Download as pdf or txt
You might also like
- Đề Cương Môn Tiếng Anh Chuyên Ngành Ngành: DượcDocument11 pagesĐề Cương Môn Tiếng Anh Chuyên Ngành Ngành: DượcNguyễn Thị Hương75% (8)
- CHN Final PaperDocument151 pagesCHN Final PaperJose Bryan NacillaNo ratings yet
- Individual Task: Ayman I. Mohadali BSMT - 1Document5 pagesIndividual Task: Ayman I. Mohadali BSMT - 1Sheima Ainie JuripaeNo ratings yet
- Fundamentals NotesDocument23 pagesFundamentals NotesElle R Naceno100% (5)
- Who Leprosy Control BurdenDocument44 pagesWho Leprosy Control BurdenClaire SoletaNo ratings yet
- Psychiatric Nursing 1Document17 pagesPsychiatric Nursing 1Marichu BajadoNo ratings yet
- Dengue Fever in The PhilippinesDocument27 pagesDengue Fever in The PhilippinesDale Marie RenomeronNo ratings yet
- Medina College College of Medical Technology Thesis Writing QuestionnaireDocument5 pagesMedina College College of Medical Technology Thesis Writing QuestionnaireDhanimie FayeNo ratings yet
- Running Head: Factors Influencing Vaccine Hesitancy 1Document18 pagesRunning Head: Factors Influencing Vaccine Hesitancy 1api-395650878No ratings yet
- The Problem: (Insert Citation)Document52 pagesThe Problem: (Insert Citation)Trisha100% (1)
- WHO Mental Health System in The PhilippinesDocument26 pagesWHO Mental Health System in The PhilippinesVERA FilesNo ratings yet
- Nursing Care PlanDocument44 pagesNursing Care PlanBiway RegalaNo ratings yet
- Department of Health - Leprosy Control Program - 2011-11-08Document9 pagesDepartment of Health - Leprosy Control Program - 2011-11-08daryl ann dep-asNo ratings yet
- TRESIBADocument16 pagesTRESIBARaina96No ratings yet
- Chapters1 5 Appendix (1) - Sample ThesisDocument94 pagesChapters1 5 Appendix (1) - Sample ThesisJohnrey Tesoro100% (5)
- Factors Influencing Community Participation in Healthcare ProgramsDocument40 pagesFactors Influencing Community Participation in Healthcare ProgramsBest Research50% (2)
- Degree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentDocument24 pagesDegree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentRJ DealcaNo ratings yet
- Impact of Pandemic To The Psychological Aspects of Nursing StudentsDocument25 pagesImpact of Pandemic To The Psychological Aspects of Nursing StudentsBrandon AreteNo ratings yet
- Research PaperDocument28 pagesResearch PapertaniamanansalabautistaNo ratings yet
- LHQW Korea ChinaDocument7 pagesLHQW Korea ChinaFebie DevinaNo ratings yet
- BipolarDocument7 pagesBipolarFikayoOjoNo ratings yet
- Type 1 Diabetes Mellitus Nael HernandezDocument15 pagesType 1 Diabetes Mellitus Nael HernandezShermayne Mallapre HernandezNo ratings yet
- FINAL Nursing ThesisDocument67 pagesFINAL Nursing ThesisAgronaSlaughter0% (1)
- PMCH I-Kwento Ni RosarioDocument1 pagePMCH I-Kwento Ni RosarioNix BatallerNo ratings yet
- Cultural Beliefs On Disease Causation in The PhilippinesDocument19 pagesCultural Beliefs On Disease Causation in The PhilippinesDexter ReyesNo ratings yet
- Clinical Case 04 2019Document12 pagesClinical Case 04 2019Erica Veluz LuyunNo ratings yet
- Drug and NCPDocument15 pagesDrug and NCPgeelawlietNo ratings yet
- Process RecordingsDocument4 pagesProcess RecordingsJayakrishnan P KripNo ratings yet
- Anaphylactic ReactionDocument9 pagesAnaphylactic ReactionZahir Jayvee Gayak IINo ratings yet
- Reflection Paper On NETIQUETTE - Mind Your Manners On Social NetworkDocument1 pageReflection Paper On NETIQUETTE - Mind Your Manners On Social NetworkNichelle HustayaNo ratings yet
- Week 14 - CD Course Task 8Document1 pageWeek 14 - CD Course Task 8Rochelle TenederoNo ratings yet
- PathophysiologyDocument9 pagesPathophysiologySuzette PipoNo ratings yet
- Running Head: Elder Assessment 1Document13 pagesRunning Head: Elder Assessment 1api-4190916620% (1)
