
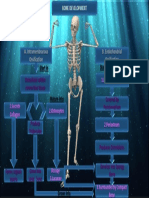
NEW Bone Production AND Periosteal Reacti On : New Bone Within A Host Bone May Appear
NEW Bone Production AND Periosteal Reacti On : New Bone Within A Host Bone May Appear
You might also like
- MOHID Matric Result CardDocument1 pageMOHID Matric Result CardAwais Chohan75% (4)
- Medical Terminology For Health Care Professionals A Word Building Approach 9th Edition Rice Test BankDocument33 pagesMedical Terminology For Health Care Professionals A Word Building Approach 9th Edition Rice Test Bankjamesbyrdcxgsaioymf100% (15)
- Virtual Long Bone DissectionDocument2 pagesVirtual Long Bone Dissectionapi-434039561No ratings yet
- G.R. No. 5887, U.S. v. Look Chaw, 18 Phil. 573 (Case Digest)Document1 pageG.R. No. 5887, U.S. v. Look Chaw, 18 Phil. 573 (Case Digest)MarisseAnne CoquillaNo ratings yet
- Os AugmentDocument5 pagesOs AugmentsalehalsadiNo ratings yet
- Classification Assessment Signs and Symptoms Anatomy and PhysiologyDocument1 pageClassification Assessment Signs and Symptoms Anatomy and PhysiologykyawNo ratings yet
- Bone Regeneration: Dr. José María Aguado Dra. Stefania Arena Dra. Rocío GrandeDocument58 pagesBone Regeneration: Dr. José María Aguado Dra. Stefania Arena Dra. Rocío GrandeZineb SqualliNo ratings yet
- Bone-Grafting MaterialsDocument10 pagesBone-Grafting MaterialsSaiful FirdausNo ratings yet
- Study About The Development of The Temporomandibular Joint in The Human FetusesDocument6 pagesStudy About The Development of The Temporomandibular Joint in The Human FetusesChristianEdwarZuñigaNo ratings yet
- Healing Following Implant Surgery: Osseous Healing-Early PhaseDocument2 pagesHealing Following Implant Surgery: Osseous Healing-Early PhaseUrjita PatilNo ratings yet
- This Study Resource Was: Dr. MALIJAN - The Skeletal and Articular System The Skull and Cranial FossaeDocument6 pagesThis Study Resource Was: Dr. MALIJAN - The Skeletal and Articular System The Skull and Cranial FossaeNovz FaustinoNo ratings yet
- Skeletal SystemDocument70 pagesSkeletal SystemHannah Bless SalvadorNo ratings yet
- Gen Histo Topic 6 BonesDocument4 pagesGen Histo Topic 6 BonesShania CandelarioNo ratings yet
- Hereditary Multiple Exostoses: Current Insights: Orthopedic Research and Reviews DoveDocument13 pagesHereditary Multiple Exostoses: Current Insights: Orthopedic Research and Reviews DoveEga AihenaNo ratings yet
- Virtual Long Bone DissectionDocument2 pagesVirtual Long Bone Dissectionapi-438665079No ratings yet
- Cods 2015 07 064Document7 pagesCods 2015 07 064محمود مساعدحلمى أبازيدNo ratings yet
- Kon Et Al-1969-Journal of PeriodontologyDocument16 pagesKon Et Al-1969-Journal of Periodontologyshir keshalesNo ratings yet
- THE SKELETAL SYSTEM I - Bone TissueDocument2 pagesTHE SKELETAL SYSTEM I - Bone TissueAmirah AnfNo ratings yet
- Clinical Aspects of Anatomy - 1Document4 pagesClinical Aspects of Anatomy - 1AakashNo ratings yet
- JIAP Apr 10 07-019 AlGhamdi pp39-44Document6 pagesJIAP Apr 10 07-019 AlGhamdi pp39-44noufabdulaziz00No ratings yet
- Schultz YPA 2001Document42 pagesSchultz YPA 2001Paulina AlvarezNo ratings yet
- Anatomy - Physiology (Chapter 6 - Skeletal System)Document43 pagesAnatomy - Physiology (Chapter 6 - Skeletal System)Kyla DuenaNo ratings yet
- Bone Tissue & Mascular TissueDocument5 pagesBone Tissue & Mascular TissueJanjan GarcesNo ratings yet
