Download as docx, pdf, or txt
You might also like
- Project Management Achieving Competitive Advantage 5th Edition Pinto Test BankDocument35 pagesProject Management Achieving Competitive Advantage 5th Edition Pinto Test Bankashleygonzalezcqyxzgwdsa100% (14)
- On Call Surgery On Call Series 4Th Edition Gregg A Adams MD Facs Full ChapterDocument67 pagesOn Call Surgery On Call Series 4Th Edition Gregg A Adams MD Facs Full Chaptersusie.robertson418100% (12)
- 1 - Script Ceu Azul 2023Document21 pages1 - Script Ceu Azul 2023Indigo Graficos50% (2)
- 5 ParotidectomyDocument6 pages5 ParotidectomyAnne MarieNo ratings yet
- Step-By-Step Guide - Minimally Invasive Lumbar Spine Decompression and Dural RepairDocument10 pagesStep-By-Step Guide - Minimally Invasive Lumbar Spine Decompression and Dural RepairPankaj Vatsa100% (1)
- Retromandibular ApproachesDocument8 pagesRetromandibular ApproachesfsjNo ratings yet
- Sling LiftDocument6 pagesSling LiftBFF BotoxNo ratings yet
- Amputation FinalDocument35 pagesAmputation FinalDr Bighnesh DashNo ratings yet
- Short Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial SurgerDocument16 pagesShort Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial Surgerlaljadeff12No ratings yet
- Dorsal SlitDocument5 pagesDorsal SlitarikaNo ratings yet
- Superficial Parotidectomy Through Retrograde Facial Nerve DissectionDocument8 pagesSuperficial Parotidectomy Through Retrograde Facial Nerve DissectionAnonymous LnWIBo1GNo ratings yet
- serdevASMS1 4 2014Document25 pagesserdevASMS1 4 2014Doctores Duarte BarrosNo ratings yet
- Versatility of The Coronal Approach in Maxillofacial Surgery PDFDocument6 pagesVersatility of The Coronal Approach in Maxillofacial Surgery PDFdrgurpal74No ratings yet
- Ilioinguinal Lymphadenectomy: Douglas F. MilamDocument7 pagesIlioinguinal Lymphadenectomy: Douglas F. Milamurovjr vajiraNo ratings yet
- Midcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekDocument11 pagesMidcheek Lift Using Facial Soft-Tissue Spaces of The MidcheekЩербакова ЛенаNo ratings yet
- Cosmetic: Minimal Access Cranial Suspension Lift: A Modified S-LiftDocument13 pagesCosmetic: Minimal Access Cranial Suspension Lift: A Modified S-LiftDini OrdoñezNo ratings yet
- Atlas of Surgical Operations, Parotidectomia - ZollingerDocument10 pagesAtlas of Surgical Operations, Parotidectomia - ZollingerDulce IsmaríNo ratings yet
- Hammond 2009Document9 pagesHammond 2009edkattaNo ratings yet
- Retrosigmoid Approach For Giant Cystic VestibularDocument3 pagesRetrosigmoid Approach For Giant Cystic VestibularTimothy CaldwellNo ratings yet
- P ('t':'3', 'I':'669533173') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document3 pagesP ('t':'3', 'I':'669533173') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)miadexxNo ratings yet
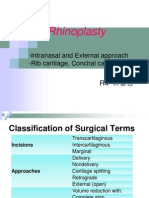
- Rhinoplasty 이홍경Document53 pagesRhinoplasty 이홍경entgo8282No ratings yet
- The Lumbar MicrodiscectomyDocument5 pagesThe Lumbar Microdiscectomyokta fianNo ratings yet
- Abdominal Wall ReconstructionDocument32 pagesAbdominal Wall ReconstructionRahab SaeedNo ratings yet
- 20-3-253 Giampapa 2000 Suturre Suspension Technique Offers PredictableDocument3 pages20-3-253 Giampapa 2000 Suturre Suspension Technique Offers PredictableGustavo MunizNo ratings yet
- ButtockectomyDocument9 pagesButtockectomytatianaNo ratings yet
- Hip DisarticulationDocument13 pagesHip DisarticulationSomeshwar GuptNo ratings yet
- Lelouarn 2007Document10 pagesLelouarn 2007saul iranNo ratings yet
- Surgical Approaches To The Facial Skeleton Mandible and TMJDocument24 pagesSurgical Approaches To The Facial Skeleton Mandible and TMJRagavi VijayaragavanNo ratings yet
- Necklift Fixation To Deep Cervical Fascia and HyoidDocument11 pagesNecklift Fixation To Deep Cervical Fascia and Hyoidrandomaeiou7273No ratings yet
- Satria EngDocument16 pagesSatria EngOjan ARPNo ratings yet
- Types of Abdominal IncisionsDocument3 pagesTypes of Abdominal Incisionsjhuzt4_facebook_343onlyNo ratings yet
