Professional Documents
Culture Documents
Myasthenia Gravis: Immunopathogenesis, Diagnosis, and Management
Myasthenia Gravis: Immunopathogenesis, Diagnosis, and Management
Uploaded by
Allan SalmeronOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Myasthenia Gravis: Immunopathogenesis, Diagnosis, and Management
Myasthenia Gravis: Immunopathogenesis, Diagnosis, and Management
Uploaded by
Allan SalmeronCopyright:
Available Formats
MYASTHENIA GRAVIS:
IMMUNOPATHOGENESIS,
DIAGNOSIS, AND
Downloaded from https://journals.lww.com/continuum by Eqz6vYqm2Eq9JSGSepYNvf+lfLXR/Nj3ZLJUch3/nEjA9tRiU+bkafXjvlTQiazIKr0sV4ZE+iVcNHuR4Nh6Qg3cmmOt8sYiBfgswt0wNh9wkGs32zCfHdDGqaJ2bg+PsZm8Mi1j3lU= on 08/23/2020
MANAGEMENT
Matthew N. Meriggioli
ABSTRACT
Acquired myasthenia gravis (MG) is an autoimmune disorder of neuromuscular
transmission that presents clinically as fluctuating skeletal muscle weakness often
affecting particular muscle groups preferentially. The target of the autoimmune
attack in most cases is the skeletal muscle acetylcholine receptor (AChR), but
in others it may be non-AChR components of the neuromuscular junction, such
as the muscle-specific receptor tyrosine kinase. The final result remains muscle
endplate dysfunction and muscle weakness. The clinical presentation may vary
considerably in MG, both for anti–AChR-positive and anti–AChR-negative disease,
and accurate diagnosis is dependent on clinical recognition of variant as well as
classic disease phenotypes. The primary aim of treatment of MG is induction and
maintenance of clinical or pharmacologic remission while minimizing adverse
effects of therapy. Treatment decisions must be individualized based on MG sever-
ity and coexisting disease, and patient participation in these decisions is essential
to successful management.
Continuum Lifelong Learning Neurol 2009;15(1):35–62.
INTRODUCTION findings that demonstrate this distinc-
Acquired myasthenia gravis (MG) is a tive pattern of weakness and may be
relatively uncommon disease, although confirmed using a number of diagnostic
prevalence rates have increased over tests. Not all patients have this classic
time with recent estimates approaching clinical presentation, however, and var-
20 per 100,000 in the US population iant or atypical presentations must be 35
(Phillips, 2003). An autoimmune attack recognized and appropriately consid-
directed against the neuromuscular ered in the differential diagnosis. Once
junction (NMJ) is the cause of symptoms the diagnosis of MG is made, therapy
in MG. The clinical hallmark is symp- usually begins with cholinesterase in-
tomatic weakness that predominates in hibitors, but most patients will require
certain muscle groups and typically immune-directed therapy. In this chap-
fluctuates in response to effort and rest. ter, the immunopathogenesis of MG is
The diagnosis of MG is primarily based reviewed, and an organized approach to
on the clinical history and examination the diagnosis and treatment of MG is
Relationship Disclosure: Dr Meriggioli has received personal compensation for consulting activities from
Nanodisc, Inc. Dr Meriggioli has received grant support from National Institute of Neurological Disorders and
Stroke (K08NS058800-01) and the Myasthenia Gravis Foundation of America.
Unlabeled Use of Products/Investigational Use Disclosure: Dr Meriggioli discusses the unlabeled use of several
immunosuppressant medications, including mycophenolate mofetil, cyclosporine, tacrolimus, and others.
Copyright # 2009, American Academy of Neurology. All rights reserved.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINTS
presented, including the management at the NMJ. In 80% to 85% of cases,
A Normal
of specific clinical situations. these antibodies are directed against
neuromuscular
transmission is the skeletal muscle nicotinic AChR and
disrupted in IMMUNOPATHOGENESIS are detectable in patient serum. Al-
myasthenia OF MYASTHENIA GRAVIS though antibodies to the AChR are
gravis (MG) by directly responsible for the pathologic
the binding of Pathogenesis of alteration of the muscle endplate result-
autoantibodies Myasthenia Gravis ing in MG, the autoantibody response is
to postsynaptic The autoimmune nature of the disease, T-cell dependent, with CD4+ T cells pro-
proteins involved initially proposed in 1960, is now firmly viding help for B cells to produce anti-
in signaling at the established (Conti-Fine et al, 2006). MG AChR antibodies (Conti-Fine et al, 2006)
neuromuscular satisfies all criteria for an antibody- (Figure 2-1). At least three mechanisms
junction. In 80%
mediated autoimmune disorder: (1) underlie the loss of functional AChRs in
to 85% of cases,
these antibodies
antibodies are present at the site of pa- anti–AChR-positive MG: (1) complement-
are directed thology, the NMJ; (2) immunoglobulin mediated lysis of the muscle endplate
against the from patients with MG causes symp- resulting in distortion and simplification
skeletal muscle toms of MG when injected into experi- of the postsynaptic muscle membrane
acetylcholine mental animals; (3) immunization with (Figure 2-2); (2) accelerated internali-
receptor (AChR). the target antigen (acetylcholine recep- zation and degradation of AChRs caused
tor [AChR]) causes disease in experi- by cross-linkage of AChR by immuno-
A Patients with
mental animals; and (4) removal of cir- globulin (Ig) G; and (3) rarely, blockade
generalized
MG who do not
culating autoantibodies decreases the of the AChR by antibodies attached to
have circulating severity of disease. Specifically, in MG, acetylcholine binding sites.
