
Azima: Battery Test
Azima: Battery Test
You might also like
- Battery TestsDocument40 pagesBattery TestsStratiatella Faith Anthony100% (1)
- Instructions For The ABILHAND-Kids Questionnaire The ABILHAND-Kids QuestionnaireDocument12 pagesInstructions For The ABILHAND-Kids Questionnaire The ABILHAND-Kids QuestionnaireFzt Taylan NurluNo ratings yet
- Soap Note 2 Community ClientDocument12 pagesSoap Note 2 Community Clientapi-271984934No ratings yet
- Adult Hemiplegia - Martha BobathDocument185 pagesAdult Hemiplegia - Martha BobathGabriela Marinescu88% (8)
- Activity Analysis Form1 3Document12 pagesActivity Analysis Form1 3api-238169773100% (4)
- 4.perceived Stress Scale (PSS) 14-ItemDocument2 pages4.perceived Stress Scale (PSS) 14-ItemBadGurl GudGirl100% (3)
- Motor Control ApproachesDocument26 pagesMotor Control ApproachesAlyssa ArroyoNo ratings yet
- Spatiotemporal Adaptation Frame of ReferenceDocument10 pagesSpatiotemporal Adaptation Frame of ReferenceKevin Parnala100% (1)
- History of CBRDocument15 pagesHistory of CBRkim100% (3)
- Introduction To Theories of Neurological RehabilitationDocument30 pagesIntroduction To Theories of Neurological RehabilitationHibaAli67% (3)
- Bobath Approach: Concepts and PrinciplesDocument30 pagesBobath Approach: Concepts and PrinciplesJulia SalvioNo ratings yet
- CH 1-Prevention PracticeDocument24 pagesCH 1-Prevention PracticeHafsa AzizNo ratings yet
- Ot Guidelines Child SpecificDocument34 pagesOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Occupational Therapy Initial EvaluationDocument10 pagesOccupational Therapy Initial EvaluationNerissa BanguiNo ratings yet
- Aota Occupational Profile AlexDocument2 pagesAota Occupational Profile Alexapi-37337354550% (2)
- Traumatic Brain Injury Physiotherapy AssessmentDocument20 pagesTraumatic Brain Injury Physiotherapy AssessmentNithin Nair100% (1)
- Marketing Occupational Therapy: Karen JacobsDocument6 pagesMarketing Occupational Therapy: Karen Jacobshazell_aseronNo ratings yet
- 2 Material HandlingDocument218 pages2 Material HandlingJon Blac100% (1)
- AAS Application Form SampleDocument22 pagesAAS Application Form SamplePopy InthavongNo ratings yet
- The Gods of Greece PDFDocument224 pagesThe Gods of Greece PDFCiro Formicola100% (2)
- The Dated Alexander Coinage of Sidon and Ake (1916)Document124 pagesThe Dated Alexander Coinage of Sidon and Ake (1916)Georgian IonNo ratings yet
- Selangor Uniform Building By-Laws 2012 - Sel. P.U. 142-2012 PDFDocument53 pagesSelangor Uniform Building By-Laws 2012 - Sel. P.U. 142-2012 PDFAnwar Yacob67% (3)
- Remediating Motor ControlDocument66 pagesRemediating Motor Controlhis.thunder122100% (3)
- Northwick Park Index of Independence in ADLDocument3 pagesNorthwick Park Index of Independence in ADLIntan Sukecy100% (2)
- Occupational Therapy: Navigation SearchDocument15 pagesOccupational Therapy: Navigation SearchArindam Mondal100% (2)
- Occupational TherapyDocument15 pagesOccupational Therapymanu sethi100% (1)
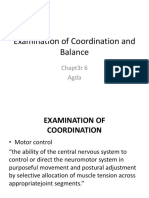
- Examination of Coordination and BalanceDocument27 pagesExamination of Coordination and BalanceBelle AgdaNo ratings yet
- Developmental Approach or Frame of ReferenceDocument27 pagesDevelopmental Approach or Frame of ReferenceHEMA CHANDRAN100% (1)
