Download as pdf or txt
You might also like
- A Requiem To Mother EarthDocument5 pagesA Requiem To Mother EarthSandra SabuNo ratings yet
- Clinical Reasoning Questions - CollaborationDocument4 pagesClinical Reasoning Questions - CollaborationMohammad OmarNo ratings yet
- Ertapenem (Invanz)Document1 pageErtapenem (Invanz)Adrianne BazoNo ratings yet
- Nursing Care Plan 1Document3 pagesNursing Care Plan 1gagandipkS100% (1)
- Med Template - Ipratropium Bromide AtroventDocument2 pagesMed Template - Ipratropium Bromide AtroventAshlee KeeferNo ratings yet
- Case Study Chapter 37 Anticoagulant and Thrombolytic DrugsDocument1 pageCase Study Chapter 37 Anticoagulant and Thrombolytic DrugsHannaNo ratings yet
- UPSC New Syllabus & Tips To Crack IAS Preliminary & Mains Exam PDFDocument59 pagesUPSC New Syllabus & Tips To Crack IAS Preliminary & Mains Exam PDFPrateek SahniNo ratings yet
- Kleiberit PUR 501 - FISPQDocument8 pagesKleiberit PUR 501 - FISPQYuri SouzaNo ratings yet
- Tutorial Chapter 1 - 0 ThermodynamicDocument2 pagesTutorial Chapter 1 - 0 ThermodynamicSufferedMuchNo ratings yet
- Combizar Drug StudyDocument6 pagesCombizar Drug StudymrnmrsllNo ratings yet
- Drug Study For Cefazolin Drug Data Classificat Ion Mechani SM of Action Indicatio Ns Contraindica Tions Adverse Effect Nursing Responsibil ItiesDocument2 pagesDrug Study For Cefazolin Drug Data Classificat Ion Mechani SM of Action Indicatio Ns Contraindica Tions Adverse Effect Nursing Responsibil ItiesCarl J.No ratings yet
- Zinc OxideDocument4 pagesZinc OxideyundayundaaNo ratings yet
- Drug Study (Pedia)Document7 pagesDrug Study (Pedia)Caurrine Monsalud100% (1)
- Metro Manila Development Screening TestDocument3 pagesMetro Manila Development Screening TestMae PonceNo ratings yet
- Suxamethonium Chloride Injection Bp-PiDocument8 pagesSuxamethonium Chloride Injection Bp-PinanaNo ratings yet
- Drug StudyDocument13 pagesDrug StudylouiseordonoNo ratings yet
- Antimalarial DrugsDocument7 pagesAntimalarial DrugsHilmanNo ratings yet
- SpironolactoneDocument2 pagesSpironolactoneNinoska Garcia-Ortiz100% (1)
- FresofolDocument4 pagesFresofolvedorangeliaNo ratings yet
- Metoclopramide (Reglan)Document1 pageMetoclopramide (Reglan)ENo ratings yet
- Co DiovanDocument2 pagesCo DiovanianecunarNo ratings yet
- MinoxidilDocument2 pagesMinoxidilHenna AhmedNo ratings yet
- Voglibose PiDocument2 pagesVoglibose PiAmit KhuntNo ratings yet
- Trifluridine and TipiracilDocument3 pagesTrifluridine and TipiracilKristine AcasioNo ratings yet
- Piracetam 800mg TabletsDocument5 pagesPiracetam 800mg TabletsSuvaneel MoulickNo ratings yet
- Drug StudyDocument1 pageDrug Studykennethbote0% (1)
- EvistaDocument18 pagesEvistaBrankoPopovićNo ratings yet
- Generic Name TizanidineDocument3 pagesGeneric Name TizanidinemadamcloudnineNo ratings yet
- DRUG STUDY NaproxenDocument1 pageDRUG STUDY NaproxenMargarette Mae VillanuevaNo ratings yet
- Clopidogrel Bisulfate - PlavixDocument2 pagesClopidogrel Bisulfate - PlavixKristi WrayNo ratings yet
- Drug StudyDocument2 pagesDrug Studydwyane0033No ratings yet
- FluconazoleDocument3 pagesFluconazoleMary Kate ClarosNo ratings yet
- BisacodylDocument1 pageBisacodylJewel GutierrezNo ratings yet
- Erythromycin & Pneumococcal VaccineDocument6 pagesErythromycin & Pneumococcal VaccineNikki Joy NavarroNo ratings yet
- Generic NameDocument2 pagesGeneric NamePerdie Branden ReizNo ratings yet
- Drug StudyDocument9 pagesDrug StudyShane Arroyo100% (1)
- Impact of Self Defence Technique Training On Practice of Adolescent GirlsDocument5 pagesImpact of Self Defence Technique Training On Practice of Adolescent GirlsEditor IJTSRDNo ratings yet
- HEMARATE FA Hemarate FA Consists of Folic AcidDocument2 pagesHEMARATE FA Hemarate FA Consists of Folic AcidMarhina Asarabi MukimNo ratings yet
- Q-MED ADRENALINE INJECTION 1 MG - 1 ML PDFDocument2 pagesQ-MED ADRENALINE INJECTION 1 MG - 1 ML PDFchannalingeshaNo ratings yet