- 3-Drugs Used in Osteoporosis (Final)Document18 pages3-Drugs Used in Osteoporosis (Final)Lana AmerieNo ratings yet
- Truly Light-Force MechanicsDocument4 pagesTruly Light-Force MechanicsVijaylaxmi MendigeriNo ratings yet
- Cranial Suture Lineage and Contributions To RepairDocument9 pagesCranial Suture Lineage and Contributions To RepairRamya DivyaNo ratings yet
- Healing of Tooth Extraction Socket: Dr. Pankaj Datta Dr. Shilpa Khullar Dr. Mittal ADocument3 pagesHealing of Tooth Extraction Socket: Dr. Pankaj Datta Dr. Shilpa Khullar Dr. Mittal AwatidinaNo ratings yet
- Pawar Bone DevelopmentDocument1 pagePawar Bone DevelopmentKuldip PawarNo ratings yet
- SKELETAL Anatomy AfnaksnfkansfnasDocument4 pagesSKELETAL Anatomy AfnaksnfkansfnasJglacier godNo ratings yet
- The Epiphyseal Plate: Physiology, Anatomy, and TraumaDocument12 pagesThe Epiphyseal Plate: Physiology, Anatomy, and TraumaLaura Mérida CáceresNo ratings yet
- Bone2008 HinduDocument2 pagesBone2008 HinduCharlie ShiNo ratings yet
- Oral Radiology - DENT 445 - Benign Tumors of The Jaws - Reading MaterialDocument39 pagesOral Radiology - DENT 445 - Benign Tumors of The Jaws - Reading MaterialiWellyFoxNo ratings yet
- The Skeletal SystemDocument5 pagesThe Skeletal SystemCharlie CharlesNo ratings yet
- 02 - Anatomy of Bone and Fracture HealingDocument5 pages02 - Anatomy of Bone and Fracture HealingABCDEFG HIJKLMNOPNo ratings yet
- Module 5 - Body TissuesDocument7 pagesModule 5 - Body TissuesGoogle BackupNo ratings yet
- Skeletal System Skeletal Anatomy: (Typical)Document10 pagesSkeletal System Skeletal Anatomy: (Typical)anon_660872041No ratings yet
- A0 แนวตั้งDocument1 pageA0 แนวตั้งaukwan7904No ratings yet
- Concept Map of Bone Formation, Growth, and RemodellingDocument1 pageConcept Map of Bone Formation, Growth, and RemodellingSylvanus Rein LangreoNo ratings yet
- Skeletal System TransesDocument11 pagesSkeletal System Transesadrielvamos28No ratings yet
- Structure Function Structure Function: GreenDocument3 pagesStructure Function Structure Function: GreenReggieNo ratings yet
- Anatomy - Physiology (Chapter 6 - Skeletal System)Document39 pagesAnatomy - Physiology (Chapter 6 - Skeletal System)Avi ZychNo ratings yet
- Ana126 2Document6 pagesAna126 2sophiashrzNo ratings yet
- BONESDocument2 pagesBONESCATHRYN MAE GAYLANNo ratings yet
- WEEK 6 TRANS AnaphyDocument13 pagesWEEK 6 TRANS AnaphygazzyngsalvadorNo ratings yet
- OsteogensisDocument10 pagesOsteogensisDaniela OliverosNo ratings yet
- HUESOSDocument22 pagesHUESOSmacarena vignaNo ratings yet
- Bone-Healing Pattern at The Surface of Titanium Implants - An Experimental Study in The Dog - RossiDocument8 pagesBone-Healing Pattern at The Surface of Titanium Implants - An Experimental Study in The Dog - Rossidiego aguilarNo ratings yet
- Biología Celular Metabolismo OseoDocument12 pagesBiología Celular Metabolismo Oseoandreaelisa17No ratings yet
- Osteosarcoma 3Document10 pagesOsteosarcoma 3Erick Eduardo Enciso ChavezNo ratings yet
- Behrents The Influence of The Trigeminal Nerve On Facial Growth and DevelopmentDocument8 pagesBehrents The Influence of The Trigeminal Nerve On Facial Growth and DevelopmentNataly ComettaNo ratings yet
- Skeletal System Functions of The Skeletal System: Human Anatomy & Physiology Kylie Jan C. SilvaDocument15 pagesSkeletal System Functions of The Skeletal System: Human Anatomy & Physiology Kylie Jan C. SilvaKert trocioNo ratings yet