- Lateral Rhinotomy and Medial Maxillectomy ApproachDocument5 pagesLateral Rhinotomy and Medial Maxillectomy ApproachNuhu Bankwhot100% (1)
- Rosenwasser - Use of A Pedicled Adipose Flap As A Sling For Anterior Subcutaneous Transposition of The Ulnar NerveDocument4 pagesRosenwasser - Use of A Pedicled Adipose Flap As A Sling For Anterior Subcutaneous Transposition of The Ulnar NervedanielpohlmanNo ratings yet
- ISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasDocument24 pagesISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasVito MasagusNo ratings yet
- Intracorporeal Ribbon Gauze in Laparoscopic SurgeryDocument1 pageIntracorporeal Ribbon Gauze in Laparoscopic Surgeryyacine tarikNo ratings yet
- Full Endoscopic Bilateral Over The Top Decompression in LumbarDocument6 pagesFull Endoscopic Bilateral Over The Top Decompression in Lumbarckilincer2No ratings yet
- Maxillary Sinus LiftingDocument15 pagesMaxillary Sinus Liftinglarisabrinza12No ratings yet
- Surgical Management For Endrometriotic CystsDocument4 pagesSurgical Management For Endrometriotic CystsLadybelle GototosNo ratings yet
- Plastic Surgery: Pablo L. Padilla, Kimberly H. Khoo, Trung Ho, Eric L. Cole, Ramón Zapata Sirvent, Linda G. PhillipsDocument29 pagesPlastic Surgery: Pablo L. Padilla, Kimberly H. Khoo, Trung Ho, Eric L. Cole, Ramón Zapata Sirvent, Linda G. Phillipssportillag1No ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument53 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsNaveed KhanNo ratings yet
- Nava 2006Document8 pagesNava 2006Pasquale ProvaNo ratings yet
- Sesamoids Hallt) X: IPJ OFDocument4 pagesSesamoids Hallt) X: IPJ OFrohitmahaliNo ratings yet
- Surgical Incision Head & NeckDocument31 pagesSurgical Incision Head & Neckromzikerenz0% (1)
- Orchydectomy ItDocument18 pagesOrchydectomy ItMeirisma SimbolonNo ratings yet
- Mastectomy/ Modified Radical Mastectomy: IndicationsDocument6 pagesMastectomy/ Modified Radical Mastectomy: IndicationsNANDAN RAINo ratings yet
- Hemorrhoidectomy: 1. Examination of Anus and Perianal AreaDocument3 pagesHemorrhoidectomy: 1. Examination of Anus and Perianal AreaTeja Laksana NukanaNo ratings yet
- Circumcision Lecture NotesDocument45 pagesCircumcision Lecture NotesRoseNo ratings yet
- Types of IncisionsDocument3 pagesTypes of IncisionsJenny Lyn LimosNo ratings yet
- Surgical Position Supino DecubbitusDocument4 pagesSurgical Position Supino DecubbitusMariana AmayaNo ratings yet
- Salivary Gland Surgery.Document7 pagesSalivary Gland Surgery.Luiz Gabriel SignorelliNo ratings yet
- Internal MastopexyDocument7 pagesInternal MastopexyfumblefumbleNo ratings yet
- Transversus Abdominis Release As An AlternativeDocument2 pagesTransversus Abdominis Release As An AlternativeLuiz ViannaNo ratings yet
- Deltopectoral ApproachDocument4 pagesDeltopectoral ApproachAlex DiconiNo ratings yet
- Parotidectomy 150219224022 Conversion Gate01Document70 pagesParotidectomy 150219224022 Conversion Gate01rajsunmun9No ratings yet
- Koran Da 1988Document4 pagesKoran Da 1988Sanjay RinaNo ratings yet
- Rhytidectomy 060904Document8 pagesRhytidectomy 060904Shirley KoehNo ratings yet
- Nexgen Complete Knee Solution: ZimmerDocument37 pagesNexgen Complete Knee Solution: Zimmerflo1987No ratings yet
- Parotid Ek Tom IDocument25 pagesParotid Ek Tom IYondi Piter PapulungNo ratings yet
- 13 Adductor Muscle Group Excision: Martin Malawer and Paul SugarbakerDocument10 pages13 Adductor Muscle Group Excision: Martin Malawer and Paul SugarbakerSanNo ratings yet
- Safe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalDocument4 pagesSafe and Optimum Steps For Total / Hemi Thyroidectomy: Otolaryngology Open Access JournalJerahmeel Sombilon GenillaNo ratings yet
- NYSORA Thoracic Paravertebral BlockDocument16 pagesNYSORA Thoracic Paravertebral BlockYee Yeow100% (1)
- Ormond 2013Document12 pagesOrmond 2013Hafiz AlfarizieNo ratings yet
- Recipe CreamsDocument1 pageRecipe CreamsfsjNo ratings yet
- RACDS - EXT - ACA - 217 - 1.0 - Membership and Fellowship in Special Dental Practice Handbook - May 2022Document45 pagesRACDS - EXT - ACA - 217 - 1.0 - Membership and Fellowship in Special Dental Practice Handbook - May 2022fsjNo ratings yet