- Generic Brand Class Therapeutic Pharmacologic Dosage: PPD's Better Pharmacy Drug Hand Book 9 Edition 2009Document4 pagesGeneric Brand Class Therapeutic Pharmacologic Dosage: PPD's Better Pharmacy Drug Hand Book 9 Edition 2009Crystal Queen MarquezNo ratings yet
- KetoconazoleDocument2 pagesKetoconazolenatinlalaNo ratings yet
- Prio, FNCP, HTPDocument11 pagesPrio, FNCP, HTPEmerick DomingoNo ratings yet
- Nausea and Vomiting Nausea and VomitingDocument6 pagesNausea and Vomiting Nausea and VomitingTHERESA CLAIRE ENCINARESNo ratings yet
- AnastrozoleDocument2 pagesAnastrozoleAnonymous FgT04krgymNo ratings yet
- Mesna: Mesna, Sold Under The BrandDocument17 pagesMesna: Mesna, Sold Under The BrandAndry HamdaniNo ratings yet
- Metformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometDocument5 pagesMetformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometAgronaSlaughterNo ratings yet
- Drug StudyDocument1 pageDrug StudyMaui LopezNo ratings yet
- TENOFOVIR (Tenofovir Disoproxil, Tenofovir Disoproxil Fumarate)Document1 pageTENOFOVIR (Tenofovir Disoproxil, Tenofovir Disoproxil Fumarate)maeNo ratings yet
- Drug StudyDocument8 pagesDrug StudyGian Era100% (1)
- Galvus Met TabDocument23 pagesGalvus Met TabMaria Nicole EconasNo ratings yet
- Drug StudyDocument1 pageDrug StudyDanian AntonioNo ratings yet
- (Generic Name) ® Drotaverine 40mgDocument2 pages(Generic Name) ® Drotaverine 40mgSangar Sardar100% (1)
- Drug StudyDocument6 pagesDrug StudyChickz HunterNo ratings yet
- PROPYLTHIOURACILDocument35 pagesPROPYLTHIOURACILMagdy Ali ELsherbenyNo ratings yet
- Drug Name Mechanism of Action Indications Contraindications Adverse Effect Nursing ConsiderationsDocument2 pagesDrug Name Mechanism of Action Indications Contraindications Adverse Effect Nursing ConsiderationsKatrina PonceNo ratings yet
- Resurrection University Medication CardDocument2 pagesResurrection University Medication CardBohung ConNo ratings yet
- Parul Datta - Pediatric Nursing 5EDocument1 pageParul Datta - Pediatric Nursing 5EmaryNo ratings yet
- Drug Study.Document9 pagesDrug Study.Chelsea Therese GuevarraNo ratings yet
- Lisinopril PDFDocument3 pagesLisinopril PDFHannaNo ratings yet
- Flouxetine Drug StudyDocument7 pagesFlouxetine Drug Studyhello poNo ratings yet
- PALMARES Drug StudyDocument13 pagesPALMARES Drug StudyIvan Jules P. PALMARESNo ratings yet
- Pravastatin SodiumDocument3 pagesPravastatin Sodiumapi-3797941No ratings yet
- Metformin Hydrochloride PDFDocument4 pagesMetformin Hydrochloride PDFHannaNo ratings yet
- Medication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Document43 pagesMedication: Captopril (Capoten) Is An ACE Inhibitor and A Common Antihypertensive. Captopril Generic Name Contents (Hide)Kath Rubio0% (1)
- Labs Drug Study 1Document17 pagesLabs Drug Study 1Drei LanuzoNo ratings yet
- Pericardiocentesis: Why Is This Procedure Done?Document3 pagesPericardiocentesis: Why Is This Procedure Done?HannaNo ratings yet
- Student - Module 9 - Renal AlterationsDocument44 pagesStudent - Module 9 - Renal AlterationsHannaNo ratings yet
- Quizlet 2 PDFDocument2 pagesQuizlet 2 PDFHannaNo ratings yet
- Metabolic AlkalosisDocument1 pageMetabolic AlkalosisHannaNo ratings yet
- Musculoskeletal Questions PDFDocument16 pagesMusculoskeletal Questions PDFHannaNo ratings yet
- Test Results-Chapter 7Document6 pagesTest Results-Chapter 7HannaNo ratings yet
- Neuro Assessment 2.0Document3 pagesNeuro Assessment 2.0HannaNo ratings yet
- Using Prepackaged Sterile KitDocument14 pagesUsing Prepackaged Sterile KitHannaNo ratings yet
- Cardiology VocabularyDocument3 pagesCardiology VocabularyHannaNo ratings yet
- Cardiovascular Drug ProjectDocument3 pagesCardiovascular Drug ProjectHannaNo ratings yet
- Decision Tree - Helping HandDocument3 pagesDecision Tree - Helping HandHannaNo ratings yet
- Badassery For Patho Exam 3Document19 pagesBadassery For Patho Exam 3HannaNo ratings yet