- Sensory Examination For Physiotherapy Student - NeuroDocument25 pagesSensory Examination For Physiotherapy Student - NeuroAnand VaghasiyaNo ratings yet
- Proprioceptive Neuromuscular FacilitationDocument7 pagesProprioceptive Neuromuscular Facilitationpsionx100% (1)
- LotcaDocument165 pagesLotcaRica Salazar100% (5)
- Constraint Induced Movement Therapy CIMTDocument22 pagesConstraint Induced Movement Therapy CIMTAniqa AsgharNo ratings yet
- Amputation Case StudyDocument10 pagesAmputation Case StudyMegan McCarthy100% (1)
- Brunnstrom'S Movement Therapy in HemiplegiaDocument9 pagesBrunnstrom'S Movement Therapy in HemiplegiaLall JingerppangNo ratings yet
- Polio Physiotherapy NotesDocument6 pagesPolio Physiotherapy NotesyigoNo ratings yet
- Class Teaching Occupational Therapy IDocument15 pagesClass Teaching Occupational Therapy IManoj BalaNo ratings yet
- Coma StimulationDocument18 pagesComa StimulationDarshika Vyas Mohan88% (17)
- Sensory ReeducationDocument52 pagesSensory Reeducationapi-373686592% (26)
- Frame of ReferenceDocument10 pagesFrame of ReferenceGustavo CabanasNo ratings yet
- Part 2: Social Skills Training: RatingDocument3 pagesPart 2: Social Skills Training: RatingGina GucioNo ratings yet
- How To Use AOTA's Mental Health Information SheetsDocument2 pagesHow To Use AOTA's Mental Health Information SheetsThe American Occupational Therapy AssociationNo ratings yet
- Soap NoteDocument1 pageSoap Noteapi-519577267No ratings yet
- Neurological Assessment CaseDocument13 pagesNeurological Assessment Casedrrajmptn0% (1)
- Spinal Cord Injury Assessment Chart (ASIA)Document2 pagesSpinal Cord Injury Assessment Chart (ASIA)cpradheep100% (5)
- Bobath LectureDocument25 pagesBobath Lectureみ にゅきゅ100% (3)
- Combined Cortical SensationsDocument14 pagesCombined Cortical SensationsDyna MaxNo ratings yet
- Occupational Therapy Toolbox Study GuideDocument44 pagesOccupational Therapy Toolbox Study GuideKristian ShumateNo ratings yet
- Rehabilitation in Spinal Cord InjuryDocument2 pagesRehabilitation in Spinal Cord InjuryAudry ArifinNo ratings yet
- Neuro-Developmental TechniqueDocument15 pagesNeuro-Developmental Techniqueapi-442568656100% (1)
- Rood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesDocument3 pagesRood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesShekinah Gracia T. Mosquera100% (2)
- Task Oriented Approach PDFDocument21 pagesTask Oriented Approach PDFAnditaNurfitri0% (1)
- Work and Occupational TherapyDocument31 pagesWork and Occupational Therapysmith197077No ratings yet
- 5 AZIMA HandoutDocument10 pages5 AZIMA HandoutLila BandahalaNo ratings yet
- 3 Shoemyen HandoutDocument9 pages3 Shoemyen HandoutLila BandahalaNo ratings yet
- Phenomenology & Interpretative Phenomenology: Oleh: Dr. Anugriaty Indah AsmaranyDocument30 pagesPhenomenology & Interpretative Phenomenology: Oleh: Dr. Anugriaty Indah AsmaranyUrfa RufaidahNo ratings yet
- Cognitive Synthesis TestDocument33 pagesCognitive Synthesis TestvedroconmioNo ratings yet
- Commentary A Method Used To Train Skeptical VoluntDocument5 pagesCommentary A Method Used To Train Skeptical VoluntCo Bay-AgiNo ratings yet
