Download as pdf or txt
You might also like
- Veterinary Pharmacology and Toxicology MCQsDocument18 pagesVeterinary Pharmacology and Toxicology MCQsSunil97% (63)
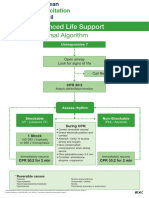
- Advanced Life Support - A0 PDFDocument1 pageAdvanced Life Support - A0 PDFiulia-uroNo ratings yet
- IB Psychology Revision Guide - FINALDocument108 pagesIB Psychology Revision Guide - FINALDhyan Valle93% (14)
- Fundamentals of Nursing Exam 2 (50 Items)Document17 pagesFundamentals of Nursing Exam 2 (50 Items)TamiyaPhil100% (2)
- Reviews: Pre-Eclampsia Part 2: Prediction, Prevention and ManagementDocument10 pagesReviews: Pre-Eclampsia Part 2: Prediction, Prevention and Managementdaeng caturNo ratings yet
- 1 s2.0 S0925443918304861 MainDocument8 pages1 s2.0 S0925443918304861 MainRobert NanNo ratings yet
- Chen2017 PDFDocument26 pagesChen2017 PDFjomoralesr91No ratings yet
- Jurnal MagnesiumDocument6 pagesJurnal MagnesiumkurniaNo ratings yet
- 2261 6189 2 PBDocument6 pages2261 6189 2 PBIip Barudak CikoleNo ratings yet
- Competing Risks Model in Screening For Preeclampsia by Maternal Factors and Biomarkers at 11-13 Weeks GestationDocument12 pagesCompeting Risks Model in Screening For Preeclampsia by Maternal Factors and Biomarkers at 11-13 Weeks GestationmochkurniawanNo ratings yet
- Prediksi Dan Pencegahan PreeklampsiaDocument18 pagesPrediksi Dan Pencegahan PreeklampsiaAsril R. HakimNo ratings yet
- Mean Arterial Blood PressureDocument9 pagesMean Arterial Blood PressureSoniamartilovaNo ratings yet
- Papp A 2Document7 pagesPapp A 2DesyHandayaniNo ratings yet
- Biomarker 2Document8 pagesBiomarker 2Devianti TandialloNo ratings yet
- Ultrasound in Obstet Gyne - 2002 - Aquilina - Improved Early Prediction of Pre Eclampsia by Combining Second TrimesterDocument8 pagesUltrasound in Obstet Gyne - 2002 - Aquilina - Improved Early Prediction of Pre Eclampsia by Combining Second TrimesterMeera Al AliNo ratings yet
- The Relationship Between Hemoglobin and Hematocrit in The First and Second Trimester of Pregnancy and The Incidence of PreeclampsiaDocument3 pagesThe Relationship Between Hemoglobin and Hematocrit in The First and Second Trimester of Pregnancy and The Incidence of PreeclampsiaBaru Chandrasekhar RaoNo ratings yet
- The Relationship of The First and Third Trimester Hematocrit Levels and PreeclampsiaDocument3 pagesThe Relationship of The First and Third Trimester Hematocrit Levels and PreeclampsiaBaru Chandrasekhar RaoNo ratings yet
- A Step Closer To Using Metabolite Biomarkers To ImDocument2 pagesA Step Closer To Using Metabolite Biomarkers To ImNilaaharan RobinsonNo ratings yet
- The Perplexing Pregnancy Disorder Preeclampsia: What Next?: Genetics of Metabolic SyndromeDocument9 pagesThe Perplexing Pregnancy Disorder Preeclampsia: What Next?: Genetics of Metabolic SyndromeNafisatul Khoiriah RafiNo ratings yet
- iTRAQ and PRM-based Quantitative Proteomics in Early Recurrent Spontaneous Abortion: Biomarkers DiscoveryDocument15 pagesiTRAQ and PRM-based Quantitative Proteomics in Early Recurrent Spontaneous Abortion: Biomarkers DiscoverypriyaNo ratings yet
- Jurnal PreeklamsiDocument11 pagesJurnal PreeklamsihexiNo ratings yet
- Pre EclampsiaDocument3 pagesPre EclampsiaFitra HadiNo ratings yet
- Obsgyn 4Document7 pagesObsgyn 4Teguh SulistiyantoNo ratings yet