antibodies to normal neuromuscular transmission is Another postsynaptic neuromuscular
AChR may have disrupted by the binding of autoanti- junction protein, the muscle-specific re-
anti–muscle- bodies to proteins involved in signaling ceptor tyrosine kinase (MuSK) has been
specific receptor
tyrosine kinase
(MuSK)
antibodies.
Current evidence
indicates that
these antibodies
may alter
the normal
36 maintenance
of a high density
of AChRs at the
neuromuscular
junction.
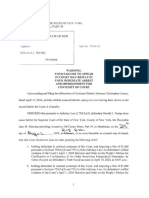
FIGURE 2-1 The immunopathogenesis of myasthenia gravis involves the production
of high-affinity anti–acetylcholine receptor (AChR) antibodies whose
synthesis is modulated by and dependent on AChR-specific T cells that
are activated after presentation of AChR peptides by antigen-presenting cells (APC).
Autoantibodies reduce the numbers of functional AChRs mainly by complement-mediated
lysis of the postsynaptic membrane and by cross-linking of AChRs, causing enhanced
endocytosis and degradation. Direct blockade of the acetylcholine-binding site on the
AChR is a less frequent mechanism.
Abs = antibodies; NMJ = neuromuscular junction.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
A The hyperplastic
thymus glands
of patients with
MG contain all
the functional
components for
the development
of an immune
response to the
AChR, favoring
a role for it in
the initiation and
maintenance of
disease in at least
some patients.
FIGURE 2-2 Electron micrographs of endplate regions from mice with
experimental myasthenia gravis (MG). A, Normal endplate
region. B, Endplate region from myasthenic mouse showing A The endplate
loss of normal endplate morphology due to complement-mediated lysis. Nerve potential (EPP)
terminals are labeled NT; postsynaptic membranes are indicated by the arrows. represents the
summated action
of a large number
of acetylcholine
implicated in many of the 10% to 15% of taneously generate anti-AChR antibod- molecules
patients who are ‘‘seronegative’’ for ies (Le Panse et al, 2008). This suggests released after
anti-AChR antibodies. These patients that the thymus gland may contribute a nerve action
have a distinct generalized form of my- to both the initiation and maintenance potential on
asthenia and harbor circulating anti- of the immune dysregulation directed the postsynaptic
MuSK antibodies (Hoch et al, 2001). against the AChR in at least a subset of AChRs.
The agrin/MuSK signaling pathway likely patients with MG and provides the
A The difference
maintains the normal functional integ- theoretical rationale for thymectomy
between the
rity of the NMJ, and current evidence in nonthymomatous MG. magnitude of
suggests that anti-MuSK antibodies may the EPP and the
alter the normal maintenance of a high Mechanism of Fatigable
current required
density of AChRs at the NMJ, leading to Muscle Weakness for firing of the
reduced numbers of functional AChRs. The summated action of a large num- muscle fiber
ber of acetylcholine molecules released action potential
Role of the Thymus Gland after a nerve action potential on the is quite large in
The thymus gland plays an incompletely postsynaptic receptors produces the normal muscle 37
understood, but likely very important, endplate potential (EPP). If the magni- and is referred
role in the pathogenesis of MG. Most tude of the EPP is greater than or equal to as the safety
factor of
patients with MG have thymic abnor- to the excitation threshold for depolar-
neuromuscular
malities, with greater than 50% of anti– ization of the surrounding sarcolemma,
transmission.
AChR-positive patients having thymic a muscle fiber action potential is pro-
hyperplasia and 10% to 15% having a duced. The difference between the A In MG, the EPP is
thymic tumor (see the chapter ‘‘Para- magnitude of the EPP and the current lessened because
neoplastic Disorders Affecting the Neu- required for threshold firing of the of the loss of
romuscular Junction or Anterior Horn muscle fiber action potential is referred functional AChRs,
resulting in a
Cell’’). The hyperplastic thymus glands to as the safety factor of neuromuscular
reduction in the
of patients with MG contain all the transmission. The action of acetylcho-
safety factor of
functional components for the devel- line on the postsynaptic membrane is neuromuscular
opment of an immune response to the brief and is terminated by the enzyme transmission.