- Stevenson Meares (1992) An Outcome Study of Psychotherapy For Patients With Borderline Personality DisorderDocument5 pagesStevenson Meares (1992) An Outcome Study of Psychotherapy For Patients With Borderline Personality DisorderbpregerNo ratings yet
- Research ProposalDocument5 pagesResearch Proposalapi-306851259No ratings yet
- House-Tree-Person TestDocument20 pagesHouse-Tree-Person TestJeffrey SniNo ratings yet
- No. 1 PDFDocument251 pagesNo. 1 PDFhasnainNo ratings yet
- Psychoanalytic Therapies: Ronald John Recio Ma Rpsy Emdrprac DaaetsDocument23 pagesPsychoanalytic Therapies: Ronald John Recio Ma Rpsy Emdrprac Daaetsylori dawnNo ratings yet
- Psycho TheatricsDocument9 pagesPsycho TheatricsAdrianaNo ratings yet
- Clarkson 1989Document6 pagesClarkson 1989mato.skurlaNo ratings yet
- Lesson 1 Quantitative IntroductionDocument26 pagesLesson 1 Quantitative Introductionjb sabelinoNo ratings yet
- Psicoterapia Sensoriomotora PDFDocument974 pagesPsicoterapia Sensoriomotora PDFJosé Luis SH100% (4)
- FaceDocument74 pagesFacehazell_aseronNo ratings yet
- The Development of Performance SkillsDocument54 pagesThe Development of Performance Skillshazell_aseronNo ratings yet
- Occupational Therapy Home Safety Intervention Via TelehealthDocument12 pagesOccupational Therapy Home Safety Intervention Via Telehealthhazell_aseronNo ratings yet
- Developmental Milestones:: Motor DevelopmentDocument13 pagesDevelopmental Milestones:: Motor Developmenthazell_aseronNo ratings yet
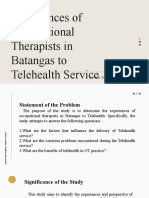
- Experiences of Occupational Therapists in Batangas To Telehealth ServiceDocument29 pagesExperiences of Occupational Therapists in Batangas To Telehealth Servicehazell_aseronNo ratings yet
- Establishing The Legal Framework of Telehealth in The PhilippinesDocument10 pagesEstablishing The Legal Framework of Telehealth in The Philippineshazell_aseronNo ratings yet
- Magsombol, Hazel Anne A. OT2-1 Ankle and Feet BiomechanicsDocument4 pagesMagsombol, Hazel Anne A. OT2-1 Ankle and Feet Biomechanicshazell_aseronNo ratings yet
- Ankle&fEET Written Procedure-MagsombolDocument2 pagesAnkle&fEET Written Procedure-Magsombolhazell_aseronNo ratings yet
- Backward Calculation For Bearing Capacity Estimation of Geogrid Reinforced Foundation by Finite Element MethodDocument13 pagesBackward Calculation For Bearing Capacity Estimation of Geogrid Reinforced Foundation by Finite Element MethodFoolad GharbNo ratings yet
- Word Form KeyDocument2 pagesWord Form KeyHoang Quynh AnhNo ratings yet
- Evans SyndromeDocument13 pagesEvans SyndromerizeviNo ratings yet
- BIZHUB 240f SM PDFDocument355 pagesBIZHUB 240f SM PDFBranga CorneliuNo ratings yet
- 01 Boothe V Director of PatentsDocument3 pages01 Boothe V Director of PatentsPio Guieb AguilarNo ratings yet
- 1 SMDocument12 pages1 SMasdNo ratings yet
- SAS Macro Tutorial ImpDocument27 pagesSAS Macro Tutorial ImpArijit DasNo ratings yet
- Tle Ap-Swine Q3 - WK3 - V4Document7 pagesTle Ap-Swine Q3 - WK3 - V4Maria Rose Tariga Aquino100% (1)
- FRANKL, CROSSLEY, 2000, Gothic Architecture IDocument264 pagesFRANKL, CROSSLEY, 2000, Gothic Architecture IGurunadham MuvvaNo ratings yet
- Is 1079 98Document12 pagesIs 1079 98Rakesh SrivastavaNo ratings yet
- LoB Player Guide Pyram KingDocument15 pagesLoB Player Guide Pyram KingRonaldo SilveiraNo ratings yet
