
Screening For Type 2 Diabetes Mellitus - UpToDate
Screening For Type 2 Diabetes Mellitus - UpToDate
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
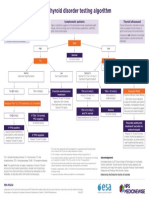
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 pageNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHNo ratings yet
- Clinical Presentation, Diagnosis, and Initial Evaluation of Diabetes Mellitus in Adults - UpToDateDocument21 pagesClinical Presentation, Diagnosis, and Initial Evaluation of Diabetes Mellitus in Adults - UpToDatePriscillaNo ratings yet
- Management of Diabetic Foot Ulcers - UpToDateDocument40 pagesManagement of Diabetic Foot Ulcers - UpToDatePriscillaNo ratings yet
- Overview of Treatment of Chronic Wounds - UpToDateDocument35 pagesOverview of Treatment of Chronic Wounds - UpToDatePriscillaNo ratings yet
- Clinical Staging and Management of Pressure-Induced Skin and Soft Tissue Injury - UpToDateDocument31 pagesClinical Staging and Management of Pressure-Induced Skin and Soft Tissue Injury - UpToDatePriscillaNo ratings yet
- Basic Principles of Wound Management - UpToDateDocument44 pagesBasic Principles of Wound Management - UpToDatePriscillaNo ratings yet
- Approach To The Differential Diagnosis of Leg Ulcers - UpToDateDocument44 pagesApproach To The Differential Diagnosis of Leg Ulcers - UpToDatePriscillaNo ratings yet
- Overview of The Treatment of Insomnia in Adults - UpToDateDocument24 pagesOverview of The Treatment of Insomnia in Adults - UpToDatePriscillaNo ratings yet
- Presentation 1Document6 pagesPresentation 1Maya RentinaNo ratings yet
- Endocrine PDFDocument450 pagesEndocrine PDFmariatiNo ratings yet
- VWA - Contemporary Management of Diabetes MellitusDocument46 pagesVWA - Contemporary Management of Diabetes MellitusVincenzina SoósNo ratings yet
- Pediatric Type 1 Diabetes MellitusDocument25 pagesPediatric Type 1 Diabetes MellitusmuhammadferhatNo ratings yet
- Pathophysiology of Type II Diabetes MellitusDocument7 pagesPathophysiology of Type II Diabetes Mellituschinthaka18389021No ratings yet
- Carbohydrate Metabolism - MCQs 4 BDocument10 pagesCarbohydrate Metabolism - MCQs 4 BSaroja Veeresh100% (1)
- SF 81Document2 pagesSF 81Keian EstalaneNo ratings yet
- CHMP Post Authorisation Summary Positive Opinion Mounjaro II 07 - enDocument2 pagesCHMP Post Authorisation Summary Positive Opinion Mounjaro II 07 - enFRUNZANo ratings yet
- A Case Study Submitted in Partial Fulfilment of The Requirements in Capstone ProjectDocument5 pagesA Case Study Submitted in Partial Fulfilment of The Requirements in Capstone Projectedison savellanoNo ratings yet
- Care of Adults 26 Endocrine ManagementDocument26 pagesCare of Adults 26 Endocrine ManagementGaras AnnaBerniceNo ratings yet
- Hospital Discharge Algorithm Based On Admission Hba For The Management of Patients With Type 2 DiabetesDocument6 pagesHospital Discharge Algorithm Based On Admission Hba For The Management of Patients With Type 2 DiabetesxtineNo ratings yet
- 8428 60351 3 PBDocument10 pages8428 60351 3 PBdika dayantiNo ratings yet
- Nama: Malsa Ramadhaniah NPM:222205102Document2 pagesNama: Malsa Ramadhaniah NPM:222205102MalsaNo ratings yet
- Protocol For Intensive Intravenous Insulin Infusion For ICUDocument2 pagesProtocol For Intensive Intravenous Insulin Infusion For ICUburlacuraduuNo ratings yet
- Lecture 6 Carbohydrate MetabolismDocument36 pagesLecture 6 Carbohydrate MetabolismDuduetsang MosalakataneNo ratings yet
- Diabetic Ketoacidosis in ChildrenDocument39 pagesDiabetic Ketoacidosis in ChildrenRichard SiahaanNo ratings yet
- Pcos Biology PaperDocument5 pagesPcos Biology Paperapi-241521552No ratings yet
- DM and Oncology Semi Finals QuizDocument15 pagesDM and Oncology Semi Finals QuizKaren mae alvarroNo ratings yet
- SnehaDocument3 pagesSneharazeena salamNo ratings yet
- Diabetic Awareness Day ProposalDocument6 pagesDiabetic Awareness Day ProposalMaizura NazarudinNo ratings yet
- Thyroid HormonesDocument2 pagesThyroid HormonesLara MieNo ratings yet
- Diabetes20171011 112709Document2 pagesDiabetes20171011 112709ROYNo ratings yet
- NUR 201 Diabetes PowerpointDocument53 pagesNUR 201 Diabetes PowerpointSaad MotawéaNo ratings yet
- Thyroid ReportDocument105 pagesThyroid ReportAARVNo ratings yet
- Mauritius NCD Survey 2015 ReportDocument56 pagesMauritius NCD Survey 2015 Reportsaima.maiharaubNo ratings yet
- T31 - Types of Diabetes and Diagnosis - PTPDocument6 pagesT31 - Types of Diabetes and Diagnosis - PTPangela adelantarNo ratings yet
- Group 8 Sedentary Lifestyle - SampleDocument16 pagesGroup 8 Sedentary Lifestyle - SamplebondbondNo ratings yet