- Lafalla 2019Document26 pagesLafalla 2019Chicinaș AlexandraNo ratings yet
- COVID-19 and T2DMDocument3 pagesCOVID-19 and T2DMMarijosse NavarroNo ratings yet
- Gene Expression Analysis in Pregnant Women and Their Infants Identifies Unique Fetal Biomarkers That Circulate in Maternal BloodDocument13 pagesGene Expression Analysis in Pregnant Women and Their Infants Identifies Unique Fetal Biomarkers That Circulate in Maternal BloodapalanavedNo ratings yet
- PIIS2589933323002525Document11 pagesPIIS2589933323002525Audrey Madina DewiNo ratings yet
- Reproductive Biology and EndocrinologyDocument4 pagesReproductive Biology and EndocrinologyAnditha Namira RSNo ratings yet
- Biomarker 3Document12 pagesBiomarker 3Devianti TandialloNo ratings yet
- PIIS0002937821019992Document2 pagesPIIS0002937821019992made dharmaNo ratings yet
- Variation in Endoglin Pathway Genes Is Associated With Preeclampsia: A Case - Control Candidate Gene Association StudyDocument9 pagesVariation in Endoglin Pathway Genes Is Associated With Preeclampsia: A Case - Control Candidate Gene Association StudyihdinzNo ratings yet
- AJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Document13 pagesAJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Ana PadillaNo ratings yet
- Abnormal Maternal Apolipoprotein Levels During PreDocument7 pagesAbnormal Maternal Apolipoprotein Levels During Prezeni okta wiyantiNo ratings yet
- Prediction of Preeclampsia Throughout Gestation With Maternal Characteristics and Biophysical and Biochemical Markers: A Longitudinal StudyDocument22 pagesPrediction of Preeclampsia Throughout Gestation With Maternal Characteristics and Biophysical and Biochemical Markers: A Longitudinal StudydhapitstinNo ratings yet
- 50 52 1 SMDocument13 pages50 52 1 SMRicvan Dana Nindrea NindreaNo ratings yet
- Poster Session II: ObjectiveDocument1 pagePoster Session II: ObjectivefujimeisterNo ratings yet
- Banala2020 PDFDocument16 pagesBanala2020 PDFMagic_OverNo ratings yet
- Studyprotocol Open AccessDocument10 pagesStudyprotocol Open AccessMeilin ZulfatinNo ratings yet
- Risk Factors, Early and Late Postpartum Complications of Retained Placenta - A Case Control StudyDocument6 pagesRisk Factors, Early and Late Postpartum Complications of Retained Placenta - A Case Control StudyMuhammad IkbarNo ratings yet
- Screening For Fetal Aneuploidies at 11 To 13 Weeks: ReviewDocument9 pagesScreening For Fetal Aneuploidies at 11 To 13 Weeks: Reviewarturm21No ratings yet
- Is Massive Proteinuria Associated With Maternal An PDFDocument6 pagesIs Massive Proteinuria Associated With Maternal An PDFAmpry LoyraNo ratings yet
- Thrombosis PDFDocument5 pagesThrombosis PDFracopNo ratings yet
- 2013 Chakraborty Outcome of Prelabor Rupture of MembranesDocument6 pages2013 Chakraborty Outcome of Prelabor Rupture of MembranesRayhan AlatasNo ratings yet
- Nugent 2018Document10 pagesNugent 2018TrịnhTrọngTuấnNo ratings yet
- Recent Advances in The Diagnosis and Management of Pre-EclampsiaDocument8 pagesRecent Advances in The Diagnosis and Management of Pre-EclampsiaPulseWangminNo ratings yet
- Management Outcome of Premature Rupture of Membranes in A Tertiary Health Facility in South Western NigeriaDocument7 pagesManagement Outcome of Premature Rupture of Membranes in A Tertiary Health Facility in South Western NigeriaSulis SipinNo ratings yet