- Wedding Vows - What Do They Really MeanDocument28 pagesWedding Vows - What Do They Really Meanpsykosomatik0% (1)
- 1 A-2 Mann - Concept of Infrastructural PowerDocument11 pages1 A-2 Mann - Concept of Infrastructural Powerrichiflowers11gmail.comNo ratings yet
- How To Install The Data Protector License KeyDocument4 pagesHow To Install The Data Protector License KeyHillary Johnson0% (1)
- Day 2UNQ3-1.docx..bakDocument13 pagesDay 2UNQ3-1.docx..bakAurellia Shafitri100% (1)
- Mortality RateDocument5 pagesMortality Rateamit kumar dewanganNo ratings yet
- Guaranty and Suretyship CasesDocument82 pagesGuaranty and Suretyship Cases001nooneNo ratings yet
- Ecosystem Services From Biodiversity To Society Part 2 1St Edition Bohan Full ChapterDocument67 pagesEcosystem Services From Biodiversity To Society Part 2 1St Edition Bohan Full Chapterharold.eychaner940100% (14)
- Create BAPI TutorialDocument28 pagesCreate BAPI TutorialRoberto Trejos GonzalezNo ratings yet
- Equinix Inc. 2022 Sustainability Report HighlightsDocument25 pagesEquinix Inc. 2022 Sustainability Report HighlightsDaniel ChuaNo ratings yet
- Installing Wonderware InTouch 2014 R2 DevelopmentDocument12 pagesInstalling Wonderware InTouch 2014 R2 DevelopmentARMANDO GALENONo ratings yet
- FRACTAL MARKETS POI Selection)Document1 pageFRACTAL MARKETS POI Selection)malik kondoNo ratings yet
- HRM Project On Engro FoodsDocument20 pagesHRM Project On Engro FoodsSaad MughalNo ratings yet
- MPTH Reviewer Part 1Document27 pagesMPTH Reviewer Part 1Hani VitalesNo ratings yet
- Thesis APDocument31 pagesThesis APIvy SorianoNo ratings yet

































































































Download as pdf or txt
You might also like
- Battery TestsDocument40 pagesBattery TestsStratiatella Faith Anthony100% (1)
- Instructions For The ABILHAND-Kids Questionnaire The ABILHAND-Kids QuestionnaireDocument12 pagesInstructions For The ABILHAND-Kids Questionnaire The ABILHAND-Kids QuestionnaireFzt Taylan NurluNo ratings yet
- Soap Note 2 Community ClientDocument12 pagesSoap Note 2 Community Clientapi-271984934No ratings yet
- Adult Hemiplegia - Martha BobathDocument185 pagesAdult Hemiplegia - Martha BobathGabriela Marinescu88% (8)
- Activity Analysis Form1 3Document12 pagesActivity Analysis Form1 3api-238169773100% (4)
- 4.perceived Stress Scale (PSS) 14-ItemDocument2 pages4.perceived Stress Scale (PSS) 14-ItemBadGurl GudGirl100% (3)
- Motor Control ApproachesDocument26 pagesMotor Control ApproachesAlyssa ArroyoNo ratings yet
- Spatiotemporal Adaptation Frame of ReferenceDocument10 pagesSpatiotemporal Adaptation Frame of ReferenceKevin Parnala100% (1)
- History of CBRDocument15 pagesHistory of CBRkim100% (3)
- Introduction To Theories of Neurological RehabilitationDocument30 pagesIntroduction To Theories of Neurological RehabilitationHibaAli67% (3)
- Bobath Approach: Concepts and PrinciplesDocument30 pagesBobath Approach: Concepts and PrinciplesJulia SalvioNo ratings yet
- CH 1-Prevention PracticeDocument24 pagesCH 1-Prevention PracticeHafsa AzizNo ratings yet
- Ot Guidelines Child SpecificDocument34 pagesOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Occupational Therapy Initial EvaluationDocument10 pagesOccupational Therapy Initial EvaluationNerissa BanguiNo ratings yet