AChR, and thymocytes in culture spon- acetylcholinesterase, which splits the
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINTS
acetylcholine molecule into choline and tained contraction (Figure 2-3A). Fa-
A MG is
acetate. If acetylcholinesterase is in- tigable muscle weakness in MG results
characterized by
fluctuating hibited, a larger and longer EPP results. when the EPP amplitudes are sufficient
fatigable Under normal circumstances, the to generate muscle fiber action poten-
weakness of safety factor of neuromuscular trans- tials at rest or after a single or a few
extraocular, mission is quite large (several times nerve stimulations, but with repeated
oropharyngeal, larger than the threshold potential or sustained muscular effort fall below
axial and/or limb required for generation of a muscle the threshold required for firing of the
muscles, with fiber action potential). With repetitive muscle fiber. Baseline weakness may
normal sensation (2 Hz to 5 Hz) stimulation of the nerve occur when the EPP amplitudes are too
and reflexes. (or sustained stimulation), there is a small to generate muscle fiber action
A Fluctuation of sequential decrease in the store of potentials at rest.
strength is most available acetylcholine molecules and
readily elicited by a resultant decrease in the magnitude CLINICAL EVALUATION
examination of of the EPP, but this has no functional MG is characterized clinically by fluc-
ocular muscle consequence in normal muscle since tuating and fatigable weakness of ex-
function. Most the safety factor of neuromuscular traocular, oropharyngeal, axial, and/or
patients with transmission is so large. limb muscles, with normal sensation
MG have some
In MG, the EPP is lessened because and reflexes. Generalized fatigue, mal-
demonstrable
of the loss of functional AChRs. The aise, exhaustion, and/or pain are not
weakness of
physiologic consequence of this is that symptoms of MG. The approach to
ocular motility or
eyelid closure, the EPP is now significantly closer in eliciting the history and performing the
whether or not magnitude to the threshold depolariza- examination of a patient with possible
there are tion required for firing of the muscle MG is covered in detail in the chapter
symptoms fiber. This reduction in the safety factor ‘‘Approach to the Patient With Sus-
referable to of neuromuscular transmission makes pected Myasthenia Gravis or ALS: A
these muscles. affected endplates more vulnerable as Clinician’s Guide.’’
stores of acetylcholine are depleted Patients with suspected MG should
during repetitive stimulation or sus- be examined so that varying and fa-
tigable weakness in specific muscle
groups may be detected. As demon-
strated in the Case 2-1, most patients
will have some detectable weakness of
eyelid closure and/or extraocular mus-
cle dysmotility when examined care-
38 fully, whether or not these muscle
groups are symptomatically weak. It is
often useful to grade disease distribu-
tion and severity since these factors
have an impact on therapeutic deci-
sions. A useful scale for both research
and general clinical purposes is the
Myasthenia Gravis Foundation of Amer-
A, Endplate potential (EPP) amplitude ica Clinical Classification (Table 2-1)
FIGURE 2-3
is reduced in myasthenia gravis (MG), (Jaretzki et al, 2000).
narrowing the safety factor of
neuromuscular transmission. With repeated stimulations
the EPP amplitude falls below threshold for muscle fiber Atypical Presentations
activation—neuromuscular transmission failure. B, When While classic clinical presentations of MG
a critical number of EPPs fail, a decremental response is
seen on repetitive nerve stimulation studies. as described usually lead to a straight-
forward diagnosis, it is also important to
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Case 2-1
A 35-year-old woman reported trouble swallowing for 6 months. She stated that fruit and
raw vegetables ‘‘seem to get stuck.’’ She had had a similar episode of dysphagia 11 months ago
that resolved after 3 weeks. She also reported nasal speech at the end of the day and intermittent
diplopia while watching television. She had been seen by two neurologists who performed
electrodiagnostic studies that were normal, including repetitive nerve stimulation (RNS) studies
and conventional EMG of multiple muscle groups.
Her neurologic examination was normal with the exception of minimal weakness of eyelid
closure. Although deltoid strength was initially normal, it was 4+/5 after 1 minute of sustained
upper arm lateral extension. Single fiber EMG (SFEMG) of the left extensor digitorum communis
muscle revealed increased jitter without blocking. A trial of pyridostigmine resulted in
improvement in symptoms of dysphagia. Moderate-dose (40 mg a day) daily prednisone was
initiated with complete remission of symptoms. Positive anti-AChR antibodies definitively
confirmed the diagnosis of MG.