- Bone Tissue: OsteocytesDocument11 pagesBone Tissue: OsteocytesA18- Jessa Mae DayagNo ratings yet
- (1976) Melcher. On The Repair Potential of Periodontal TissuesDocument5 pages(1976) Melcher. On The Repair Potential of Periodontal TissuesDaniel EchegarayNo ratings yet
- Skeletal System ReviewerDocument14 pagesSkeletal System ReviewerDaniel DanielNo ratings yet
- Anatomy and Physiology of The Skeletal SystemDocument12 pagesAnatomy and Physiology of The Skeletal SystemalxrezxNo ratings yet
- Stenosis and Homeopathy - DR Debra KatchenDocument7 pagesStenosis and Homeopathy - DR Debra KatchenSangram007No ratings yet
- Phillips and Verano 2011Document4 pagesPhillips and Verano 2011Kendy Huallpamaita CárdenasNo ratings yet
- Basic Knowledge of Bone Grafting: March 2012Document29 pagesBasic Knowledge of Bone Grafting: March 2012Nadira NurinNo ratings yet
- Case Study: Netflix: SummaryDocument3 pagesCase Study: Netflix: SummaryThaise CortesNo ratings yet
- Bone Grafting With Coralline HydroxyapatiteDocument11 pagesBone Grafting With Coralline HydroxyapatiteFellicia RachmadianaNo ratings yet
- Taphonomic and Ecologic Information From Bone WeatheringDocument13 pagesTaphonomic and Ecologic Information From Bone WeatheringLola CarrerNo ratings yet
- New Bone Formation Using An Extracted ToothDocument8 pagesNew Bone Formation Using An Extracted ToothDaniela LilloNo ratings yet
- Joint Function Preservation: A Focus on the Osteochondral UnitFrom EverandJoint Function Preservation: A Focus on the Osteochondral UnitNo ratings yet
- Shopping Mall Shopping MallDocument8 pagesShopping Mall Shopping MallRafidah mkNo ratings yet
- Embodied Yoga Principles Posture Guide Author Embodied Yoga Principles Online Teacher TrainingDocument222 pagesEmbodied Yoga Principles Posture Guide Author Embodied Yoga Principles Online Teacher TrainingKartheek ChandraNo ratings yet
- Division Memorandum - s2020 - 220 PDFDocument16 pagesDivision Memorandum - s2020 - 220 PDFARLENE MARASIGANNo ratings yet
- Report Opr - 584 107Document34 pagesReport Opr - 584 107maximuspalpatineNo ratings yet
- Padanan KataDocument3 pagesPadanan Katabk28oktober19282 smkNo ratings yet
- Arthur Edward Waite - The Pictorial Key To The TarotDocument111 pagesArthur Edward Waite - The Pictorial Key To The TarotFran DossinNo ratings yet
- CSC 2105: D S I: ATA Tructure NtroductionDocument22 pagesCSC 2105: D S I: ATA Tructure NtroductionFahim AhmedNo ratings yet
- Mataria - Engineering Research JournalDocument5 pagesMataria - Engineering Research JournalAwadHilmyNo ratings yet
- Culture of HaryanaDocument2 pagesCulture of HaryanaanittaNo ratings yet
- Decimal Series: 1 Naya Paisa Copper Nickle IssueDocument8 pagesDecimal Series: 1 Naya Paisa Copper Nickle IssueSeshadri VenkatNo ratings yet
- PHILOSOPHY 11 Q1 Week5 - 6 MELC7 8 MOD Mabuti Elizabeth and Obrero Daniel Daniel ObreroDocument19 pagesPHILOSOPHY 11 Q1 Week5 - 6 MELC7 8 MOD Mabuti Elizabeth and Obrero Daniel Daniel ObreroWilma DamoNo ratings yet
- Kinematics Analysis OF Robots (Part 2) : Eng4406 Robotics and Machine VisionDocument30 pagesKinematics Analysis OF Robots (Part 2) : Eng4406 Robotics and Machine VisionANSHUMAN KUMARNo ratings yet
- Document 3Document2 pagesDocument 3ANKIT KUMAR DUBEYNo ratings yet
