Download as pdf or txt
You might also like
- B2 Listening FCE For Schools 1 Test 4 QuestionsDocument4 pagesB2 Listening FCE For Schools 1 Test 4 QuestionsÁlvaro Izquierdo Díaz25% (12)
- 27 Flights Controls PDFDocument186 pages27 Flights Controls PDFAaron Harvey100% (3)
- Fuchs - in Defense of The Human Being (2021)Document273 pagesFuchs - in Defense of The Human Being (2021)BododNo ratings yet
- Abraham-Hicks 2001-2009 Collection 56CDsDocument2 pagesAbraham-Hicks 2001-2009 Collection 56CDsSahl H JamsheerNo ratings yet
- In Vitro Generation Of: Immortalized CD34+Document3 pagesIn Vitro Generation Of: Immortalized CD34+Mind NiramindNo ratings yet
- Transmit: For ofDocument32 pagesTransmit: For ofARACRAFTNo ratings yet
- Pluripotent Stem Cell GuidebookDocument52 pagesPluripotent Stem Cell GuidebookJonathan Torralba TorrónNo ratings yet
- Final Capstone Poster-Mann PDFDocument1 pageFinal Capstone Poster-Mann PDFAmy Nottingham-MartinNo ratings yet
- Genetic DisordersDocument3 pagesGenetic Disordersdia akuNo ratings yet
- Ingeniería Genética I: Transferencia HorizontalDocument12 pagesIngeniería Genética I: Transferencia HorizontalHandball AmeliaNo ratings yet
- Gene Structure 1+2 - محمود منصورDocument3 pagesGene Structure 1+2 - محمود منصورانس ابوهيبةNo ratings yet
- Authors: Ibel Carri, María Marcela Barrio, Morten Nielsen: BackgroundDocument1 pageAuthors: Ibel Carri, María Marcela Barrio, Morten Nielsen: BackgroundrexNo ratings yet
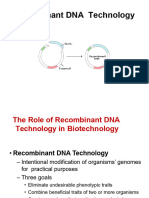
- Recombinant DNA Technology 2023Document29 pagesRecombinant DNA Technology 2023Ana Laura Mendoza AriasNo ratings yet
- 18 - 유전자의 발현 조절Document30 pages18 - 유전자의 발현 조절김도윤No ratings yet
- From Gene To Protein: How Genes WorkDocument58 pagesFrom Gene To Protein: How Genes WorkGabe GallagherNo ratings yet
- DNA TechnologyDocument28 pagesDNA TechnologyJohn NinoNo ratings yet
- Genes and The Genetic Code: An Introduction To Gene Expression With Georgina CornwallDocument24 pagesGenes and The Genetic Code: An Introduction To Gene Expression With Georgina CornwallJeanne Waldo ReminajesNo ratings yet
- 1 Embryo Development Plastids LTDocument83 pages1 Embryo Development Plastids LTrodrigoNo ratings yet
- MIC 210 Basic Molecular Biology: DNA CloningDocument54 pagesMIC 210 Basic Molecular Biology: DNA CloningDrAhmedSalimNo ratings yet
- Matrix Functional Studies - 2024Document1 pageMatrix Functional Studies - 2024arnehoushmand9No ratings yet
- Step 1 Notes DrawingsDocument7 pagesStep 1 Notes DrawingsDeborah PetersNo ratings yet
- Note 22 Nov 2022Document2 pagesNote 22 Nov 2022sjames20032312No ratings yet
- Best HandMade Notes of INHERITANCE ChapterDocument12 pagesBest HandMade Notes of INHERITANCE Chapterhbadhani11No ratings yet
- Strategi KloningDocument13 pagesStrategi Kloningfadil pohanNo ratings yet
- Genetics2 ROAMSDocument11 pagesGenetics2 ROAMSvkNo ratings yet
- Character Sheet Page 1Document2 pagesCharacter Sheet Page 1CanageekNo ratings yet
- Lec 8Document3 pagesLec 8lilliaNo ratings yet
- Transcription FactorsDocument13 pagesTranscription Factorsfazila zahoorNo ratings yet
- Immunopeptidomics PDFDocument14 pagesImmunopeptidomics PDFYanbo PanNo ratings yet
- Csir Net Unit 13 Min Maps BiotecnikDocument12 pagesCsir Net Unit 13 Min Maps BiotecniksantsarnsinghNo ratings yet
- Termofisher Guide Stem CellDocument60 pagesTermofisher Guide Stem Cellnadhifa akNo ratings yet
- III. Gen Perk S2 - DIR 2021 - Pengontrolan Ekspresi GenDocument17 pagesIII. Gen Perk S2 - DIR 2021 - Pengontrolan Ekspresi GenSisy YuliantyNo ratings yet
- BIO353 Lecture9 (Transcription SHF 2021 LongDocument115 pagesBIO353 Lecture9 (Transcription SHF 2021 LongMina KoçNo ratings yet
- 12 Zoology PraticalDocument9 pages12 Zoology PraticalAl RaashidNo ratings yet
- Protein Synthesis LegendDocument1 pageProtein Synthesis Legendkirby kirNo ratings yet
- Chapter 13 - Genetic EngineeringDocument23 pagesChapter 13 - Genetic EngineeringDanielle TurnerNo ratings yet
- EUKARYOTIC DNA VIRUSES - Temporal Control: 1. Simian Virus 40Document2 pagesEUKARYOTIC DNA VIRUSES - Temporal Control: 1. Simian Virus 40Maria August P. PrudencioNo ratings yet