- Sas 34Document3 pagesSas 34Sistine Rose LabajoNo ratings yet
- PexDocument4 pagesPextagastaNo ratings yet












































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 pageNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHNo ratings yet
- Clinical Presentation, Diagnosis, and Initial Evaluation of Diabetes Mellitus in Adults - UpToDateDocument21 pagesClinical Presentation, Diagnosis, and Initial Evaluation of Diabetes Mellitus in Adults - UpToDatePriscillaNo ratings yet
- Management of Diabetic Foot Ulcers - UpToDateDocument40 pagesManagement of Diabetic Foot Ulcers - UpToDatePriscillaNo ratings yet
- Overview of Treatment of Chronic Wounds - UpToDateDocument35 pagesOverview of Treatment of Chronic Wounds - UpToDatePriscillaNo ratings yet
- Clinical Staging and Management of Pressure-Induced Skin and Soft Tissue Injury - UpToDateDocument31 pagesClinical Staging and Management of Pressure-Induced Skin and Soft Tissue Injury - UpToDatePriscillaNo ratings yet
- Basic Principles of Wound Management - UpToDateDocument44 pagesBasic Principles of Wound Management - UpToDatePriscillaNo ratings yet
- Approach To The Differential Diagnosis of Leg Ulcers - UpToDateDocument44 pagesApproach To The Differential Diagnosis of Leg Ulcers - UpToDatePriscillaNo ratings yet
- Overview of The Treatment of Insomnia in Adults - UpToDateDocument24 pagesOverview of The Treatment of Insomnia in Adults - UpToDatePriscillaNo ratings yet
- Presentation 1Document6 pagesPresentation 1Maya RentinaNo ratings yet
- Endocrine PDFDocument450 pagesEndocrine PDFmariatiNo ratings yet
- VWA - Contemporary Management of Diabetes MellitusDocument46 pagesVWA - Contemporary Management of Diabetes MellitusVincenzina SoósNo ratings yet
- Pediatric Type 1 Diabetes MellitusDocument25 pagesPediatric Type 1 Diabetes MellitusmuhammadferhatNo ratings yet
- Pathophysiology of Type II Diabetes MellitusDocument7 pagesPathophysiology of Type II Diabetes Mellituschinthaka18389021No ratings yet
- Carbohydrate Metabolism - MCQs 4 BDocument10 pagesCarbohydrate Metabolism - MCQs 4 BSaroja Veeresh100% (1)
- SF 81Document2 pagesSF 81Keian EstalaneNo ratings yet
- CHMP Post Authorisation Summary Positive Opinion Mounjaro II 07 - enDocument2 pagesCHMP Post Authorisation Summary Positive Opinion Mounjaro II 07 - enFRUNZANo ratings yet
- A Case Study Submitted in Partial Fulfilment of The Requirements in Capstone ProjectDocument5 pagesA Case Study Submitted in Partial Fulfilment of The Requirements in Capstone Projectedison savellanoNo ratings yet
- Care of Adults 26 Endocrine ManagementDocument26 pagesCare of Adults 26 Endocrine ManagementGaras AnnaBerniceNo ratings yet
- Hospital Discharge Algorithm Based On Admission Hba For The Management of Patients With Type 2 DiabetesDocument6 pagesHospital Discharge Algorithm Based On Admission Hba For The Management of Patients With Type 2 DiabetesxtineNo ratings yet
- 8428 60351 3 PBDocument10 pages8428 60351 3 PBdika dayantiNo ratings yet
- Nama: Malsa Ramadhaniah NPM:222205102Document2 pagesNama: Malsa Ramadhaniah NPM:222205102MalsaNo ratings yet
- Protocol For Intensive Intravenous Insulin Infusion For ICUDocument2 pagesProtocol For Intensive Intravenous Insulin Infusion For ICUburlacuraduuNo ratings yet
- Lecture 6 Carbohydrate MetabolismDocument36 pagesLecture 6 Carbohydrate MetabolismDuduetsang MosalakataneNo ratings yet
- Diabetic Ketoacidosis in ChildrenDocument39 pagesDiabetic Ketoacidosis in ChildrenRichard SiahaanNo ratings yet
- Pcos Biology PaperDocument5 pagesPcos Biology Paperapi-241521552No ratings yet
- DM and Oncology Semi Finals QuizDocument15 pagesDM and Oncology Semi Finals QuizKaren mae alvarroNo ratings yet
- SnehaDocument3 pagesSneharazeena salamNo ratings yet
- Diabetic Awareness Day ProposalDocument6 pagesDiabetic Awareness Day ProposalMaizura NazarudinNo ratings yet
- Thyroid HormonesDocument2 pagesThyroid HormonesLara MieNo ratings yet
- Diabetes20171011 112709Document2 pagesDiabetes20171011 112709ROYNo ratings yet
- NUR 201 Diabetes PowerpointDocument53 pagesNUR 201 Diabetes PowerpointSaad MotawéaNo ratings yet
- Thyroid ReportDocument105 pagesThyroid ReportAARVNo ratings yet
- Mauritius NCD Survey 2015 ReportDocument56 pagesMauritius NCD Survey 2015 Reportsaima.maiharaubNo ratings yet
- T31 - Types of Diabetes and Diagnosis - PTPDocument6 pagesT31 - Types of Diabetes and Diagnosis - PTPangela adelantarNo ratings yet
- Group 8 Sedentary Lifestyle - SampleDocument16 pagesGroup 8 Sedentary Lifestyle - SamplebondbondNo ratings yet
- Sas 34Document3 pagesSas 34Sistine Rose LabajoNo ratings yet
- PexDocument4 pagesPextagastaNo ratings yet