Comment. This case illustrates the fact that some patients with MG may have little or no
objective findings of weakness on examination, particularly early in the disease course. The
history of a prior episode of dysphagia, which resolved completely for a period of time, is
characteristic of the early clinical course of many patients with MG. The enhanced sensitivity
of SFEMG allowed for a timely diagnosis and initiation of treatment in this mild case, which was
buttressed by the later finding of elevated titers of anti-AChR antibodies.
recognize more atypical presentations. inent ocular signs or symptoms, partic-
Bulbar weakness with difficulty talking, ularly in older adults. In these cases,
chewing, or swallowing is the initial differentiation from motor neuron
symptom in up to 15% of patients but disease may present a diagnostic chal-
may occasionally occur without prom- lenge (see the chapter ‘‘Approach to
TABLE 2-1 Myasthenia Gravis Foundation of America Clinical
Classification of Myasthenia Gravis
Classification Distribution/Severity of Weakness
Class I Ocular
Class II Mild generalized
Class IIa Predominantly limb/axial muscles 39
Class IIb Predominantly oropharyngeal/respiratory muscles
Class III Moderate generalized
Class IIIa Predominantly limb/axial muscles
Class IIIb Predominantly oropharyngeal/respiratory muscles
Class IV Severe generalized
Class IVa Predominantly limb/axial muscles
Class IVb Predominantly oropharyngeal/respiratory muscles (feeding tube)
Class V Intubation
Modified with permission from Jaretzki A III, Barohn RJ, Ernstoff RM, et al; Task Force of the Medical Scientific
Advisory Board of the Myasthenia Gravis Foundation of America. Neurology 2000;55(1):16–23. Copyright # 2000,
AAN Enterprises, Inc. All rights reserved.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINTS
the Patient With Suspected Myasthenia DIAGNOSTIC PROCEDURES
A Patients with
Gravis or ALS: A Clinician’s Guide’’). The major tools used to confirm the
anti-MuSK
antibodies may Although rare, focal weakness in single clinical diagnosis of a disorder of neuro-
have atypical muscle groups as a presenting feature muscular transmission may be divided
presentations of MG may also occur. ‘‘Dropped head into three main groups: pharmacologic,
characterized by syndrome,’’ caused by severe neck electrophysiologic, and immunologic.
prominent extensor weakness, and initial presen-
oropharyngeal, tations with relatively isolated vocal
facial, neck, and cord or respiratory muscle weakness Pharmacologic Tests
respiratory muscle are rare presentations, but MG should Edrophonium chloride test. By in-
weakness. be considered in the differential diag- hibiting the normal action of acetyl-
A When performing nosis in these patients. If the disease cholinesterase, edrophonium chloride
the edrophonium remains untreated, weakness may become and other acetylcholinesterase inhibi-
(Tensilon) test, fixed and severely involved muscles may tors allow acetylcholine molecules to
only unequivocal become atrophic, giving the appearance diffuse more widely throughout the
improvement in of a chronic myopathy in some patients. synaptic cleft and to interact with
strength of a AChRs sequentially, increasing the am-
sentinel muscle plitude and duration of the EPP. Its
should be Myasthenia Gravis With rapid onset (30 seconds) and short
accepted as a Anti–Muscle-Specific Receptor duration of effect (5 to 10 minutes)
positive result. Tyrosine Kinase Antibodies
Thus, the
make it an ideal agent for this purpose.
response to
Patients with anti-MuSK antibodies may The test consists of administering
edrophonium is have atypical clinical presentations char- edrophonium intravenously and ob-
most reliable in acterized by prominent facial, bulbar, serving for an improvement in muscle
patients with neck, and respiratory muscle involve- strength. The dose of edrophonium
significant ocular ment, sometimes with relative sparing required to produce clinical improve-
or oropharyngeal of ocular muscles (Evoli et al, 2003). ment cannot be predetermined. A
weakness. Clinical presentations similar to anti– number of protocols for administration
AChR-positive generalized MG also oc- have been used, but most commonly a
cur, but purely ocular presentations are test dose of up to 2 mg is given followed
very rare. Respiratory crises are more by subsequent doses of 3 mg to 8 mg
frequent than in those with generalized until there is a positive response or a
anti–AChR-positive disease. While fati- total of 10 mg is given. The patient is
gable muscle weakness may be a observed for 90 seconds in between
prominent symptom, it may be difficult doses and for 3 to 5 minutes after the
40 to demonstrate this fatigability clinically full 10-mg dose is administered.
since weakness in affected muscles may When to use the edrophonium test.
