Download as pdf or txt
You might also like
- 217 RF Peripheral Neurovascular DysfunctionDocument8 pages217 RF Peripheral Neurovascular Dysfunctionapi-271775750No ratings yet
- Scientific Discussion - En.idDocument9 pagesScientific Discussion - En.idassajadda lizikriNo ratings yet
- Archives of Practical Pediatrics 12Document5 pagesArchives of Practical Pediatrics 12Ashok jainNo ratings yet
- Basic Care & Comfort Nclex RN UwDocument10 pagesBasic Care & Comfort Nclex RN Uwgwen scribd100% (1)
- VT Quick Facts For NCLEX Pediatrics PDFDocument23 pagesVT Quick Facts For NCLEX Pediatrics PDFMerlande Remy90% (10)
- Guia de ConstipacionDocument5 pagesGuia de ConstipacionWalter Barriga ManriqueNo ratings yet
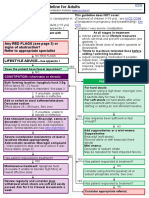
- Laxative Treatment Guideline For AdultsDocument7 pagesLaxative Treatment Guideline For AdultsPurim KTshipNo ratings yet
- Handout Therapy Increased Intestinal Permeability ClinicianDocument2 pagesHandout Therapy Increased Intestinal Permeability ClinicianThe Machi WellnessNo ratings yet
- Constipation Treatment Algorithm For Primary Care Management of Chronic Constipation in AdultsDocument2 pagesConstipation Treatment Algorithm For Primary Care Management of Chronic Constipation in AdultsRuth RNo ratings yet
- Section Constipation - AutosavedDocument46 pagesSection Constipation - Autosavedahmedmls206No ratings yet
- Management of Dehydration (Nsgeud)Document3 pagesManagement of Dehydration (Nsgeud)Mary MenuNo ratings yet
- Summer Training Guide For Pharmacy StudentsDocument129 pagesSummer Training Guide For Pharmacy StudentsDylanSalamNo ratings yet
- GI1026Document3 pagesGI10262pwtqbcynjNo ratings yet
- Methylphenidate March 2018 RevisedDocument14 pagesMethylphenidate March 2018 RevisedEmotional EternalNo ratings yet
- Gastrointestinal System: Antidiarrheals Half-Life: Onset: Peaks: DurationDocument2 pagesGastrointestinal System: Antidiarrheals Half-Life: Onset: Peaks: DurationsyerlyNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanKabang MoaNo ratings yet
- Nursing Care Plan Assessment Diagnosis and Inference Objectives Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis and Inference Objectives Nursing Intervention Rationale Evaluationjay kusainNo ratings yet
- Gifolfox HandoutDocument8 pagesGifolfox Handoutnunuk wijayantiNo ratings yet
- 1.113.medication Administration TimingDocument14 pages1.113.medication Administration TimingSophiaNo ratings yet
- Nursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CityDocument3 pagesNursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CitySoniaMarieBalanayNo ratings yet
- For The Patient: AfatinibDocument5 pagesFor The Patient: Afatinibpriyanka_wataneNo ratings yet
- Nursing Care Plan - CancerDocument3 pagesNursing Care Plan - CancerChristineAla0% (1)
- Gifolfiri Handout 2Document8 pagesGifolfiri Handout 2nunuk wijayantiNo ratings yet
- Anti EmeticsDocument112 pagesAnti Emeticsjoel david knda mjNo ratings yet
- OtcDocument28 pagesOtcsalmayousif11081998No ratings yet
- Management of ConstipationDocument3 pagesManagement of ConstipationFarah Balqis BaragbahNo ratings yet
- Case AnalysisDocument25 pagesCase AnalysisGerly LagutingNo ratings yet
- Lec 7Document21 pagesLec 7Ahmed IsmaillNo ratings yet
- KonstipasiDocument30 pagesKonstipasiJulia MalikaNo ratings yet
- Drug Cards Milk of MagnesiaDocument1 pageDrug Cards Milk of MagnesiaAdrianne Bazo100% (1)
- Pharmacology of The GIT System: CIC Ragasa, RN-MDDocument70 pagesPharmacology of The GIT System: CIC Ragasa, RN-MDCarmencita Ileen Ragasa - AhmedNo ratings yet