- Research Article Placental Expression of NEMO Protein in Normal Pregnancy and PreeclampsiaDocument13 pagesResearch Article Placental Expression of NEMO Protein in Normal Pregnancy and PreeclampsiaAnonymous xEnIDVNo ratings yet
- P ('t':'3', 'I':'668007329') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document5 pagesP ('t':'3', 'I':'668007329') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)niko4eyesNo ratings yet
- Mihu 2015Document7 pagesMihu 2015Nuryasni NuryasniNo ratings yet
- Obstetric Outcome in Preeclampsia: Vasanthi, Nissar Begum, Shamshad BegumDocument1 pageObstetric Outcome in Preeclampsia: Vasanthi, Nissar Begum, Shamshad Begumpavani pNo ratings yet
- Nejmoa2212111 230209 220631Document11 pagesNejmoa2212111 230209 220631Miguel VargasNo ratings yet
- Early Pregnancy Biomarkers in Pre-Eclampsia: A Systematic Review and Meta-AnalysisDocument22 pagesEarly Pregnancy Biomarkers in Pre-Eclampsia: A Systematic Review and Meta-AnalysismochkurniawanNo ratings yet
- Systematic Review Placenta Calcification and Fetal OutcomeDocument22 pagesSystematic Review Placenta Calcification and Fetal OutcomeRizka AdiNo ratings yet
- 100-Article Text-165-1-10-20191127Document6 pages100-Article Text-165-1-10-20191127FATIMAH WANDANo ratings yet
- Antenatal Care of Preeclampsia: From The Inverted Pyramid To The Arrow Model?Document4 pagesAntenatal Care of Preeclampsia: From The Inverted Pyramid To The Arrow Model?Alfa FebriandaNo ratings yet
- Early Prediction and Aspirin For Prevention of Pre-Eclampsia (EPAPP) Study: A Randomized Controlled TrialDocument5 pagesEarly Prediction and Aspirin For Prevention of Pre-Eclampsia (EPAPP) Study: A Randomized Controlled TrialTeguh SulistiyantoNo ratings yet
- 2020 Article 569Document7 pages2020 Article 569GINECOLOGIA OBSTETRICIANo ratings yet
- Mousavi 2018Document6 pagesMousavi 2018Alexandra MateiNo ratings yet
- PSTK 2Document6 pagesPSTK 2subhashbhukyaNo ratings yet
- A Review Article EndocrineDocument14 pagesA Review Article EndocrineJohn DoeNo ratings yet
- Pregnancy HypertensionDocument7 pagesPregnancy HypertensionEgi NabilaNo ratings yet
- 1330 2769 1 SM PDFDocument9 pages1330 2769 1 SM PDFRini Cullen'sNo ratings yet
- Diabetes in Pregnancy: The Complete Guide to ManagementFrom EverandDiabetes in Pregnancy: The Complete Guide to ManagementLisa E. MooreNo ratings yet
- Placental Expression of Vegf, PLGF and Their Receptors in A Model of Placental Insufficiency-Intrauterine Growth Restriction (Pi-Iugr)Document13 pagesPlacental Expression of Vegf, PLGF and Their Receptors in A Model of Placental Insufficiency-Intrauterine Growth Restriction (Pi-Iugr)Feri ZidaneNo ratings yet
- Cell Biology: A. Ahmed, C. Dunk, S. Ahmad and A. KhaliqDocument9 pagesCell Biology: A. Ahmed, C. Dunk, S. Ahmad and A. KhaliqFeri ZidaneNo ratings yet
- Analysis of SEMA3B Methylation and Expression PatternsDocument8 pagesAnalysis of SEMA3B Methylation and Expression PatternsFeri ZidaneNo ratings yet
- The Biology of Preeclampsia: Keizo Kanasaki and Raghu KalluriDocument7 pagesThe Biology of Preeclampsia: Keizo Kanasaki and Raghu KalluriFeri ZidaneNo ratings yet
- Protein Family Review Sema PDFDocument14 pagesProtein Family Review Sema PDFFeri ZidaneNo ratings yet
- Restricted Innervation of Uterus and PlacentaDocument10 pagesRestricted Innervation of Uterus and PlacentaFeri ZidaneNo ratings yet
