Download as pdf or txt
You might also like
- Etomidate As An Induction Agent For Endotracheal Intubation in CriticallyDocument6 pagesEtomidate As An Induction Agent For Endotracheal Intubation in CriticallyJose Eduardo Valle LomeliNo ratings yet
- Ctev Short CaseDocument3 pagesCtev Short CaseEmmanuel DanielsNo ratings yet
- Griese2017 PDFDocument10 pagesGriese2017 PDFgustavo adolfo rodriguez alzateNo ratings yet
- Aagl Practice Guidelines For The Diagnosis and Management of Endometrial Polyps PDFDocument8 pagesAagl Practice Guidelines For The Diagnosis and Management of Endometrial Polyps PDFhusain abdul halimNo ratings yet
- Research Article: Machine Learning-Based Model To Predict The Disease Severity and Outcome in COVID-19 PatientsDocument10 pagesResearch Article: Machine Learning-Based Model To Predict The Disease Severity and Outcome in COVID-19 Patientsamin mohNo ratings yet
- What To Know About The Cost-Effectiveness of Seasonal Malaria Chemoprevention in Endemic Countries: A Systematic ReviewDocument8 pagesWhat To Know About The Cost-Effectiveness of Seasonal Malaria Chemoprevention in Endemic Countries: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Acute Kidney Injury Following Multisystem Infammatory Syndrome Associated With SARS CoV 2 Infection in ChildrenDocument14 pagesAcute Kidney Injury Following Multisystem Infammatory Syndrome Associated With SARS CoV 2 Infection in ChildrenBlack ManNo ratings yet
- Vaccine Cold ChainDocument6 pagesVaccine Cold ChainDianne LimosNo ratings yet
- 10.1007@s00383 020 04696 yDocument11 pages10.1007@s00383 020 04696 yMeta ParamitaNo ratings yet
- Adverse Drug Reactions of Spontaneous Reports in Shanghai Pediatric PopulationDocument6 pagesAdverse Drug Reactions of Spontaneous Reports in Shanghai Pediatric PopulationLika MaharNo ratings yet
- Work ExposureDocument5 pagesWork ExposureJaved IqbalNo ratings yet
- Cutaneous Candidiasis - An Evidence-Based Review of Topical and Systemic Treatments To Inform Clinical PracticeDocument11 pagesCutaneous Candidiasis - An Evidence-Based Review of Topical and Systemic Treatments To Inform Clinical PracticeRose ParkNo ratings yet
- TocilizumabDocument14 pagesTocilizumabTri CahyaniNo ratings yet
- The Influence of Comorbidity On The Severity of CODocument13 pagesThe Influence of Comorbidity On The Severity of COBurhan AquariusNo ratings yet
- 32 01 09 GrazinaDocument16 pages32 01 09 GrazinaDisty ANo ratings yet
- Do Spermicides Containing Nonoxynol-9 Prevent Sexually Transmitted Infections: A Meta-AnalysisDocument4 pagesDo Spermicides Containing Nonoxynol-9 Prevent Sexually Transmitted Infections: A Meta-Analysisindah febrianiNo ratings yet
- International Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsDocument9 pagesInternational Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsPujiNo ratings yet
- Journal 6Document4 pagesJournal 6margareth silaenNo ratings yet
- 10.1007@s00404 019 05301 XDocument11 pages10.1007@s00404 019 05301 XAbdElilah KoNo ratings yet
- Corticosteroids As Adjunctive Therapy in Bacterial Meningitis: A Systematic Review of Clinical TrialsDocument11 pagesCorticosteroids As Adjunctive Therapy in Bacterial Meningitis: A Systematic Review of Clinical TrialsDexter IanNo ratings yet
- Risk Factors of Colorectal Carcinoma Incidence in Young Adults: A Meta-AnalysisDocument6 pagesRisk Factors of Colorectal Carcinoma Incidence in Young Adults: A Meta-AnalysisNoviTrianaNo ratings yet
- Journal ReadingDocument14 pagesJournal ReadingelvanNo ratings yet
- Hahn El 2016Document9 pagesHahn El 2016ka waiiNo ratings yet