- General System TheoryDocument307 pagesGeneral System TheoryCarlos Luiz100% (3)
- PW Select October 2016Document22 pagesPW Select October 2016Publishers WeeklyNo ratings yet
- Unit 4 Company Law Unit 4 Company LawDocument42 pagesUnit 4 Company Law Unit 4 Company LawRanjan BaradurNo ratings yet
- General FOB CIF Contract-02 - 3 - 2020 PDFDocument11 pagesGeneral FOB CIF Contract-02 - 3 - 2020 PDFKhánh Linh Mai Trần100% (1)
- Chapter 1 Toxins - Kill The Primates, Rule The World. Or: Don't Turn Your Back On A Fungus!Document9 pagesChapter 1 Toxins - Kill The Primates, Rule The World. Or: Don't Turn Your Back On A Fungus!Eved1981 superrito.comNo ratings yet
- Narrative Medicine Form Function and EthicsDocument5 pagesNarrative Medicine Form Function and EthicsPetruta FlangeaNo ratings yet
- Company Profile PT. Simtex Mechatronic IndojayaDocument63 pagesCompany Profile PT. Simtex Mechatronic IndojayaAriMooskyterNo ratings yet
- UCC1Document2 pagesUCC1windykern100% (2)
- Fiber Optic Cable Outdoor,: Bellcomms BellcommsDocument1 pageFiber Optic Cable Outdoor,: Bellcomms BellcommsChawengsak ChoomuangNo ratings yet
- Đề Khảo Sát Chất Lượng Lần 1 Năm Học 2018-2019Document29 pagesĐề Khảo Sát Chất Lượng Lần 1 Năm Học 2018-2019Vu Tien ManhNo ratings yet
- 05 Május.-Uj-Beo-AlapDocument16 pages05 Május.-Uj-Beo-AlapPéter MészárosNo ratings yet
- Packet Sniffer in Python: Import SocketDocument9 pagesPacket Sniffer in Python: Import SocketRihab BenabdelazizNo ratings yet
- Gerunds - and - Infinitives Anton Salazar GelbertDocument2 pagesGerunds - and - Infinitives Anton Salazar GelbertGELBERT GELY ANTON SALAZARNo ratings yet
- IUFD For 4th Year Medical StudentsDocument19 pagesIUFD For 4th Year Medical StudentsDegefaw BikoyNo ratings yet
























































































Download as pdf or txt
You might also like
- MOHID Matric Result CardDocument1 pageMOHID Matric Result CardAwais Chohan75% (4)
- Medical Terminology For Health Care Professionals A Word Building Approach 9th Edition Rice Test BankDocument33 pagesMedical Terminology For Health Care Professionals A Word Building Approach 9th Edition Rice Test Bankjamesbyrdcxgsaioymf100% (15)
- Virtual Long Bone DissectionDocument2 pagesVirtual Long Bone Dissectionapi-434039561No ratings yet
- G.R. No. 5887, U.S. v. Look Chaw, 18 Phil. 573 (Case Digest)Document1 pageG.R. No. 5887, U.S. v. Look Chaw, 18 Phil. 573 (Case Digest)MarisseAnne CoquillaNo ratings yet
- Os AugmentDocument5 pagesOs AugmentsalehalsadiNo ratings yet
- Classification Assessment Signs and Symptoms Anatomy and PhysiologyDocument1 pageClassification Assessment Signs and Symptoms Anatomy and PhysiologykyawNo ratings yet
- Bone Regeneration: Dr. José María Aguado Dra. Stefania Arena Dra. Rocío GrandeDocument58 pagesBone Regeneration: Dr. José María Aguado Dra. Stefania Arena Dra. Rocío GrandeZineb SqualliNo ratings yet
- Bone-Grafting MaterialsDocument10 pagesBone-Grafting MaterialsSaiful FirdausNo ratings yet
- Study About The Development of The Temporomandibular Joint in The Human FetusesDocument6 pagesStudy About The Development of The Temporomandibular Joint in The Human FetusesChristianEdwarZuñigaNo ratings yet
- Healing Following Implant Surgery: Osseous Healing-Early PhaseDocument2 pagesHealing Following Implant Surgery: Osseous Healing-Early PhaseUrjita PatilNo ratings yet