- Sweet Tamarind Chutney RecipeDocument1 pageSweet Tamarind Chutney RecipefsjNo ratings yet
- Persian Love CakeDocument1 pagePersian Love CakefsjNo ratings yet
- Screenshot 2020-08-24 at 12.35.51 PM PDFDocument1 pageScreenshot 2020-08-24 at 12.35.51 PM PDFfsjNo ratings yet
- How To Make Sour Cream RecipeDocument1 pageHow To Make Sour Cream RecipefsjNo ratings yet
- Retromandibular ApproachesDocument8 pagesRetromandibular ApproachesfsjNo ratings yet
- Impressions Materials PDFDocument51 pagesImpressions Materials PDFfsjNo ratings yet
- Full Denture Prob SolvingDocument9 pagesFull Denture Prob SolvingfsjNo ratings yet
- PL1011Sum09 PDFDocument2 pagesPL1011Sum09 PDFfsjNo ratings yet
- PL1030 Sum 09Document1 pagePL1030 Sum 09fsjNo ratings yet
- PL1006Aut03 PDFDocument2 pagesPL1006Aut03 PDFfsjNo ratings yet
- CA Professional and Business License Handbook 6th Ed - 1999Document307 pagesCA Professional and Business License Handbook 6th Ed - 1999Lynx CroweNo ratings yet
- Deploying C++Builder ApplicationsDocument11 pagesDeploying C++Builder ApplicationsalhadeedNo ratings yet
- OS101 ReviewerDocument3 pagesOS101 ReviewerMimi DamascoNo ratings yet
- Medieval PhilosophyDocument52 pagesMedieval PhilosophyMelkamNo ratings yet
- Thermodynamics ReportDocument5 pagesThermodynamics ReportshirlinNo ratings yet
- MCQ On BiomoleculesDocument14 pagesMCQ On BiomoleculesUttkarsha kapoor100% (1)
- Estimate Electrical Guwahati UniversityDocument19 pagesEstimate Electrical Guwahati UniversityTandon Abhilash BorthakurNo ratings yet
- Sarthak GuptaDocument10 pagesSarthak GuptasuyashguptaNo ratings yet
- What MSX - Vol1 No 3 - Autumn 1985Document108 pagesWhat MSX - Vol1 No 3 - Autumn 1985BulesteNo ratings yet
- Enclosed Conductor Rail Boxline Program 0842: WWW - Conductix.UsDocument28 pagesEnclosed Conductor Rail Boxline Program 0842: WWW - Conductix.UsElsad HuseynovNo ratings yet
- 1 Enterprise Lan Switching Cisco Ccna 200 125 200 105 m1 SlidesDocument65 pages1 Enterprise Lan Switching Cisco Ccna 200 125 200 105 m1 SlidesMiticuta SurubNo ratings yet
- National Museum of RwandaDocument4 pagesNational Museum of Rwandajonah BanalekakiNo ratings yet
- Biography of Gabriela SilangDocument2 pagesBiography of Gabriela SilangAngel MonjasNo ratings yet
- Freight Chargers CalclationDocument2 pagesFreight Chargers CalclationAkama KulasekaraNo ratings yet
- List Rickt Divx (01 - 09 10)Document22 pagesList Rickt Divx (01 - 09 10)Mila MulianiNo ratings yet
- ISO 31010. Técnicas Evaluación RiesgosDocument6 pagesISO 31010. Técnicas Evaluación Riesgosmarta suanchez gil0% (1)
- Enraf-Nonius Manumed Basic ENDocument16 pagesEnraf-Nonius Manumed Basic ENFlexxxy SssNo ratings yet
- MR Certification CurriculumDocument5 pagesMR Certification CurriculumJunaid RazzaqNo ratings yet
- Adeshwar Nursing Institute Khamhargaon, Jagdalpur: Community Health Nursing Lesson Plan ON Wound DressingDocument8 pagesAdeshwar Nursing Institute Khamhargaon, Jagdalpur: Community Health Nursing Lesson Plan ON Wound DressingNitesh BhuraNo ratings yet
- Cases 4-6Document13 pagesCases 4-6CHAN SIN JIANNo ratings yet
- Learning Styles and Learning PreferencesDocument32 pagesLearning Styles and Learning Preferencespatterson nji mbakwaNo ratings yet
- IPG Fall 2014 Spanish TitlesDocument100 pagesIPG Fall 2014 Spanish TitlesIndependent Publishers GroupNo ratings yet
- Milkfish Cage Culture Flyer PDFDocument2 pagesMilkfish Cage Culture Flyer PDFPrincess FontillasNo ratings yet
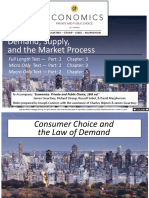
- Demand, Supply, and The Market Process: Full Length Text - Micro Only Text - Macro Only TextDocument66 pagesDemand, Supply, and The Market Process: Full Length Text - Micro Only Text - Macro Only TextCeline YoonNo ratings yet
- The Importance of TeamworkDocument8 pagesThe Importance of TeamworkBraga MihaelaNo ratings yet
- Info Pompe Pistonase PDFDocument44 pagesInfo Pompe Pistonase PDFMarin GarazNo ratings yet
- TCS NQT Part4Document5 pagesTCS NQT Part4djustinlivingstonNo ratings yet