- Wagner2022 Article EfficacyAndSafetyOfIntravenousDocument13 pagesWagner2022 Article EfficacyAndSafetyOfIntravenoustito reddyNo ratings yet
- Snow2021 Article TocilizumabInCOVID-19AMeta-anaDocument12 pagesSnow2021 Article TocilizumabInCOVID-19AMeta-anaYajaira UgenioNo ratings yet
- Contact Lens and Anterior Eye: Dayron F. Martínez-Pulgarín, Marcel Y. Avila, Alfonso J. Rodríguez-MoralesDocument8 pagesContact Lens and Anterior Eye: Dayron F. Martínez-Pulgarín, Marcel Y. Avila, Alfonso J. Rodríguez-MoralesAndi SilpiaNo ratings yet
- Jurnal 3 KA inggDocument7 pagesJurnal 3 KA inggMardika Wulandari 20 XII IPS3No ratings yet
- 2018 Article 276Document8 pages2018 Article 276Lulu NurainiNo ratings yet
- P0581 548 Risk Factors of Severity of Dengue.639Document1 pageP0581 548 Risk Factors of Severity of Dengue.639Hendri HariyantoNo ratings yet
- Investigation of Intertriginous Mycotic and Pseudomycotic (Erythrasma) Infections and Their Causative Agents With Emphasize On Clinical PresentationsDocument7 pagesInvestigation of Intertriginous Mycotic and Pseudomycotic (Erythrasma) Infections and Their Causative Agents With Emphasize On Clinical PresentationsKiki FatmawatyNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument7 pagesInternational Journal of Pediatric OtorhinolaryngologyAndi SuhriyanaNo ratings yet
- 1 s2.0 S0933365721001500 MainDocument16 pages1 s2.0 S0933365721001500 MainmsworkbbhNo ratings yet
- Fan Bai, Gang Gang Li, Qingmin Liu, Xinwu Niu, Ruilian Li, and Huiqun MaDocument26 pagesFan Bai, Gang Gang Li, Qingmin Liu, Xinwu Niu, Ruilian Li, and Huiqun Maluthfianisa azhariNo ratings yet
- The Prevalence and Outcomes of Frail Older Adults in Clinical Trials in Multiple Myeloma: A Systematic ReviewDocument13 pagesThe Prevalence and Outcomes of Frail Older Adults in Clinical Trials in Multiple Myeloma: A Systematic Reviewfga.crislainebernardino01No ratings yet
- JMM D 21 00263Document23 pagesJMM D 21 00263Jonathas TrindadeNo ratings yet
- Risk Factors For Ectopic Pregnancy: A Comprehensive Analysis Based On A Large Case-Control, Population-Based Study in FranceDocument10 pagesRisk Factors For Ectopic Pregnancy: A Comprehensive Analysis Based On A Large Case-Control, Population-Based Study in FranceAreef EymanNo ratings yet
- 15 - 93-98 Ujmr 034Document6 pages15 - 93-98 Ujmr 034KHADIJA TELANo ratings yet
- Oxidative Stress in Acne Vulgaris: Jisha R., Saboora Beegum M., Yogapriya VDocument4 pagesOxidative Stress in Acne Vulgaris: Jisha R., Saboora Beegum M., Yogapriya VvinayNo ratings yet
- Articulo 8Document7 pagesArticulo 8Marcela RodriguezNo ratings yet
- 1909 Recent Advances in Pharmacological Treatments of Adult DermatomyositisDocument10 pages1909 Recent Advances in Pharmacological Treatments of Adult DermatomyositisFlorian LamblinNo ratings yet
- Ljad 308Document11 pagesLjad 308laurenNo ratings yet
- JMV 26509Document12 pagesJMV 26509a27091No ratings yet
- A Study of Effectiveness and Safety of Topical ComDocument7 pagesA Study of Effectiveness and Safety of Topical ComFalaq AgastyaNo ratings yet
- Predicciom-Meningitis NiñosDocument12 pagesPredicciom-Meningitis NiñosJulioRoblesZanelliNo ratings yet
- Tight Glycemic Control in Critically Ill PediatricDocument11 pagesTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaNo ratings yet
- Review ArticleDocument8 pagesReview ArticleIdmNo ratings yet
- The Histopathological Spectrum of Human MeningiomaDocument13 pagesThe Histopathological Spectrum of Human MeningiomaHastrina MailaniNo ratings yet