- This Study Resource Was: Dr. MALIJAN - The Skeletal and Articular System The Skull and Cranial FossaeDocument6 pagesThis Study Resource Was: Dr. MALIJAN - The Skeletal and Articular System The Skull and Cranial FossaeNovz FaustinoNo ratings yet
- Skeletal SystemDocument70 pagesSkeletal SystemHannah Bless SalvadorNo ratings yet
- Gen Histo Topic 6 BonesDocument4 pagesGen Histo Topic 6 BonesShania CandelarioNo ratings yet
- Hereditary Multiple Exostoses: Current Insights: Orthopedic Research and Reviews DoveDocument13 pagesHereditary Multiple Exostoses: Current Insights: Orthopedic Research and Reviews DoveEga AihenaNo ratings yet
- Virtual Long Bone DissectionDocument2 pagesVirtual Long Bone Dissectionapi-438665079No ratings yet
- Cods 2015 07 064Document7 pagesCods 2015 07 064محمود مساعدحلمى أبازيدNo ratings yet
- Kon Et Al-1969-Journal of PeriodontologyDocument16 pagesKon Et Al-1969-Journal of Periodontologyshir keshalesNo ratings yet
- THE SKELETAL SYSTEM I - Bone TissueDocument2 pagesTHE SKELETAL SYSTEM I - Bone TissueAmirah AnfNo ratings yet
- Clinical Aspects of Anatomy - 1Document4 pagesClinical Aspects of Anatomy - 1AakashNo ratings yet
- JIAP Apr 10 07-019 AlGhamdi pp39-44Document6 pagesJIAP Apr 10 07-019 AlGhamdi pp39-44noufabdulaziz00No ratings yet
- Schultz YPA 2001Document42 pagesSchultz YPA 2001Paulina AlvarezNo ratings yet
- Anatomy - Physiology (Chapter 6 - Skeletal System)Document43 pagesAnatomy - Physiology (Chapter 6 - Skeletal System)Kyla DuenaNo ratings yet
- Bone Tissue & Mascular TissueDocument5 pagesBone Tissue & Mascular TissueJanjan GarcesNo ratings yet
- 3-Drugs Used in Osteoporosis (Final)Document18 pages3-Drugs Used in Osteoporosis (Final)Lana AmerieNo ratings yet
- Truly Light-Force MechanicsDocument4 pagesTruly Light-Force MechanicsVijaylaxmi MendigeriNo ratings yet
- Cranial Suture Lineage and Contributions To RepairDocument9 pagesCranial Suture Lineage and Contributions To RepairRamya DivyaNo ratings yet
- Healing of Tooth Extraction Socket: Dr. Pankaj Datta Dr. Shilpa Khullar Dr. Mittal ADocument3 pagesHealing of Tooth Extraction Socket: Dr. Pankaj Datta Dr. Shilpa Khullar Dr. Mittal AwatidinaNo ratings yet
- Pawar Bone DevelopmentDocument1 pagePawar Bone DevelopmentKuldip PawarNo ratings yet
- SKELETAL Anatomy AfnaksnfkansfnasDocument4 pagesSKELETAL Anatomy AfnaksnfkansfnasJglacier godNo ratings yet
- The Epiphyseal Plate: Physiology, Anatomy, and TraumaDocument12 pagesThe Epiphyseal Plate: Physiology, Anatomy, and TraumaLaura Mérida CáceresNo ratings yet
- Bone2008 HinduDocument2 pagesBone2008 HinduCharlie ShiNo ratings yet
- Oral Radiology - DENT 445 - Benign Tumors of The Jaws - Reading MaterialDocument39 pagesOral Radiology - DENT 445 - Benign Tumors of The Jaws - Reading MaterialiWellyFoxNo ratings yet
- The Skeletal SystemDocument5 pagesThe Skeletal SystemCharlie CharlesNo ratings yet
- 02 - Anatomy of Bone and Fracture HealingDocument5 pages02 - Anatomy of Bone and Fracture HealingABCDEFG HIJKLMNOPNo ratings yet
- Module 5 - Body TissuesDocument7 pagesModule 5 - Body TissuesGoogle BackupNo ratings yet
- Skeletal System Skeletal Anatomy: (Typical)Document10 pagesSkeletal System Skeletal Anatomy: (Typical)anon_660872041No ratings yet
- A0 แนวตั้งDocument1 pageA0 แนวตั้งaukwan7904No ratings yet