- Laxative Guidelines Nov 2013Document2 pagesLaxative Guidelines Nov 2013Purim KTshipNo ratings yet
- Summer Training Guide For Pharmacy StudentsDocument129 pagesSummer Training Guide For Pharmacy Studentstalal150% (2)
- Pharma Bullets NCDocument6 pagesPharma Bullets NCTed ChrisNo ratings yet
- KUSAIN - NCP IN NCM 112 RLE ConstipationDocument2 pagesKUSAIN - NCP IN NCM 112 RLE Constipationjay kusainNo ratings yet
- DiarrhoeaDocument46 pagesDiarrhoeaPrajna TiwariNo ratings yet
- Practical Guide To The Low Histamine Diet PDFDocument8 pagesPractical Guide To The Low Histamine Diet PDFTwinkle DaneNo ratings yet
- Paediatric ConstipationNCP JohnMicah 12216068Document3 pagesPaediatric ConstipationNCP JohnMicah 12216068John MicahNo ratings yet
- Running Head: Client Teaching Wound Care 1Document10 pagesRunning Head: Client Teaching Wound Care 1zoie ziazzetteNo ratings yet
- GI Topic SummaryDocument16 pagesGI Topic SummaryShingie MatemaNo ratings yet
- Brent Hospital and Colleges IncorporatedDocument4 pagesBrent Hospital and Colleges Incorporateddaniel gariandoNo ratings yet
- Drugs Affecting The Body System and Nursing ConsiderationsDocument7 pagesDrugs Affecting The Body System and Nursing ConsiderationsLOVELLE GRACE DE JESUSNo ratings yet
- Health Teaching: Medication Exercise Treatment Hygiene Outpatient DietDocument3 pagesHealth Teaching: Medication Exercise Treatment Hygiene Outpatient DietAl TheóNo ratings yet
- (Ikaw Na Bahala Kung Ano Pipiliin Mo Sa Dalawa Haha) : Irritable Bowel Syndrome (IBS)Document1 page(Ikaw Na Bahala Kung Ano Pipiliin Mo Sa Dalawa Haha) : Irritable Bowel Syndrome (IBS)SDFSAFSADFAFDSAFNo ratings yet
- Tugas DulcolaxDocument2 pagesTugas DulcolaxPriska Nagh Gas-oneNo ratings yet
- Irritable Bowel Syndrome Prescribing GuidanceDocument1 pageIrritable Bowel Syndrome Prescribing Guidancetom8989No ratings yet
- Constipatio 2022-23Document60 pagesConstipatio 2022-23husseinali1rr23No ratings yet
- DGJKHVDocument7 pagesDGJKHVGILIANNE MARIE JIMENEANo ratings yet
- Gerd HTP Bn3aDocument4 pagesGerd HTP Bn3aKristil ChavezNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Constipation: Constipation Fewer Than Three Bowel Movements Per WeekDocument8 pagesConstipation: Constipation Fewer Than Three Bowel Movements Per WeekIbrahim Abdullah100% (1)
- Comprehensive 22-32 EngDocument160 pagesComprehensive 22-32 EngIsna AzizahNo ratings yet
- Constipation Formulary (Otago) : DiagnosisDocument4 pagesConstipation Formulary (Otago) : DiagnosisMiguel SanJuanNo ratings yet
- NCP (Diarrhea)Document2 pagesNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Drugstudy Ms. IbaleDocument23 pagesDrugstudy Ms. IbaleNabor, MelagroseNo ratings yet
- Food for Thought, Health and Weight Loss: The Science Behind DietingFrom EverandFood for Thought, Health and Weight Loss: The Science Behind DietingNo ratings yet
- How to Slim Down: Low Carb Diet Recipes to Lose 5 Pounds In 5 Days, Lower Cholesterol, Eliminate Toxins & Enjoy Your LifeFrom EverandHow to Slim Down: Low Carb Diet Recipes to Lose 5 Pounds In 5 Days, Lower Cholesterol, Eliminate Toxins & Enjoy Your LifeNo ratings yet
- Intermittent Fasting Diet: A Comprehensive Guide to Improved Health and WellnessFrom EverandIntermittent Fasting Diet: A Comprehensive Guide to Improved Health and WellnessNo ratings yet
- Intermittent Fasting Studies: How Does Intermittent Fasting WorkFrom EverandIntermittent Fasting Studies: How Does Intermittent Fasting WorkNo ratings yet