- Aota Occupational Profile AlexDocument2 pagesAota Occupational Profile Alexapi-37337354550% (2)
- Traumatic Brain Injury Physiotherapy AssessmentDocument20 pagesTraumatic Brain Injury Physiotherapy AssessmentNithin Nair100% (1)
- Marketing Occupational Therapy: Karen JacobsDocument6 pagesMarketing Occupational Therapy: Karen Jacobshazell_aseronNo ratings yet
- 2 Material HandlingDocument218 pages2 Material HandlingJon Blac100% (1)
- AAS Application Form SampleDocument22 pagesAAS Application Form SamplePopy InthavongNo ratings yet
- The Gods of Greece PDFDocument224 pagesThe Gods of Greece PDFCiro Formicola100% (2)
- The Dated Alexander Coinage of Sidon and Ake (1916)Document124 pagesThe Dated Alexander Coinage of Sidon and Ake (1916)Georgian IonNo ratings yet
- Selangor Uniform Building By-Laws 2012 - Sel. P.U. 142-2012 PDFDocument53 pagesSelangor Uniform Building By-Laws 2012 - Sel. P.U. 142-2012 PDFAnwar Yacob67% (3)
- Remediating Motor ControlDocument66 pagesRemediating Motor Controlhis.thunder122100% (3)
- Northwick Park Index of Independence in ADLDocument3 pagesNorthwick Park Index of Independence in ADLIntan Sukecy100% (2)
- Occupational Therapy: Navigation SearchDocument15 pagesOccupational Therapy: Navigation SearchArindam Mondal100% (2)
- Occupational TherapyDocument15 pagesOccupational Therapymanu sethi100% (1)
- Examination of Coordination and BalanceDocument27 pagesExamination of Coordination and BalanceBelle AgdaNo ratings yet
- Developmental Approach or Frame of ReferenceDocument27 pagesDevelopmental Approach or Frame of ReferenceHEMA CHANDRAN100% (1)
- Sensory Examination For Physiotherapy Student - NeuroDocument25 pagesSensory Examination For Physiotherapy Student - NeuroAnand VaghasiyaNo ratings yet
- Proprioceptive Neuromuscular FacilitationDocument7 pagesProprioceptive Neuromuscular Facilitationpsionx100% (1)
- LotcaDocument165 pagesLotcaRica Salazar100% (5)
- Constraint Induced Movement Therapy CIMTDocument22 pagesConstraint Induced Movement Therapy CIMTAniqa AsgharNo ratings yet
- Amputation Case StudyDocument10 pagesAmputation Case StudyMegan McCarthy100% (1)
- Brunnstrom'S Movement Therapy in HemiplegiaDocument9 pagesBrunnstrom'S Movement Therapy in HemiplegiaLall JingerppangNo ratings yet
- Polio Physiotherapy NotesDocument6 pagesPolio Physiotherapy NotesyigoNo ratings yet
- Class Teaching Occupational Therapy IDocument15 pagesClass Teaching Occupational Therapy IManoj BalaNo ratings yet
- Coma StimulationDocument18 pagesComa StimulationDarshika Vyas Mohan88% (17)
- Sensory ReeducationDocument52 pagesSensory Reeducationapi-373686592% (26)
- Frame of ReferenceDocument10 pagesFrame of ReferenceGustavo CabanasNo ratings yet
- Part 2: Social Skills Training: RatingDocument3 pagesPart 2: Social Skills Training: RatingGina GucioNo ratings yet
- How To Use AOTA's Mental Health Information SheetsDocument2 pagesHow To Use AOTA's Mental Health Information SheetsThe American Occupational Therapy AssociationNo ratings yet
- Soap NoteDocument1 pageSoap Noteapi-519577267No ratings yet
- Neurological Assessment CaseDocument13 pagesNeurological Assessment Casedrrajmptn0% (1)