be quite severe at baseline. In many of Despite its widespread use in the clini-
these patients, abnormalities are pref- cal diagnosis of MG, the test can be ob-
erentially demonstrated by clinical and/ jectively and reliably interpreted in only
or electrophysiologic testing of weak a few specific situations. The most im-
muscles, particularly those with weak- portant consideration in performance
ness restricted to facial, neck, or shoul- of the edrophonium test is the end
der muscles. Disease onset in patients point to be used. Only unequivocal im-
with anti-MuSK MG tends to be earlier, provement in strength of a sentinel
generally by the third or fourth decade, muscle should be accepted as a positive
and patients are frequently, but not result. For this reason, resolution of eye-
exclusively, young females. Thymus his- lid ptosis and improvement in strength
tology in these patients is usually nor- of a single paretic extraocular muscle
mal or only mildly abnormal. have been advocated as the only truly
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINT
valid end points because observed func- endplates. Characteristically in MG, a
A Repetitive nerve
tion in these muscles is largely inde- decrementing response of at least 10%
stimulation
pendent of fluctuating effort. Side effects to trains of 2-Hz to 5-Hz stimulation studies are most
from edrophonium include salivation, occurs (Figure 2-3B). This may be sensitive in the
sweating, nausea, stomach cramping, present at baseline or after a period of evaluation of
and muscle fasciculations. Hypotension exercise (postactivation exhaustion). generalized MG
and bradycardia are infrequent and gen- Although a seemingly simple test, and are more
erally resolve with rest in the supine careful attention to proper technique likely to be
position, but atropine (0.4 mg to 2 mg) is important to avoid erroneous RNS abnormal if a
should be available in the event that results. The sensitivity of RNS for clinically weak
bradycardia persists. diagnosing MG ranges from 53% to muscle is tested.
Published reports indicate that the 100% for RNS in generalized MG, and
sensitivity of the edrophonium test in 10% to 17% for ocular MG (Meriggioli
the diagnosis of MG ranges from 71.5% and Sanders, 2005). In generalized MG,
to 95% for generalized MG (Pascuzzi, RNS studies are abnormal in approxi-
2003). The specificity of the test is not mately 60% of patients when a hand
clear, but a positive response to edro- and a shoulder muscle are tested. RNS
phonium has been reported in a variety is more likely to be abnormal in a
of conditions other than MG, including proximal or facial muscle in patients
other disorders of the NMJ, such as with MG and is more likely to be
Lambert-Eaton myasthenic syndrome abnormal in clinically weak muscles.
and botulism, as well as in patients To obtain the maximal diagnostic yield,
with motor neuron disease. Nonres- multiple muscles should be tested,
ponsiveness as well as hypersensitivity particularly clinically weak muscles. If
to cholinesterase inhibitors has been RNS is normal and a high suspicion for
observed in patients with MG who have an NMJ disorder exists, SFEMG of at
anti-MuSK antibodies (Hatanaka et al, least one symptomatic muscle should
2005). be performed (see discussion later in
this chapter).
Single fiber EMG. SFEMG is a se-
Electrophysiologic Tests lective recording technique in which a
Electrophysiologic studies are per- specially constructed concentric nee-
formed in patients with suspected dle is used to identify and record ac-
NMJ disease to confirm a defect in tion potentials from individual muscle
neuromuscular transmission and also fibers. The variation in latency from
to exclude other diseases of the motor nerve activation to muscle action po- 41
unit that may contribute to the clinical tential is the neuromuscular jitter and
presentation. The two principal elec- is produced by fluctuations in the time
trophysiologic tests used to confirm a it takes for the EPP at the NMJ to reach
defect in neuromuscular transmission the threshold for action-potential gen-
are RNS studies and SFEMG. eration. Jitter measurements performed
Repetitive nerve stimulation. RNS during voluntary activation of the mus-
is the most commonly used electro- cle involve the patient minimally con-
physiologic test of neuromuscular tracting the muscle under study while
transmission. At low rates of stimulation the examiner positions the recording
(2 Hz to 5 Hz) RNS serves to stress electrode to record two or more time-
diseased motor endplates by depleting locked potentials (Figure 2-4). Jitter
the store of readily releasable acetyl- is measured as the variation in the
choline, causing failure of neuromus- time interval between the two action
cular transmission in diseased motor potentials in the pair (interpotential
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINT
A Single fiber
EMG is the most
sensitive test
for the diagnosis
of MG but may
be abnormal in
primary nerve
or muscle disease.
The finding of
normal jitter in
a clinically weak
muscle rules out
a defect in
neuromuscular
transmission as
a cause for
weakness in
that muscle.
FIGURE 2-4 A, In single fiber EMG (SFEMG) testing, the recording electrode
is positioned to record from two or more time-locked potentials. Jitter
is measured as the variation in the time interval between the two
action potentials in the pair. B, An example of normal jitter; 40 consecutive discharges
are superimposed. C, Abnormal jitter; 50 consecutive discharges are superimposed.
interval). An increase in the magnitude defect in neuromuscular transmission
of this jitter is the most sensitive as a cause for the weakness. It is im-
electrophysiologic sign of a defect in portant to understand that the en-
neuromuscular transmission. When the hanced sensitivity of SFEMG comes at
defect in neuromuscular transmission is the price of reduced specificity and that
more severe, some nerve impulses fail jitter may be increased in primary nerve
to elicit action potentials, and SFEMG or even muscle disease. Nerve conduc-
recordings demonstrate an intermit- tion studies and conventional EMG
tent absence of one or more single should be done in all cases when
muscle fiber action potentials on con- SFEMG is abnormal to rule out disor-
secutive firings. This is called impulse ders of nerve and muscle that may be
42 blocking and represents neuromuscular associated with defects in neuromuscu-
transmission failure at the involved lar transmission.