- Suggested Answers To Assignments, Chapter 27, Growth and Development of The Adolescent: 11 To 18 YearsDocument7 pagesSuggested Answers To Assignments, Chapter 27, Growth and Development of The Adolescent: 11 To 18 YearsHannaNo ratings yet
- Suggested Answers To Assignments, Chapter 34, The Dying ChildDocument4 pagesSuggested Answers To Assignments, Chapter 34, The Dying ChildHannaNo ratings yet
- Suggested Answers To Assignments, Chapter 40, The Child With A Musculoskeletal DisorderDocument4 pagesSuggested Answers To Assignments, Chapter 40, The Child With A Musculoskeletal DisorderHannaNo ratings yet
- Suggested Answers To Assignments, Chapter 42, The Child With A Psychosocial DisorderDocument6 pagesSuggested Answers To Assignments, Chapter 42, The Child With A Psychosocial DisorderHannaNo ratings yet
- Delhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsDocument3 pagesDelhi Public School, Greater Noida Pre-Mid Term Exam Class X Mathematics SESSION 2020-21 Set 1 MM: 40 Time: 1.5 Hours InstructionsAnishikaNo ratings yet
- Validation ConceptsDocument41 pagesValidation ConceptsSyed Ghazanfar AliNo ratings yet
- Structural Identification & Poc-1: Topic Page NoDocument35 pagesStructural Identification & Poc-1: Topic Page Nosiddansh100% (1)
- Amina Ahmed Benchmark Solution Oet Writing Task Practice With CorretionDocument1 pageAmina Ahmed Benchmark Solution Oet Writing Task Practice With CorretionFïzã PäthäñNo ratings yet
- Al55 66 Technical Manual v11 EngDocument60 pagesAl55 66 Technical Manual v11 EngProblem VelikiNo ratings yet
- Behaviour of Hollow Core Slabs Under Point LoadsDocument17 pagesBehaviour of Hollow Core Slabs Under Point LoadsVálter LúcioNo ratings yet
- CWAG Rectangular CoordinatesDocument52 pagesCWAG Rectangular CoordinatesRolando MerleNo ratings yet
- BSD-GL-HAL-HMS-100 - (Terms & Definitions)Document42 pagesBSD-GL-HAL-HMS-100 - (Terms & Definitions)Eduard GadzhievNo ratings yet
- Louis I KahnDocument27 pagesLouis I KahnKiran BasuNo ratings yet
- Veins and Hydrothermal DepositsDocument2 pagesVeins and Hydrothermal Depositsalimurtadha100% (1)
- The Fruit Garden CAL: Columbine & AcanthusDocument7 pagesThe Fruit Garden CAL: Columbine & AcanthusMiraNo ratings yet
- Research Progress of The Arti Ficial Intelligence Application in Wastewater Treatment During 2012 - 2022: A Bibliometric AnalysisDocument17 pagesResearch Progress of The Arti Ficial Intelligence Application in Wastewater Treatment During 2012 - 2022: A Bibliometric AnalysisjinxiaohuibabaNo ratings yet
- BEL PE Question Papers For ECE With Answers - 6 Knowledge AddaDocument14 pagesBEL PE Question Papers For ECE With Answers - 6 Knowledge AddaVishwanand ThombareNo ratings yet
- The Normal DistributionDocument30 pagesThe Normal DistributionJohn Rich CaidicNo ratings yet
- Data Transformation by Andy FieldDocument1 pageData Transformation by Andy FieldGon MartNo ratings yet
- EVM TechmaxDocument96 pagesEVM Techmaxnikhileshdhuri97No ratings yet
- 02 - D03 - Basic Funtion of SIPROTEC 5Document7 pages02 - D03 - Basic Funtion of SIPROTEC 5DianaNo ratings yet
- WATERGUARD 45 (Acrylic Waterproofing Coating)Document3 pagesWATERGUARD 45 (Acrylic Waterproofing Coating)Santosh Kumar PatnaikNo ratings yet
- 6 Landforms - SCIENCEDocument9 pages6 Landforms - SCIENCEArianne RealNo ratings yet
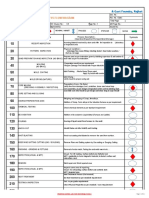
- Process SequenceDocument2 pagesProcess SequenceUmesh SakhareliyaNo ratings yet
- 8210.40 Single Band RET For Multiband Antennas (Controlling White Antenna Array)Document1 page8210.40 Single Band RET For Multiband Antennas (Controlling White Antenna Array)Mohammad AlloushNo ratings yet
- Sewing Skills Checklist PDFDocument44 pagesSewing Skills Checklist PDFyemkem100% (1)
- 1 s2.0 S0264127522004105 MainDocument11 pages1 s2.0 S0264127522004105 MainAsimov RiyazNo ratings yet
- Industrial RoboticsDocument77 pagesIndustrial RoboticsIslam Fouad100% (4)
- Carbohydrates Lecture Bio024Document17 pagesCarbohydrates Lecture Bio024mike angelo albacieteNo ratings yet