- Gastric Sleeve Cookbook: 77 Delicious and Healthy Gastric Sleeve Recipes with an Easy Guide to Being on the Gastric Sleeve DietFrom EverandGastric Sleeve Cookbook: 77 Delicious and Healthy Gastric Sleeve Recipes with an Easy Guide to Being on the Gastric Sleeve DietNo ratings yet
- 2012 Cleveland Clinic Regional Hospitals EMS ProtocolDocument330 pages2012 Cleveland Clinic Regional Hospitals EMS ProtocolMarian Ioan-LucianNo ratings yet
- Intrathecal Morphine For Analgesia in Minimally Invasive Cardiac Surgery: A Randomized, Placebo-Controlled, Double-Blinded Clinical TrialDocument13 pagesIntrathecal Morphine For Analgesia in Minimally Invasive Cardiac Surgery: A Randomized, Placebo-Controlled, Double-Blinded Clinical TrialLidwina ApyakaNo ratings yet
- Appendix 20 Reporting Form For Transfusion Related Adverse EventDocument4 pagesAppendix 20 Reporting Form For Transfusion Related Adverse Eventmuhamad syafiq SharianNo ratings yet
- Radiology FactSheet ICN907164Document4 pagesRadiology FactSheet ICN907164Vevi VarcetyNo ratings yet
- Hormone HandoutDocument2 pagesHormone Handoutszisz889No ratings yet
- Adherence To Antibiotic Prescription of Dental PatientsDocument9 pagesAdherence To Antibiotic Prescription of Dental PatientsFogellNo ratings yet
- Aids Quiz: The Answer Is DDocument4 pagesAids Quiz: The Answer Is DagarhemantNo ratings yet
- Mental Retardation Lesson PlanDocument10 pagesMental Retardation Lesson Plansp2056251No ratings yet
- Ziabeen ThesisDocument109 pagesZiabeen ThesisHuma Hameed DogarNo ratings yet
- Avocado Seeds BenefitsDocument5 pagesAvocado Seeds Benefitsclonazzyo67% (3)
- Review On DIY Ventilator Using Arduino - Formatted PaperDocument3 pagesReview On DIY Ventilator Using Arduino - Formatted Paperrogergold199No ratings yet
- Active Substance Similar Drugs Dosage Form: Composition:: CapsulesDocument3 pagesActive Substance Similar Drugs Dosage Form: Composition:: CapsulesvalsukhNo ratings yet
- Blood Smears and The Use of Wrights StainDocument5 pagesBlood Smears and The Use of Wrights Stainkaleb16_2No ratings yet
- 1-3rd-BDS-Oral Pathology Syllabus 2020Document7 pages1-3rd-BDS-Oral Pathology Syllabus 2020KhanNo ratings yet
- Dorn TherapyDocument4 pagesDorn Therapymorito2008100% (2)
- nsg-430cc Care Plan 2Document10 pagesnsg-430cc Care Plan 2api-509452165No ratings yet
- Activity-Sheets ParaydayDocument2 pagesActivity-Sheets ParaydayJohn Vincent ParaydayNo ratings yet
- Perinatal GLDocument94 pagesPerinatal GLovidiuroscaNo ratings yet
- Books To DownloadDocument7 pagesBooks To DownloadVishal PatleNo ratings yet
- FTPDocument2 pagesFTPDesta FransiscaNo ratings yet
- Gestational HypertensionDocument71 pagesGestational HypertensionDevikha PeremelNo ratings yet
- Practical Homoeopathy For The People PDFDocument175 pagesPractical Homoeopathy For The People PDFMorgan CabreraNo ratings yet
- Bone TumorsDocument58 pagesBone Tumorsdrqazi777No ratings yet
- Giant Juvenile Fibroadenoma of Breast Mimicking Phylloides Tumour - A Case ReportDocument8 pagesGiant Juvenile Fibroadenoma of Breast Mimicking Phylloides Tumour - A Case ReportsridharNo ratings yet
- Gavin, Nicole - Final Thesis - RedactedDocument245 pagesGavin, Nicole - Final Thesis - RedactedKarlo MedeirosNo ratings yet
- Acupuncture (Acup) : 2017-18 CalendarDocument4 pagesAcupuncture (Acup) : 2017-18 CalendarElanghovan ArumugamNo ratings yet
- Aravind Eye Care SystemDocument3 pagesAravind Eye Care SystemShruti MohapatraNo ratings yet