endplate. SFEMG is the most sensitive In light of the cost and expertise
clinical test for detection of a defect in required for maintenance of a reusable
neuromuscular transmission, and its single fiber needle electrode, it has been
sensitivity allows for demonstration of suggested that conventional concentric
abnormalities in clinically unaffected needle electrodes may be used to evalu-
muscles. ate neuromuscular jitter. Small studies
The sensitivity of SFEMG for diag- indicate that SFEMG using a concentric
nosing MG ranges from 82% to 99%, needle electrode can demonstrate an
with the highest sensitivity attained abnormality in neuromuscular transmis-
when up to three muscles are tested sion, although with somewhat lower
(Meriggioli and Sanders, 2005). The sensitivity. Normative jitter values for
finding of normal jitter in a clinically voluntarily activated extensor digitorum
weak muscle essentially rules out a communis muscle have recently been
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
published (Kouyoumdjian and Stålberg, moma (see the chapter ‘‘Paraneoplas-
A Elevated titers
2008). tic Disorders Affecting the Neuro-
of anti–AChR-
muscular Junction or Anterior Horn binding
Immunologic Tests Cell’’). antibodies are
Anti-acetylcholine receptor anti- highly specific for
bodies. Antibodies that react with MG but are not
Striated Muscle
AChR proteins are generally regarded found in 10% to
Antibody Assays
as specific serologic markers for ac- 15% of patients.
quired MG. The AChR-binding antibody Antibodies to striated muscle were the
first autoantibody discovered in MG. A Concentrations
assay is the most widely used diagnostic of anti-AChR
test for MG. In general, an elevated They are highly associated with thy-
antibodies vary
concentration of anti–AChR-binding an- moma, being positive in 75% to 80% of
widely among
tibodies in a patient with compatible MG patients with thymoma but are
patients with
clinical features essentially confirms the also positive in nonthymomatous MG, similar degrees
diagnosis of MG, but normal antibody particularly in older patients. Antibod- of weakness and
concentrations do not exclude the di- ies to striated muscle are most useful cannot reliably
agnosis. Anti–AChR-binding antibodies as a marker of thymoma in patients predict severity
are detected in approximately 80% to with MG onset before age 40 (see of disease or
85% of patients with generalized MG, the chapter ‘‘Paraneoplastic Disorders response to
Affecting the Neuromuscular Junction therapy.
but only in 55% of those with purely
ocular symptoms (Keesey, 2004). Se- or Anterior Horn Cell’’). However, A Striational
rum concentrations of AChR-binding striational antibodies may be a valu- antibodies are
antibodies vary widely among patients able marker for MG in middle-aged or correlated with
with similar degrees of weakness and older adult patients with mild disease, the presence of
cannot reliably predict the severity of where they can be the only serologic thymoma but
disease in individual patients. abnormality. may be the
only serologic
Acetylcholine receptor–blocking
abnormality in
antibodies. Blocking antibodies in- Anti–Muscle-Specific Receptor later-onset MG
hibit the binding of radiolabeled - Tyrosine Kinase Antibodies without
bungarotoxin to the AChR by compet- As noted, a proportion of patients with thymoma.
ing for binding to the acetylcholine generalized anti–AChR-antibody-negative
binding site or by allosteric inhibition. A Anti-MuSK
MG have been found to have IgG anti- antibodies are
They represent a minority of the AChR bodies to MuSK, an NMJ protein that found in
antibodies and usually occur in associ- plays an important role in the cluster- approximately
ation with AChR-binding antibodies.
Since less than 1% of patients with MG
ing of AChRs. MuSK antibodies are typi- 40% of anti– 43
cally not found in anti–AChR-antibody- AChR-negative
have only serum-blocking antibodies, positive MG or in ocular MG, although patients with
they add little to diagnostic sensitivity. a few case reports of patients with ocular generalized MG.
Acetylcholine receptor–modulating MG and anti-MuSK antibodies have been
antibodies. Anti-AChR antibodies cross- A A CT scan of the
published. Approximately 40% of pa- chest should be
link the AChR in the membrane and tients with anti–AChR-antibody-negative obtained in all
increase their rate of degradation. The generalized MG have anti-MuSK anti- patients with MG
AChR-modulating antibody test mea- bodies (McConville et al, 2004). to exclude the
sures the rate of loss of labeled AChR presence of a
from human myotubes. A positive thymoma.