- Biology CellDocument7 pagesBiology CellAida AzharNo ratings yet
- Gene Regulation: What It Is, and How To Detect It: by Jordan, Jennifer, and BrianDocument12 pagesGene Regulation: What It Is, and How To Detect It: by Jordan, Jennifer, and BriansujathaNo ratings yet
- Graduate Course For Year October - 13 - 2005Document97 pagesGraduate Course For Year October - 13 - 2005api-3701422No ratings yet
- Lodish CloningDocument38 pagesLodish CloninggustavoNo ratings yet
- UNIT 9 BIOTECH #ProjectClimaxDocument1 pageUNIT 9 BIOTECH #ProjectClimaxfdghdchNo ratings yet
- Lecture 30 Notes - DhruvDocument68 pagesLecture 30 Notes - Dhruvhyy370815No ratings yet
- CanalsDocument25 pagesCanalsJurgen suarez moncaleanoNo ratings yet
- Cell CycleDocument1 pageCell CycleAvinashNo ratings yet
- Gene Regulation, Transposon N Genetic VariationDocument27 pagesGene Regulation, Transposon N Genetic Variationbishalstha079No ratings yet
- Mbt1 B Cloning Expression 14 15Document91 pagesMbt1 B Cloning Expression 14 15Abhishek SinghNo ratings yet
- Lecture 3 Early Embryonic DevelopmentDocument40 pagesLecture 3 Early Embryonic DevelopmentZari Sofia LevisteNo ratings yet
- Biology Data: D N A V T N B, BDocument3 pagesBiology Data: D N A V T N B, Bapara_jitNo ratings yet
- Folwchart NGSDocument3 pagesFolwchart NGSกรวรินทร์ ชำนาญกุลNo ratings yet
- Central DogmaDocument48 pagesCentral Dogmajhem.me28No ratings yet
- Biol 23Document820 pagesBiol 23defnedemircayNo ratings yet
- Bacterial MorphologyDocument2 pagesBacterial MorphologyJulia IshakNo ratings yet
- Gene Function: Group 1 Animal Breeding 2018Document10 pagesGene Function: Group 1 Animal Breeding 2018Alif Utama PNo ratings yet
- Lva1 App6891 PDFDocument33 pagesLva1 App6891 PDFabhishekNo ratings yet
- Stem CellDocument1 pageStem CellSNo ratings yet
- PubMed Central, Table 1 - BMC Biol. 2017 15 - 53. Published Online 2017 Jun 29. Doi - 10.1186 - s12915-017-0392-4Document1 pagePubMed Central, Table 1 - BMC Biol. 2017 15 - 53. Published Online 2017 Jun 29. Doi - 10.1186 - s12915-017-0392-4KarenNo ratings yet
- Lecture 3Document34 pagesLecture 3silaazak3No ratings yet
- Powerpoint Protein LocalizationDocument54 pagesPowerpoint Protein LocalizationJoseph BenaiahNo ratings yet
- Genetics: From Genes To GenomesDocument58 pagesGenetics: From Genes To GenomesAshleyNo ratings yet
- Bio Compare and ContrastDocument2 pagesBio Compare and ContrastRhea SivakumarNo ratings yet
- A175547 PCR ApplicationDocument1 pageA175547 PCR ApplicationMohammad Danial SakariaNo ratings yet
- KT152 GeNeiPure Plasmid ExtractionDocument11 pagesKT152 GeNeiPure Plasmid ExtractionHemant KawalkarNo ratings yet
- SDJ 2018-05 ResearchDocument11 pagesSDJ 2018-05 ResearchSaifuddin HaswareNo ratings yet
- Chapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartDocument53 pagesChapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartSaifuddin HaswareNo ratings yet
- Crisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Document12 pagesCrisp1 and Alopecia Areata in C3H/Hej Mice: Crisp1/Crisp1, Cysteine-Rich Secretory Protein 1, Gene/Protein Crisp1Saifuddin HaswareNo ratings yet
- Oral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot StudyDocument7 pagesOral Squamous Cell Carcinoma of Tongue: Histological Risk Assessment. A Pilot StudySaifuddin HaswareNo ratings yet
- JCDP 20 444Document5 pagesJCDP 20 444Saifuddin HaswareNo ratings yet
- Mono99 17Document160 pagesMono99 17Saifuddin HaswareNo ratings yet
- Capture of Hair Geometry From Multiple ImagesDocument8 pagesCapture of Hair Geometry From Multiple ImagesSaifuddin HaswareNo ratings yet
- Cheng JARODocument15 pagesCheng JAROSaifuddin HaswareNo ratings yet
- Adenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceDocument7 pagesAdenovirus-Mediated Wnt5a Expression Inhibits The Telogen-To-Anagen Transition of Hair Follicles in MiceSaifuddin HaswareNo ratings yet
- Variations of Hair Follicle Size and Distribution in Different Body SitesDocument6 pagesVariations of Hair Follicle Size and Distribution in Different Body SitesSaifuddin HaswareNo ratings yet
- Splenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapyDocument9 pagesSplenic Melanosis During Normal Murine C57BL/6 Hair Cycle and After ChemotherapySaifuddin HaswareNo ratings yet
- Inexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishDocument7 pagesInexhaustible Hair-Cell Regeneration in Young and Aged ZebrafishSaifuddin HaswareNo ratings yet
- 286 FullDocument8 pages286 FullSaifuddin HaswareNo ratings yet
- Noise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKDocument14 pagesNoise Induced Loss of Hair Cells and Cochlear Synaptopathy Are Mediated by The Activation of AMPKSaifuddin HaswareNo ratings yet
- Hair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsDocument15 pagesHair Cortisol Analyses in Different Mammal Species: Choosing The Wrong Assay May Lead To Erroneous ResultsSaifuddin HaswareNo ratings yet
- Thymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationDocument9 pagesThymosin Beta 4 Induces Hair Growth Via Stem Cell Migration and DifferentiationSaifuddin HaswareNo ratings yet
- September 2013 BourlandDocument38 pagesSeptember 2013 BourlandSaifuddin HaswareNo ratings yet
- Uncombable Hair SyndromeDocument3 pagesUncombable Hair SyndromeSaifuddin HaswareNo ratings yet
- Marketing ManagementDocument9 pagesMarketing ManagementShashi mehtaNo ratings yet
- Geronimo StiltonDocument2 pagesGeronimo StiltonRajeshNo ratings yet
- ENGLISH PLUS-Syllabus by MercadoDocument8 pagesENGLISH PLUS-Syllabus by MercadoJean GuntanNo ratings yet
- Data Warehousing Quick GuideDocument66 pagesData Warehousing Quick Guidejacktheking2010No ratings yet
- Multi-Disease Prediction With Machine LearningDocument7 pagesMulti-Disease Prediction With Machine LearningUmar KhanNo ratings yet
- Bidding Docs For DBWD Nlif May Final 2013projectDocument158 pagesBidding Docs For DBWD Nlif May Final 2013projectrain06021992No ratings yet
- Bandarban at A GlanceDocument29 pagesBandarban at A GlanceShahriazAlamNo ratings yet
- Day 1 NotesDocument4 pagesDay 1 NotesPawan KumarNo ratings yet
- Reflection By: Wan Ahmad Fayadh Bin Wan IbrahimDocument3 pagesReflection By: Wan Ahmad Fayadh Bin Wan IbrahimcfghdftNo ratings yet
- Kvs Split Up of Syllabus Class I & IIDocument9 pagesKvs Split Up of Syllabus Class I & IISanjeev MachalNo ratings yet
- Abbotsford Law Court Provincial AdvanceDocument108 pagesAbbotsford Law Court Provincial Advancesampv90No ratings yet
- L.chandra Vs Union of IndiaDocument15 pagesL.chandra Vs Union of IndiaKashish GaurNo ratings yet
- Development of Virtual Museum Model For YouthDocument5 pagesDevelopment of Virtual Museum Model For YouthSoumyadip RoyNo ratings yet
- 865 F.2d 1260 Unpublished DispositionDocument25 pages865 F.2d 1260 Unpublished DispositionScribd Government DocsNo ratings yet
- Sample MemorandumDocument1 pageSample MemorandumAtanaskaNalbantovaNo ratings yet
- Economics SubwayDocument3 pagesEconomics SubwayRaghvi AryaNo ratings yet
- Case Study RubricDocument2 pagesCase Study RubricShainaNo ratings yet
- MSDS Full1 PDFDocument92 pagesMSDS Full1 PDFSunthron SomchaiNo ratings yet
- Differential Equations & Transforms (BMAT102L)Document19 pagesDifferential Equations & Transforms (BMAT102L)Venkat BalajiNo ratings yet
- Liljedahl v. Glassgow, 190 Iowa 827 (1921)Document6 pagesLiljedahl v. Glassgow, 190 Iowa 827 (1921)Jovelan V. EscañoNo ratings yet
- Eco Map 3Document1 pageEco Map 3Ferent Diana-roxanaNo ratings yet
- Public-Key Cryptography: Data and Network Security 1Document15 pagesPublic-Key Cryptography: Data and Network Security 1asadNo ratings yet
- 99 Names of Allah SWT and Mohammed (PBUH)Document11 pages99 Names of Allah SWT and Mohammed (PBUH)api-26870382100% (1)
- Case Studies of Lower Respiratory Tract InfectionsDocument25 pagesCase Studies of Lower Respiratory Tract InfectionsMarianNo ratings yet
- 16SEE - Schedule of PapersDocument36 pages16SEE - Schedule of PapersPiyush Jain0% (1)
- Senior High School 2010Document123 pagesSenior High School 2010John EltNo ratings yet