- Spinal Cord Injury Assessment Chart (ASIA)Document2 pagesSpinal Cord Injury Assessment Chart (ASIA)cpradheep100% (5)
- Bobath LectureDocument25 pagesBobath Lectureみ にゅきゅ100% (3)
- Combined Cortical SensationsDocument14 pagesCombined Cortical SensationsDyna MaxNo ratings yet
- Occupational Therapy Toolbox Study GuideDocument44 pagesOccupational Therapy Toolbox Study GuideKristian ShumateNo ratings yet
- Rehabilitation in Spinal Cord InjuryDocument2 pagesRehabilitation in Spinal Cord InjuryAudry ArifinNo ratings yet
- Neuro-Developmental TechniqueDocument15 pagesNeuro-Developmental Techniqueapi-442568656100% (1)
- Rood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesDocument3 pagesRood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesShekinah Gracia T. Mosquera100% (2)
- Task Oriented Approach PDFDocument21 pagesTask Oriented Approach PDFAnditaNurfitri0% (1)
- Work and Occupational TherapyDocument31 pagesWork and Occupational Therapysmith197077No ratings yet
- 5 AZIMA HandoutDocument10 pages5 AZIMA HandoutLila BandahalaNo ratings yet
- 3 Shoemyen HandoutDocument9 pages3 Shoemyen HandoutLila BandahalaNo ratings yet
- Phenomenology & Interpretative Phenomenology: Oleh: Dr. Anugriaty Indah AsmaranyDocument30 pagesPhenomenology & Interpretative Phenomenology: Oleh: Dr. Anugriaty Indah AsmaranyUrfa RufaidahNo ratings yet
- Cognitive Synthesis TestDocument33 pagesCognitive Synthesis TestvedroconmioNo ratings yet
- Commentary A Method Used To Train Skeptical VoluntDocument5 pagesCommentary A Method Used To Train Skeptical VoluntCo Bay-AgiNo ratings yet
- Stevenson Meares (1992) An Outcome Study of Psychotherapy For Patients With Borderline Personality DisorderDocument5 pagesStevenson Meares (1992) An Outcome Study of Psychotherapy For Patients With Borderline Personality DisorderbpregerNo ratings yet
- Research ProposalDocument5 pagesResearch Proposalapi-306851259No ratings yet
- House-Tree-Person TestDocument20 pagesHouse-Tree-Person TestJeffrey SniNo ratings yet
- No. 1 PDFDocument251 pagesNo. 1 PDFhasnainNo ratings yet
- Psychoanalytic Therapies: Ronald John Recio Ma Rpsy Emdrprac DaaetsDocument23 pagesPsychoanalytic Therapies: Ronald John Recio Ma Rpsy Emdrprac Daaetsylori dawnNo ratings yet
- Psycho TheatricsDocument9 pagesPsycho TheatricsAdrianaNo ratings yet
- Clarkson 1989Document6 pagesClarkson 1989mato.skurlaNo ratings yet
- Lesson 1 Quantitative IntroductionDocument26 pagesLesson 1 Quantitative Introductionjb sabelinoNo ratings yet
- Psicoterapia Sensoriomotora PDFDocument974 pagesPsicoterapia Sensoriomotora PDFJosé Luis SH100% (4)
- FaceDocument74 pagesFacehazell_aseronNo ratings yet
- The Development of Performance SkillsDocument54 pagesThe Development of Performance Skillshazell_aseronNo ratings yet
- Occupational Therapy Home Safety Intervention Via TelehealthDocument12 pagesOccupational Therapy Home Safety Intervention Via Telehealthhazell_aseronNo ratings yet
- Developmental Milestones:: Motor DevelopmentDocument13 pagesDevelopmental Milestones:: Motor Developmenthazell_aseronNo ratings yet
- Experiences of Occupational Therapists in Batangas To Telehealth ServiceDocument29 pagesExperiences of Occupational Therapists in Batangas To Telehealth Servicehazell_aseronNo ratings yet