result is most useful when the AChR- Other Testing
binding assay is negative, which occurs Chest CT should be performed in all
in about 3% to 4% of patients. High patients with MG to exclude the pres-
levels of AChR-modulating antibodies ence of a thymoma. Chest CT is more
may be seen in association with thy- sensitive than plain chest x-rays for
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
identifying masses in the anterior me- patients with significant ptosis or extra-
diastinum, but MRI does not improve ocular muscle weakness, bedside test-
the diagnostic yield. Because iodinated ing using IV edrophonium is sensitive,
contrast agents may exacerbate myas- but results are subjective. The applica-
thenic weakness, the use of these tion of an ice pack locally to a ptotic
agents is not recommended in the eyelid may also improve myasthenic
routine workup of a patient with MG. ptosis and may be considered an ad-
Because MG often coexists with other junctive diagnostic test, particularly if
autoimmune disorders, particularly thy- the edrophonium test is contraindi-
roid disease, baseline testing of thy- cated or not available. RNS studies are
roid function should be obtained at most likely to yield a positive result if
the time of MG diagnosis, and other clinically weak muscles are tested.
autoimmune serologics should be con- SFEMG is the most sensitive diagnostic
sidered if clinically indicated. test for MG but may be abnormal in
primary nerve or muscle disease. Nor-
Confirming the Diagnosis mal SFEMG in a clinically weak muscle
Once the clinical diagnosis is sus- excludes the diagnosis of MG. The find-
pected, it is important to obtain objec- ing of elevated serum levels of anti–
tive confirmation of the diagnosis using AChR-binding antibodies or anti-MuSK
the tests described above. In general, antibodies in patients with clinical signs
confirmatory immunologic or electro- and symptoms of MG essentially con-
physiologic testing is preferred for a firms the diagnosis. Antibody testing
confident diagnosis. The order in which should be performed on nonimmuno-
the tests are chosen depends on the suppressed patients and should be re-
presenting clinical picture, the sensitiv- peated if initially negative as 15.2% of
ity and specificity of the test for the initially seronegative patients may be-
suspected diagnosis, and the available come positive (Chan et al, 2007).
expertise. A cost-effective approach is
also desirable. Table 2-2 lists the NMJ Differential Diagnosis
tests that should be considered based The differential diagnosis of MG is given
on different clinical presentations. In in Table 2-3. In general, alternative
TABLE 2-2 Diagnostic Tests Based on Distribution of Myasthenic Weakness
44 Distribution Sensitivity Electrodiagnostic Sensitivity Sensitivity
of Weakness Bedside Test (%) Test (Muscle) (%) Immunologic (%)
Ocular (1) Edrophonium 60–95 (1) SFEMG (facial) 90 AChR-Ab 50
(2) Ice packa 89
Oropharyngeal/ None (1) RNS 60 (1) AChR-Ab 85
Generalized (limb/cranial)
(2) SFEMG 99 (2) MuSK-Ab 40–50
(limb/facial) (if above is
negative)
a
Only if ptosis is present.
SFEMG = Single fiber EMG; AChR-Ab = Acetylcholine receptor antibody; RNS = repetitive nerve stimulation; MuSK-Ab =
Muscle-specific receptor tyrosine kinase antibody.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 2-3 Differential Diagnosis of Myasthenia Gravis
Diagnosis Points of Differentiation Comments
Lambert-Eaton Relative sparing of ocular Anti-acetylcholine
myasthenic muscles; hyporeflexia, receptor–binding antibody
syndrome dry mouth absent, anti-voltage-gated
calcium channel antibody
present; low-amplitude
CMAP
Congenital Onset in infancy or Repetitive CMAP (See
myasthenic childhood; no response the chapter ‘‘Congenital
syndromes to immunomodulation Myasthenic Syndromes’’)
Botulism Rapid descending pattern Low-amplitude CMAP
of progression; pupillary,
autonomic involvement
Motor neuron Presence of corticospinal Single fiber EMG
disease or corticobulbar abnormal with
features, muscle cramps/ increased fiber density
fasciculations
Mitochondrial Onset more gradual, no Single fiber EMG may
disorders fluctuation, often no be mildly abnormal
diplopia despite severe
ophthalmoplegia
Acute immune No fluctuation in weakness, Nerve conduction studies,
demyelinating areflexia, acute onset blink reflex, CSF
polyneuropathy
variant syndromes
Thyroid Proptosis MRI demonstration
ophthalmopathy of enlarged extraocular
muscles
CNS disorders Sudden onset, consciousness, MRI brain
causing cranial coordination and sensation
nerve dysfunction affected, ocular weakness
in distribution of single
cranial nerves
45
CMAP = compound muscle action potential.
diagnoses to be considered include aise, apathy, and somnolence rather
other disorders of the NMJ, motor than true fatigable muscle weakness.