- Allergy - 2022 - Farraia - Allergen Immunotherapy For Asthma Prevention A Systematic Review and Meta Analysis ofDocument17 pagesAllergy - 2022 - Farraia - Allergen Immunotherapy For Asthma Prevention A Systematic Review and Meta Analysis ofpedrotiagosilvaNo ratings yet
- Kelaidi-2010Document8 pagesKelaidi-2010María Alejandra Lopez SalasNo ratings yet
- A Systematic Review of Individual Patient Data Meta-Analyses On Surgical InterventionsDocument12 pagesA Systematic Review of Individual Patient Data Meta-Analyses On Surgical InterventionsNitya KrishnaNo ratings yet
- PediatriaDocument11 pagesPediatrianuelitopNo ratings yet
- Respiratory Distress in PediatricsDocument6 pagesRespiratory Distress in Pediatricsthirunagari praveenNo ratings yet
- Immunodeficiencies Based On Clinical, Systematic Classification of PrimaryDocument8 pagesImmunodeficiencies Based On Clinical, Systematic Classification of PrimaryJimmyNo ratings yet
- Karumbi Et Al 2013Document6 pagesKarumbi Et Al 2013sundaimeNo ratings yet
- Microbiology of Chronic Suppurative Otitis Media in A Tertiary Care Setup of Uttarakhand State, IndiaDocument10 pagesMicrobiology of Chronic Suppurative Otitis Media in A Tertiary Care Setup of Uttarakhand State, IndiaMas YettyNo ratings yet
- Treatment of Enterocutaneous Fistula A Systematic Review and MetaanalysisDocument12 pagesTreatment of Enterocutaneous Fistula A Systematic Review and MetaanalysisMarcus CezilloNo ratings yet
- Muzii Et Al., 2020Document9 pagesMuzii Et Al., 2020Jonathan LucisNo ratings yet
- AppendicitisDocument13 pagesAppendicitisASdaNo ratings yet
- Insulin LikeDocument8 pagesInsulin LikecarolineNo ratings yet
- WWW - Kup.at/ Journals/eano/index - HTML: Systemic Treatment of Recurrent MeningiomaDocument8 pagesWWW - Kup.at/ Journals/eano/index - HTML: Systemic Treatment of Recurrent MeningiomaAnonymous KKqrboTNo ratings yet
- Propranolol-Resistant Infantile Hemangioma Successfully Treated With SirolimusDocument3 pagesPropranolol-Resistant Infantile Hemangioma Successfully Treated With SirolimusindriNo ratings yet
- Treatment of Alarming Head and Neck Infantile HemaDocument5 pagesTreatment of Alarming Head and Neck Infantile HemaindriNo ratings yet
- Pulsed Dye Laser Therapy For Infantile Hemangiomas: A Systemic Review and Meta-AnalysisDocument8 pagesPulsed Dye Laser Therapy For Infantile Hemangiomas: A Systemic Review and Meta-AnalysisindriNo ratings yet
- NSC Update in Dermatology and Venereology 2018 (26 - 28 October 2018)Document2 pagesNSC Update in Dermatology and Venereology 2018 (26 - 28 October 2018)indriNo ratings yet
- Resection of Localized Cheek Infantile HemangiomaDocument4 pagesResection of Localized Cheek Infantile HemangiomaindriNo ratings yet
- Annals of Plastic and Reconstructive SurgeryDocument3 pagesAnnals of Plastic and Reconstructive SurgeryindriNo ratings yet
- Microbiology Laboratoric TestDocument17 pagesMicrobiology Laboratoric TestindriNo ratings yet
- Epidermolysis Bullosa Acquisita The 2019 Update PDFDocument28 pagesEpidermolysis Bullosa Acquisita The 2019 Update PDFindriNo ratings yet
- 008Document3 pages008indriNo ratings yet
- Sun Pharmaceutical Industries LTD Vs DWD PharmaceuticalsDocument13 pagesSun Pharmaceutical Industries LTD Vs DWD PharmaceuticalsDeon FernandesNo ratings yet
- Reflection (Setting Application 3)Document2 pagesReflection (Setting Application 3)DavidNo ratings yet
- Social Anxiety (CASE STUDY)Document7 pagesSocial Anxiety (CASE STUDY)Angel DIMACULANGANNo ratings yet
- BSA Application FormDocument8 pagesBSA Application Formnekimo155No ratings yet
- Tugas Bahasa Inggris HERMAWANDocument2 pagesTugas Bahasa Inggris HERMAWANherawan761No ratings yet