- She Was A: 1. Health Perception - Health Management PatternDocument9 pagesShe Was A: 1. Health Perception - Health Management PatternJo Marchianne PigarNo ratings yet
- Essay On The Importance of Mental Health ParityDocument1 pageEssay On The Importance of Mental Health ParityPrince BatiocoNo ratings yet
- Principles of ImmunizationDocument4 pagesPrinciples of ImmunizationDoc Prince CaballeroNo ratings yet
- VIADO PortfolioDocument97 pagesVIADO PortfolioROANN MAE VIADONo ratings yet
- 69 Current Philippine Health SituationDocument51 pages69 Current Philippine Health SituationkatlisayNo ratings yet
- SYNTHESISDocument2 pagesSYNTHESISairish catindigNo ratings yet
- Schizophrenia Paper FinalDocument9 pagesSchizophrenia Paper Finalapi-277268224No ratings yet
- ImmunizationDocument36 pagesImmunizationshahbaz100% (8)
- Framework For Maternal and Child Health NursingDocument18 pagesFramework For Maternal and Child Health NursingKristil ChavezNo ratings yet
- Health Promotion of The ElderlyDocument16 pagesHealth Promotion of The ElderlyCarloAragonNo ratings yet
- Cyber Crime - An EssayDocument2 pagesCyber Crime - An EssayEr. Hebin RajNo ratings yet
- 314 Lecture Module RevDocument92 pages314 Lecture Module RevMaica LectanaNo ratings yet
- Nursing Informatics in TaiwanDocument3 pagesNursing Informatics in TaiwanKrishia HidalgoNo ratings yet
- Beneficence NonmaleficenceDocument1 pageBeneficence NonmaleficenceggalicinaoNo ratings yet
- Case Analysis On Geriatrics FinalDocument30 pagesCase Analysis On Geriatrics Final3D - AURELIO, Lyca Mae M.No ratings yet
- NCMB 314 Finals ReviewerDocument24 pagesNCMB 314 Finals ReviewerANGELICA MACASONo ratings yet
- Research - Group4 - BSN3 1 1 1Document119 pagesResearch - Group4 - BSN3 1 1 1ruth samuel0% (1)
- Process RecordingDocument6 pagesProcess RecordingteuuuuNo ratings yet
- Alcohol Dependence SyndromeDocument3 pagesAlcohol Dependence SyndromeMohd AminuddinNo ratings yet
- Defense MechanismsDocument4 pagesDefense MechanismsEiziddeen IsmailNo ratings yet
- Acute Renal Failure 2Document56 pagesAcute Renal Failure 2Jeeca O. Veloso100% (1)
- Craniotomy: Memdova, Monette A. Bsn-3B Llevado, Emielou A. Bsn-3BDocument26 pagesCraniotomy: Memdova, Monette A. Bsn-3B Llevado, Emielou A. Bsn-3BMonette Abalos MendovaNo ratings yet
- Upper Gastrointestinal BleedingDocument32 pagesUpper Gastrointestinal BleedinglicservernoidaNo ratings yet
- Western Mindanao State University College of Nursing Zamboanga CityDocument4 pagesWestern Mindanao State University College of Nursing Zamboanga CityEzra LambarteNo ratings yet
- History of Community Health NursingDocument35 pagesHistory of Community Health NursingAgung setiawan100% (1)
- Drug Index Updated2Document113 pagesDrug Index Updated2tam meiNo ratings yet
- Burnout Syndrome Among Undergraduate Nursing Students at A Public University PDFDocument8 pagesBurnout Syndrome Among Undergraduate Nursing Students at A Public University PDFRaise RaiseNo ratings yet
- Fluoracil Drug StudyDocument3 pagesFluoracil Drug StudyNicole Louize CaloraNo ratings yet
- HIV Thesis Sample IntroductionDocument2 pagesHIV Thesis Sample IntroductionVane UcatNo ratings yet
- Childrens Uniform Mental Health Assessment CUMHA 1Document14 pagesChildrens Uniform Mental Health Assessment CUMHA 1Hira WarsiNo ratings yet
- Xpulse 200 FI (ABWD) - (May 2019)Document86 pagesXpulse 200 FI (ABWD) - (May 2019)krishna SarmaNo ratings yet
- Catalog of Tools For Assessing and Addressing Vaccine HesitancyDocument10 pagesCatalog of Tools For Assessing and Addressing Vaccine Hesitancykrishna SarmaNo ratings yet
- Block Panchayath DivisionsDocument6 pagesBlock Panchayath Divisionskrishna SarmaNo ratings yet
- Kerala Paddy Wetland ActDocument14 pagesKerala Paddy Wetland Actkrishna SarmaNo ratings yet