- Concept Map of Bone Formation, Growth, and RemodellingDocument1 pageConcept Map of Bone Formation, Growth, and RemodellingSylvanus Rein LangreoNo ratings yet
- Skeletal System TransesDocument11 pagesSkeletal System Transesadrielvamos28No ratings yet
- Structure Function Structure Function: GreenDocument3 pagesStructure Function Structure Function: GreenReggieNo ratings yet
- Anatomy - Physiology (Chapter 6 - Skeletal System)Document39 pagesAnatomy - Physiology (Chapter 6 - Skeletal System)Avi ZychNo ratings yet
- Ana126 2Document6 pagesAna126 2sophiashrzNo ratings yet
- BONESDocument2 pagesBONESCATHRYN MAE GAYLANNo ratings yet
- WEEK 6 TRANS AnaphyDocument13 pagesWEEK 6 TRANS AnaphygazzyngsalvadorNo ratings yet
- OsteogensisDocument10 pagesOsteogensisDaniela OliverosNo ratings yet
- HUESOSDocument22 pagesHUESOSmacarena vignaNo ratings yet
- Bone-Healing Pattern at The Surface of Titanium Implants - An Experimental Study in The Dog - RossiDocument8 pagesBone-Healing Pattern at The Surface of Titanium Implants - An Experimental Study in The Dog - Rossidiego aguilarNo ratings yet
- Biología Celular Metabolismo OseoDocument12 pagesBiología Celular Metabolismo Oseoandreaelisa17No ratings yet
- Osteosarcoma 3Document10 pagesOsteosarcoma 3Erick Eduardo Enciso ChavezNo ratings yet
- Behrents The Influence of The Trigeminal Nerve On Facial Growth and DevelopmentDocument8 pagesBehrents The Influence of The Trigeminal Nerve On Facial Growth and DevelopmentNataly ComettaNo ratings yet
- Skeletal System Functions of The Skeletal System: Human Anatomy & Physiology Kylie Jan C. SilvaDocument15 pagesSkeletal System Functions of The Skeletal System: Human Anatomy & Physiology Kylie Jan C. SilvaKert trocioNo ratings yet
- Bone Tissue: OsteocytesDocument11 pagesBone Tissue: OsteocytesA18- Jessa Mae DayagNo ratings yet
- (1976) Melcher. On The Repair Potential of Periodontal TissuesDocument5 pages(1976) Melcher. On The Repair Potential of Periodontal TissuesDaniel EchegarayNo ratings yet
- Skeletal System ReviewerDocument14 pagesSkeletal System ReviewerDaniel DanielNo ratings yet
- Anatomy and Physiology of The Skeletal SystemDocument12 pagesAnatomy and Physiology of The Skeletal SystemalxrezxNo ratings yet
- Stenosis and Homeopathy - DR Debra KatchenDocument7 pagesStenosis and Homeopathy - DR Debra KatchenSangram007No ratings yet
- Phillips and Verano 2011Document4 pagesPhillips and Verano 2011Kendy Huallpamaita CárdenasNo ratings yet
- Basic Knowledge of Bone Grafting: March 2012Document29 pagesBasic Knowledge of Bone Grafting: March 2012Nadira NurinNo ratings yet
- Case Study: Netflix: SummaryDocument3 pagesCase Study: Netflix: SummaryThaise CortesNo ratings yet
- Bone Grafting With Coralline HydroxyapatiteDocument11 pagesBone Grafting With Coralline HydroxyapatiteFellicia RachmadianaNo ratings yet
- Taphonomic and Ecologic Information From Bone WeatheringDocument13 pagesTaphonomic and Ecologic Information From Bone WeatheringLola CarrerNo ratings yet
- New Bone Formation Using An Extracted ToothDocument8 pagesNew Bone Formation Using An Extracted ToothDaniela LilloNo ratings yet
- Joint Function Preservation: A Focus on the Osteochondral UnitFrom EverandJoint Function Preservation: A Focus on the Osteochondral UnitNo ratings yet
- Shopping Mall Shopping MallDocument8 pagesShopping Mall Shopping MallRafidah mkNo ratings yet