- Hormonal Regulation and Distinct Functions of Semaphorin-3BDocument21 pagesHormonal Regulation and Distinct Functions of Semaphorin-3BFeri ZidaneNo ratings yet
- Runjan Chetty@uhn On CaDocument17 pagesRunjan Chetty@uhn On CaFeri ZidaneNo ratings yet
- Diagnostic Test Mapeh 7Document5 pagesDiagnostic Test Mapeh 7FAITH HANNAH BERONIONo ratings yet
- 5096 s07 Ms 2Document7 pages5096 s07 Ms 2mstudy1234560% (1)
- Colonel SandersDocument4 pagesColonel SandersHizkia PardosiNo ratings yet
- Bobath Upper LimbDocument12 pagesBobath Upper LimbPrincess Urduja Jimenez-SerranoNo ratings yet
- AGD PPT HermantoDocument33 pagesAGD PPT HermantoWahyu Permata LisaNo ratings yet
- Managment of Trauma Patient in ERDocument46 pagesManagment of Trauma Patient in ERtofanNo ratings yet
- Kidney Transplantation: Group 9 Syazwaniyati Nurulasmira Nur Hamiza Siti NursuhadaDocument12 pagesKidney Transplantation: Group 9 Syazwaniyati Nurulasmira Nur Hamiza Siti NursuhadaSiti Nursuhada binti Mohd AminNo ratings yet
- Latest Thesis. Rough Print12Document107 pagesLatest Thesis. Rough Print12Ajmal Hussain100% (1)
- M7 LN Behavioural Measures of Animal Welfare PDFDocument7 pagesM7 LN Behavioural Measures of Animal Welfare PDFXz RiveraNo ratings yet
- Tracheostomy Guidelines 2018Document97 pagesTracheostomy Guidelines 2018KateCuadraNo ratings yet
- Sociodemographic Data and The Relationship With The Climacteric Symptomatology - Paraiba, Northeast of BrazilDocument8 pagesSociodemographic Data and The Relationship With The Climacteric Symptomatology - Paraiba, Northeast of BrazilInternational Medical PublisherNo ratings yet
- Nursing Philosophy ReflectionDocument7 pagesNursing Philosophy Reflectionapi-480790431No ratings yet
- StemBook 2011 FinalDocument187 pagesStemBook 2011 Finalskeebs23No ratings yet
- List of Important World International Days (2022 Updated)Document53 pagesList of Important World International Days (2022 Updated)Cybot CybotNo ratings yet
- An Introduction To Stem CellsDocument14 pagesAn Introduction To Stem CellsAref DahabrahNo ratings yet
- Chemical Coordination and Integration Handwriten Notes For Neet and JeeDocument5 pagesChemical Coordination and Integration Handwriten Notes For Neet and JeetechnosonicindiaNo ratings yet
- PISMA: A Visual Representation of Motif Distribution in DNA SequencesDocument9 pagesPISMA: A Visual Representation of Motif Distribution in DNA SequencesJesus JimenezNo ratings yet
- 2013 (4 6-59)Document18 pages2013 (4 6-59)Dani GarnidaNo ratings yet
- Thi thử Anh Chuyên Vĩnh Phúc lần 1 tháng 5-2012Document6 pagesThi thử Anh Chuyên Vĩnh Phúc lần 1 tháng 5-2012Trường Học Số100% (1)
- Amtrak Crash Injury DescriptionDocument62 pagesAmtrak Crash Injury DescriptionPhiladelphiaMagazineNo ratings yet
- Marik Covid Protocol SummaryDocument2 pagesMarik Covid Protocol SummaryInternos YopalNo ratings yet
- Case Report 3 MukokelDocument3 pagesCase Report 3 MukokelWidychii GadiestchhetyaNo ratings yet
- Assignment of Pathology 401: Submitted byDocument5 pagesAssignment of Pathology 401: Submitted byaymen gulzarNo ratings yet
- Drop ReqDocument20 pagesDrop Reqwace marikuzaNo ratings yet
- OilsDocument67 pagesOilsNatural2NaturalNo ratings yet
- Cholinergic Agonists VO-BoustanyDocument20 pagesCholinergic Agonists VO-Boustanymarian ghaddarNo ratings yet