- Letter of Invitation For The ReactorDocument2 pagesLetter of Invitation For The ReactorImmah PinedaNo ratings yet
- Organizational Chart of Davao Doctors CollegeDocument1 pageOrganizational Chart of Davao Doctors CollegeKristoffer Castro-DNo ratings yet
- CENSUSDocument16 pagesCENSUSDiana GorospeNo ratings yet
- SCAI SHOCK Bedside Checklist 2022Document1 pageSCAI SHOCK Bedside Checklist 2022Katherine AzocarNo ratings yet
- Special Categories For Nomination/Reservation: (A) Special Categories Are Not Applicable To The Following CoursesDocument1 pageSpecial Categories For Nomination/Reservation: (A) Special Categories Are Not Applicable To The Following CoursesAkshara RathoreNo ratings yet
- History of UphsDocument3 pagesHistory of UphsDIANE EDRANo ratings yet
- Mkell DNP Project 9-16Document2 pagesMkell DNP Project 9-16Miserable*No ratings yet
- Health status of refugees and migrants in turkey: an evidence review of published scientific papers Daniele Mipatrini, Matteo Dembech, Sarp Uner, Samer Jabbour, Altin Malaj, Toker Erguder, Evis Kasapi, Pavel Ursu, Dorit Nitzan, Nedret EmirogluDocument30 pagesHealth status of refugees and migrants in turkey: an evidence review of published scientific papers Daniele Mipatrini, Matteo Dembech, Sarp Uner, Samer Jabbour, Altin Malaj, Toker Erguder, Evis Kasapi, Pavel Ursu, Dorit Nitzan, Nedret EmirogluAnonymous qgJBUnLURNo ratings yet
- 2 Banas-Nograles v. Comelec - G.R. No. 246328, 10 September 2019Document15 pages2 Banas-Nograles v. Comelec - G.R. No. 246328, 10 September 2019Bee CGNo ratings yet
- Introduction To Hospital Pharmacy: OutlineDocument12 pagesIntroduction To Hospital Pharmacy: OutlinePrincess TiongsonNo ratings yet
- Diabetes and Ocular Disease Past, Present, and Future TherapiesDocument534 pagesDiabetes and Ocular Disease Past, Present, and Future TherapiesHealthCare100% (2)
- Geron Group 1 ReportingDocument13 pagesGeron Group 1 ReportingPotato TomatoNo ratings yet
- Albert EllisDocument8 pagesAlbert EllisGaurish SalgaocarNo ratings yet
- CEKA AttachmentsDocument6 pagesCEKA AttachmentsPavithra balasubramaniNo ratings yet
- Sing and Plur NounsDocument8 pagesSing and Plur NounsJuan Carlos JCNo ratings yet
- Tamil Nadu Private Clinical Establishments (Regulation) Amendment Act, 2018.Document6 pagesTamil Nadu Private Clinical Establishments (Regulation) Amendment Act, 2018.ShivramNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Nursing Diagnosis Objective Intervention Rationale Evaluationmyer pasandalanNo ratings yet
- Training Manual PsychologistsDocument75 pagesTraining Manual PsychologistsNagarjuna KalimisettyNo ratings yet
- SLT Ca Ts TC ExDocument1 pageSLT Ca Ts TC ExMahmoud AtefNo ratings yet
- Measles Management Guidelines - 091222-1Document14 pagesMeasles Management Guidelines - 091222-1Tushar AmbedareNo ratings yet
- New Age Careers Careers That Didnt Exist 20 Yr Ago PDFDocument16 pagesNew Age Careers Careers That Didnt Exist 20 Yr Ago PDFHariom KushwahNo ratings yet
- Febuxostat Mylan Epar Public Assessment Report - enDocument28 pagesFebuxostat Mylan Epar Public Assessment Report - entomas.palominosNo ratings yet
- Nursing Diagnosis - Wikipedia, The Free EncyclopediaDocument9 pagesNursing Diagnosis - Wikipedia, The Free EncyclopediaDika YolandaNo ratings yet
- Management of The Rhesus Negative MotherDocument32 pagesManagement of The Rhesus Negative MothertotalpregnancycareNo ratings yet
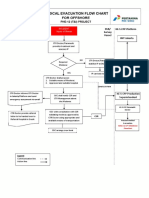
- 3-A4 - Medical Evacuation Flow Chart (Rev.0)Document1 page3-A4 - Medical Evacuation Flow Chart (Rev.0)SiskaNo ratings yet
- Indo-German Newsletter 02Document5 pagesIndo-German Newsletter 02Bulbul SharmaNo ratings yet
- Ot Guidelines ParkinsonDocument145 pagesOt Guidelines ParkinsonFanny100% (1)