- Embodied Yoga Principles Posture Guide Author Embodied Yoga Principles Online Teacher TrainingDocument222 pagesEmbodied Yoga Principles Posture Guide Author Embodied Yoga Principles Online Teacher TrainingKartheek ChandraNo ratings yet
- Division Memorandum - s2020 - 220 PDFDocument16 pagesDivision Memorandum - s2020 - 220 PDFARLENE MARASIGANNo ratings yet
- Report Opr - 584 107Document34 pagesReport Opr - 584 107maximuspalpatineNo ratings yet
- Padanan KataDocument3 pagesPadanan Katabk28oktober19282 smkNo ratings yet
- Arthur Edward Waite - The Pictorial Key To The TarotDocument111 pagesArthur Edward Waite - The Pictorial Key To The TarotFran DossinNo ratings yet
- CSC 2105: D S I: ATA Tructure NtroductionDocument22 pagesCSC 2105: D S I: ATA Tructure NtroductionFahim AhmedNo ratings yet
- Mataria - Engineering Research JournalDocument5 pagesMataria - Engineering Research JournalAwadHilmyNo ratings yet
- Culture of HaryanaDocument2 pagesCulture of HaryanaanittaNo ratings yet
- Decimal Series: 1 Naya Paisa Copper Nickle IssueDocument8 pagesDecimal Series: 1 Naya Paisa Copper Nickle IssueSeshadri VenkatNo ratings yet
- PHILOSOPHY 11 Q1 Week5 - 6 MELC7 8 MOD Mabuti Elizabeth and Obrero Daniel Daniel ObreroDocument19 pagesPHILOSOPHY 11 Q1 Week5 - 6 MELC7 8 MOD Mabuti Elizabeth and Obrero Daniel Daniel ObreroWilma DamoNo ratings yet
- Kinematics Analysis OF Robots (Part 2) : Eng4406 Robotics and Machine VisionDocument30 pagesKinematics Analysis OF Robots (Part 2) : Eng4406 Robotics and Machine VisionANSHUMAN KUMARNo ratings yet
- Document 3Document2 pagesDocument 3ANKIT KUMAR DUBEYNo ratings yet
- General System TheoryDocument307 pagesGeneral System TheoryCarlos Luiz100% (3)
- PW Select October 2016Document22 pagesPW Select October 2016Publishers WeeklyNo ratings yet
- Unit 4 Company Law Unit 4 Company LawDocument42 pagesUnit 4 Company Law Unit 4 Company LawRanjan BaradurNo ratings yet
- General FOB CIF Contract-02 - 3 - 2020 PDFDocument11 pagesGeneral FOB CIF Contract-02 - 3 - 2020 PDFKhánh Linh Mai Trần100% (1)
- Chapter 1 Toxins - Kill The Primates, Rule The World. Or: Don't Turn Your Back On A Fungus!Document9 pagesChapter 1 Toxins - Kill The Primates, Rule The World. Or: Don't Turn Your Back On A Fungus!Eved1981 superrito.comNo ratings yet
- Narrative Medicine Form Function and EthicsDocument5 pagesNarrative Medicine Form Function and EthicsPetruta FlangeaNo ratings yet
- Company Profile PT. Simtex Mechatronic IndojayaDocument63 pagesCompany Profile PT. Simtex Mechatronic IndojayaAriMooskyterNo ratings yet
- UCC1Document2 pagesUCC1windykern100% (2)
- Fiber Optic Cable Outdoor,: Bellcomms BellcommsDocument1 pageFiber Optic Cable Outdoor,: Bellcomms BellcommsChawengsak ChoomuangNo ratings yet
- Đề Khảo Sát Chất Lượng Lần 1 Năm Học 2018-2019Document29 pagesĐề Khảo Sát Chất Lượng Lần 1 Năm Học 2018-2019Vu Tien ManhNo ratings yet
- 05 Május.-Uj-Beo-AlapDocument16 pages05 Május.-Uj-Beo-AlapPéter MészárosNo ratings yet
- Packet Sniffer in Python: Import SocketDocument9 pagesPacket Sniffer in Python: Import SocketRihab BenabdelazizNo ratings yet
- Gerunds - and - Infinitives Anton Salazar GelbertDocument2 pagesGerunds - and - Infinitives Anton Salazar GelbertGELBERT GELY ANTON SALAZARNo ratings yet
- IUFD For 4th Year Medical StudentsDocument19 pagesIUFD For 4th Year Medical StudentsDegefaw BikoyNo ratings yet