- Establishing The Legal Framework of Telehealth in The PhilippinesDocument10 pagesEstablishing The Legal Framework of Telehealth in The Philippineshazell_aseronNo ratings yet
- Magsombol, Hazel Anne A. OT2-1 Ankle and Feet BiomechanicsDocument4 pagesMagsombol, Hazel Anne A. OT2-1 Ankle and Feet Biomechanicshazell_aseronNo ratings yet
- Ankle&fEET Written Procedure-MagsombolDocument2 pagesAnkle&fEET Written Procedure-Magsombolhazell_aseronNo ratings yet
- Backward Calculation For Bearing Capacity Estimation of Geogrid Reinforced Foundation by Finite Element MethodDocument13 pagesBackward Calculation For Bearing Capacity Estimation of Geogrid Reinforced Foundation by Finite Element MethodFoolad GharbNo ratings yet
- Word Form KeyDocument2 pagesWord Form KeyHoang Quynh AnhNo ratings yet
- Evans SyndromeDocument13 pagesEvans SyndromerizeviNo ratings yet
- BIZHUB 240f SM PDFDocument355 pagesBIZHUB 240f SM PDFBranga CorneliuNo ratings yet
- 01 Boothe V Director of PatentsDocument3 pages01 Boothe V Director of PatentsPio Guieb AguilarNo ratings yet
- 1 SMDocument12 pages1 SMasdNo ratings yet
- SAS Macro Tutorial ImpDocument27 pagesSAS Macro Tutorial ImpArijit DasNo ratings yet
- Tle Ap-Swine Q3 - WK3 - V4Document7 pagesTle Ap-Swine Q3 - WK3 - V4Maria Rose Tariga Aquino100% (1)
- FRANKL, CROSSLEY, 2000, Gothic Architecture IDocument264 pagesFRANKL, CROSSLEY, 2000, Gothic Architecture IGurunadham MuvvaNo ratings yet
- Is 1079 98Document12 pagesIs 1079 98Rakesh SrivastavaNo ratings yet
- LoB Player Guide Pyram KingDocument15 pagesLoB Player Guide Pyram KingRonaldo SilveiraNo ratings yet
- Wedding Vows - What Do They Really MeanDocument28 pagesWedding Vows - What Do They Really Meanpsykosomatik0% (1)
- 1 A-2 Mann - Concept of Infrastructural PowerDocument11 pages1 A-2 Mann - Concept of Infrastructural Powerrichiflowers11gmail.comNo ratings yet
- How To Install The Data Protector License KeyDocument4 pagesHow To Install The Data Protector License KeyHillary Johnson0% (1)
- Day 2UNQ3-1.docx..bakDocument13 pagesDay 2UNQ3-1.docx..bakAurellia Shafitri100% (1)
- Mortality RateDocument5 pagesMortality Rateamit kumar dewanganNo ratings yet
- Guaranty and Suretyship CasesDocument82 pagesGuaranty and Suretyship Cases001nooneNo ratings yet
- Ecosystem Services From Biodiversity To Society Part 2 1St Edition Bohan Full ChapterDocument67 pagesEcosystem Services From Biodiversity To Society Part 2 1St Edition Bohan Full Chapterharold.eychaner940100% (14)
- Create BAPI TutorialDocument28 pagesCreate BAPI TutorialRoberto Trejos GonzalezNo ratings yet
- Equinix Inc. 2022 Sustainability Report HighlightsDocument25 pagesEquinix Inc. 2022 Sustainability Report HighlightsDaniel ChuaNo ratings yet
- Installing Wonderware InTouch 2014 R2 DevelopmentDocument12 pagesInstalling Wonderware InTouch 2014 R2 DevelopmentARMANDO GALENONo ratings yet
- FRACTAL MARKETS POI Selection)Document1 pageFRACTAL MARKETS POI Selection)malik kondoNo ratings yet
- HRM Project On Engro FoodsDocument20 pagesHRM Project On Engro FoodsSaad MughalNo ratings yet
- MPTH Reviewer Part 1Document27 pagesMPTH Reviewer Part 1Hani VitalesNo ratings yet
- Thesis APDocument31 pagesThesis APIvy SorianoNo ratings yet