SINGHNo ratings yet
- Agency/Person Information: OSS Amage EportDocument1 pageAgency/Person Information: OSS Amage EportClarenceJoy Ferrer Dela CruzNo ratings yet
- JMT HR - Form 003 v1 - New Employee Information FormDocument1 pageJMT HR - Form 003 v1 - New Employee Information FormMaral Inocencio AltarNo ratings yet
- FIR Form PunjabDocument1 pageFIR Form PunjabSanjiv KumarNo ratings yet
- PMRF RevisedDocument2 pagesPMRF RevisedDBVS GRAY MORTERANo ratings yet
- Public Liability Claim Form EngDocument1 pagePublic Liability Claim Form EngVeron AcNo ratings yet
- 18 Account Opening FormDocument11 pages18 Account Opening Formhl2225742No ratings yet
- Steps Forward Patient DemographicsDocument3 pagesSteps Forward Patient DemographicsdawnNo ratings yet
- Page Loan FormDocument2 pagesPage Loan FormChukwuemeka Great NwankwoNo ratings yet
- Home Loans Application: First National Bank Ghana Limited, A Subsidiary of Firstrand Group, South AfricaDocument12 pagesHome Loans Application: First National Bank Ghana Limited, A Subsidiary of Firstrand Group, South Africazirri23No ratings yet
- Nomination Form PLIDocument2 pagesNomination Form PLIGeethanjali RajanalaNo ratings yet
- TERC HR - Form 003 v1 - New Employee Information FormDocument1 pageTERC HR - Form 003 v1 - New Employee Information FormMaral Inocencio AltarNo ratings yet
- Employee Information Form 06Document3 pagesEmployee Information Form 06Dave PagaraNo ratings yet
- Children Policy ProposalDocument4 pagesChildren Policy ProposalNitin KumarNo ratings yet
- ERISA/Non-ERISA - Change of Beneficiary/ Spousal Consent: SECTION 1: Participant InformationDocument5 pagesERISA/Non-ERISA - Change of Beneficiary/ Spousal Consent: SECTION 1: Participant InformationandryNo ratings yet
- Prepaid Card Application Form: 1. Personal InformationDocument9 pagesPrepaid Card Application Form: 1. Personal InformationcharmainejalaNo ratings yet
- Patient Intatke FormsDocument3 pagesPatient Intatke FormsBryan KiddNo ratings yet
- Please Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeDocument2 pagesPlease Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeMosses BryanNo ratings yet
- CamScanner 10-17-2020 16.26.25 PDFDocument9 pagesCamScanner 10-17-2020 16.26.25 PDFNamasteNo ratings yet
- Claims Forms Auto Secure Private Car Twowheeler - PDF 42898fa34f PDFDocument2 pagesClaims Forms Auto Secure Private Car Twowheeler - PDF 42898fa34f PDFNamasteNo ratings yet
- Tesla Case Study: Submitted byDocument21 pagesTesla Case Study: Submitted byNamasteNo ratings yet
- Chapter-1: Management Accounting - AnDocument20 pagesChapter-1: Management Accounting - AnNamasteNo ratings yet
- Marketing Management-I CP (2019-20)Document7 pagesMarketing Management-I CP (2019-20)NamasteNo ratings yet
- Payslip PDFDocument1 pagePayslip PDFNamasteNo ratings yet
- AD - Portfolio - Equity - and - Debt - Final - 300919Document78 pagesAD - Portfolio - Equity - and - Debt - Final - 300919NamasteNo ratings yet
- APAR User Manual For Ratee Officer PDFDocument25 pagesAPAR User Manual For Ratee Officer PDFNamasteNo ratings yet
- Green Toys Inc - tcm18-229912Document12 pagesGreen Toys Inc - tcm18-229912NamasteNo ratings yet
- Data Driven Decision Making - Course 3 Week 1 Linking Data & Data Modelling Retail WorkbookDocument20 pagesData Driven Decision Making - Course 3 Week 1 Linking Data & Data Modelling Retail WorkbookUdaiveer SinghNo ratings yet
- Collaborating Lawfully To Perform Architectural Consultancy Services in MalaysiaDocument2 pagesCollaborating Lawfully To Perform Architectural Consultancy Services in MalaysiaRidha Razak100% (1)
- Going To University Is More Important Than Ever For Young People - All Must Have DegreesDocument8 pagesGoing To University Is More Important Than Ever For Young People - All Must Have Degreessebastyan_v5466No ratings yet
- Free LancingDocument6 pagesFree LancingArslan HussainNo ratings yet
- Cópia de OECD International Influencer Income and Tax Treaties IBFDDocument18 pagesCópia de OECD International Influencer Income and Tax Treaties IBFDEduarda ManossoNo ratings yet
- Membership: AgreementDocument6 pagesMembership: AgreementMichael KennedyNo ratings yet
- Hull OFOD11 e Solutions CH 30Document6 pagesHull OFOD11 e Solutions CH 30Park GeunhyeNo ratings yet
- Accounting Research PaperDocument8 pagesAccounting Research PaperEsther MpyisiNo ratings yet
- Forensic Audit Report of BKR Foods Pvt. LTDDocument7 pagesForensic Audit Report of BKR Foods Pvt. LTDA Kumar LegacyNo ratings yet
- BrexitDocument8 pagesBrexitKomal RaniNo ratings yet
- India Localization in Enterprise ReleaseDocument11 pagesIndia Localization in Enterprise Releasesandipsen1986No ratings yet
- Chapter 2Document45 pagesChapter 2Dark HunterNo ratings yet
- MAS-03 WorksheetDocument32 pagesMAS-03 WorksheetPaupauNo ratings yet
- 08L0767 Fy18-19 Kyc Aml CFT Fatca CRSDocument13 pages08L0767 Fy18-19 Kyc Aml CFT Fatca CRSabhi646son5124No ratings yet
- BMP6036 - Assigment-2 - Nguyen-Ngoc-Han-2240147 - June-192023-1 2Document21 pagesBMP6036 - Assigment-2 - Nguyen-Ngoc-Han-2240147 - June-192023-1 2HƯƠNG THƠM NguyenNo ratings yet
- Definition and Importance of Lean ManagementDocument2 pagesDefinition and Importance of Lean Managementprakhar guptaNo ratings yet
- R80 Brief For InvestorDocument16 pagesR80 Brief For Investorihsan daniNo ratings yet
- Future of Retail BankingDocument23 pagesFuture of Retail BankingpchresearchNo ratings yet
- Lit Review - Wandana FernandoDocument10 pagesLit Review - Wandana FernandoWandana FernandoNo ratings yet
- Dot 65841 DS1Document234 pagesDot 65841 DS1soghraNo ratings yet
- Breakout Trading Strategies Quick GuideDocument10 pagesBreakout Trading Strategies Quick GuideAdam ChoNo ratings yet
- Why Do They Do ItDocument5 pagesWhy Do They Do Itenzo.rojasaliaga97No ratings yet
- CV Jiaxuan YeDocument2 pagesCV Jiaxuan Yeapi-572237590No ratings yet
- Claims Automation InfographicDocument1 pageClaims Automation InfographicHavoc2003No ratings yet
- SS02 Handouts 2Document2 pagesSS02 Handouts 2RonibeMalinginNo ratings yet
- 05 - Chapter 2Document24 pages05 - Chapter 2annetteNo ratings yet
- Order Book 19.12.2020Document1,065 pagesOrder Book 19.12.2020bikramNo ratings yet
- Why We Study ManagmentDocument6 pagesWhy We Study ManagmentAgumas AlehegnNo ratings yet