- A Brief Note On Orthopedic PhysiotherapyDocument2 pagesA Brief Note On Orthopedic Physiotherapyasfand khanNo ratings yet
- Dissertation Mzizi JNDocument118 pagesDissertation Mzizi JNpamelaNo ratings yet
- Do You Believe That Every Filipino Should Own A House or Is It Enough For Us To Have A Roof Above Our Head?Document2 pagesDo You Believe That Every Filipino Should Own A House or Is It Enough For Us To Have A Roof Above Our Head?Krista Jane AvilaNo ratings yet
- Pile Foundation: Method StatmentDocument12 pagesPile Foundation: Method StatmentDeepak PatilNo ratings yet
- Embryology and PsychologyDocument3 pagesEmbryology and PsychologyReshma UbeyratnaNo ratings yet
- Sdo Bulacan Cse Action Plan 2023 2024Document4 pagesSdo Bulacan Cse Action Plan 2023 2024heraldantoni.resurreccion100% (2)
- Effect of Hyaluronic Acid On The Osseointegration of Dental ImplantsDocument5 pagesEffect of Hyaluronic Acid On The Osseointegration of Dental Implantsjaviers45No ratings yet
- Intravaginal Progesterone Device (1.9g) and Estradiol Benzoate For Follicular Control in The Mare During Spring and SummerDocument10 pagesIntravaginal Progesterone Device (1.9g) and Estradiol Benzoate For Follicular Control in The Mare During Spring and SummerCaio DonizettiNo ratings yet
- Research Methods Concepts and Connections 2nd Edition Passer Test BankDocument33 pagesResearch Methods Concepts and Connections 2nd Edition Passer Test Bankmilterjubilatepo8y1b100% (29)
- Week Physical Activity Log TemplateDocument3 pagesWeek Physical Activity Log TemplateDanessa BaybayanNo ratings yet
- Life Is A Stage - Autistic Perspectives On NeurotypicalityDocument10 pagesLife Is A Stage - Autistic Perspectives On NeurotypicalityvictorNo ratings yet
- Pandemic 19 BontsgfdDocument2 pagesPandemic 19 BontsgfdRhendelle Jun BacongNo ratings yet
- Service Management Operations Strategy Information Technology 10Th Edition Sanjeev K Bordoloi Full Download ChapterDocument51 pagesService Management Operations Strategy Information Technology 10Th Edition Sanjeev K Bordoloi Full Download Chapteramanda.mejia743100% (10)
- Laboratory Activity No 2 - GLOVA-NDDocument4 pagesLaboratory Activity No 2 - GLOVA-NDandreyou99No ratings yet
- Puerto Rico NPI Data EdirectoryDocument62 pagesPuerto Rico NPI Data EdirectoryNPI Data ServicesNo ratings yet
- Aspects of The Topic ReadingsDocument4 pagesAspects of The Topic ReadingsBettNo ratings yet
- Soal BHS ING SAS SM 2 2023 2024Document3 pagesSoal BHS ING SAS SM 2 2023 2024Hari EngkufNo ratings yet
- Buasao Heading New Feeding Narrative ReportDocument5 pagesBuasao Heading New Feeding Narrative ReportDaisy Ann AlferezNo ratings yet
- DIAGNOSTIC TEST Tonometry Corneal StainingDocument29 pagesDIAGNOSTIC TEST Tonometry Corneal StainingJhonelle ProdigalidadNo ratings yet
- Slickline FATALITY - Lesson LearnedDocument5 pagesSlickline FATALITY - Lesson LearnedHossam Hussain HamoudaNo ratings yet
- Mental Healt Assessment Website SynopsisDocument20 pagesMental Healt Assessment Website Synopsisshishir6418No ratings yet
- Brochure - Teleradiology Market - Forecast To 2025Document32 pagesBrochure - Teleradiology Market - Forecast To 2025Purav PillaiNo ratings yet
- 1.b. Bronchiolitis Clinical Presentation - History, Physical Examination, ComplicationsDocument3 pages1.b. Bronchiolitis Clinical Presentation - History, Physical Examination, ComplicationsDavid CraigNo ratings yet
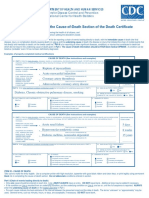
- Instructions For Completing The Cause of Death Section On Death Certificate PDFDocument2 pagesInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoNo ratings yet