neuron disease, primary muscle dis-
eases (particularly those that affect
ocular and pharyngeal muscles), and TREATMENT
CNS lesions affecting the brainstem The outlook for patients with MG has
nuclei. Disorders such as chronic fa- improved considerably in recent years,
tigue syndrome and certain mood largely due to advances in intensive care
disorders may be also be considered, medicine and the use of immunomo-
but symptoms in these cases usually dulating agents. The therapeutic goal is
consist of generalized exhaustion, mal- to return the patient to normal function
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINTS
as rapidly as possible while minimizing
A The treatment of TABLE 2-4 Medications that
the side effects of therapy. The treat- May Exacerbate
MG must be
individualized ment of patients with MG must be Myasthenia Gravis
according to the individualized according to the extent
extent and (ocular versus generalized) and severity " Absolutely Contraindicated
severity of disease (mild to severe) of disease and the Curare and related drugs
and the presence presence or absence of concomitant
D-Penicillamine
of concomitant disease (including but not limited to
illnesses. In most other autoimmune diseases and thy- Botulinum toxin
cases, treatment moma). It is also important to make the Interferon alfa
of MG is a lifelong patient and other treating physicians
process.
aware of medications that may exacer- " Contraindicated—Likely
to Adversely Affect
A Pyridostigmine bate symptoms in MG (Table 2-4). Neuromuscular Transmission
produces some
degree of Symptomatic (Nonimmune) Antibiotics
improvement in Treatment of Myasthenia Gravis Aminoglycosides (gentamicin,
most patients Cholinesterase inhibitors produce kanamycin, neomycin,
with MG, marked streptomycin, tobramycin)
some degree of improvement in most
improvement in a Macrolides (erythromycin,
patients, considerable improvement in
few, and little or azithromycin, telithromycin)
some patients, and little or no improve-
no improvement
ment in others. Pyridostigmine bromide Fluoroquinolones
in others.
(Mestinon) is the most commonly used (ciprofloxacin, levofloxacin,
A Treatment with cholinesterase inhibitor for the man- norfloxacin)
pyridostigmine agement of the symptoms of MG. The Quinine, quinidine,
does not affect initial oral dose in adults is 30 mg to procainamide
disease 60 mg every 4 to 6 hours, which may be Magnesium salts
progression or
adjusted to maximize benefit and min- (IV magnesium replacement)
outcome in MG
imize side effects. Doses exceeding " Caution—May Exacerbate
and will not
prevent a patient
120 mg every 4 hours are rarely effective Weakness in Some Patients
from experiencing and potentially dangerous since these With Myasthenia Gravis
a severe higher doses may overexpose remain- Calcium channel blockers
exacerbation or ing functional AChRs to acetylcholine,
potentially desensitizing them and ex- Beta-blockers
even crisis.
acerbating weakness. Dosing guidelines Lithium
for other cholinesterase inhibitors as
46 well as pediatric dosing guidelines are
Iodinated contrast agents
Statin drugs
given in Table 2-5. Patients will usually
report the onset of a beneficial re-
sponse 30 to 45 minutes after adminis-
tration of pyridostigmine and wearing it. It is important to understand that
off of the benefit approximately 3 to 6 treatment with cholinesterase inhibi-
hours later. Optimal dosing of pyridos- tors does not affect disease progression
tigmine requires individualization, and or outcome and will not prevent a
most patients can learn to self-adjust patient with severe bulbar or respiratory
their dose to maximize benefit. A sus- muscle weakness from experiencing a
tained release form of pyridostigmine worsening of symptoms leading to a
(Mestinon Timespan) is not useful as a severe exacerbation or even crisis.
daytime agent because of its variable Muscarinic side effects are the most
absorption and should be reserved for common adverse reactions of cholines-
nighttime use in patients who require terase inhibitors and include stomach
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINT
TABLE 2-5 Dosing of Anticholinesterase Drugs A The goal of
immune-directed
therapy of MG
Pediatric
is to induce a
Drug Oral Intramuscular Intravenous Oral Dose
remission or near
Pyridostigmine 30 mg to 2.0 mg every 0.7 mg every 1.0 mg/kg to remission of
bromide 60 mg every 4 to 6 hours 4 to 6 hours 7.0 mg/kg symptoms and
(Mestinon) 4 to 6 hours every 4 to then to maintain
6 hours the remission with
the minimal dose
Neostigmine 15 mg 1.5 mg 0.5 mg 0.3 mg/kg to
of medication
(Prostigmin) (bromide) (methylsulfate) (methylsulfate) 2.0 mg/kg in
every 4 to every 4 to every 4 to divided doses required.
6 hours 6 hours 6 hours (3 or 4 times
per day)
Ambenonium 7.5 mg, in - - 0.15 mg/kg up
chloride divided doses to maximum
(3 or 4 times of 1.5 mg/kg/d
per day) in divided
doses
cramps, diarrhea, sweating, bronchial tions in MG: (1) as a short-term interven-
and nasal secretions, bradycardia, nau- tion in patients who have experienced a
sea, and vomiting. When these side sudden worsening of MG, including
effects occur, it is usually an indication myasthenic crisis (see discussion later in
that the dose is too high, and suppress- this chapter); (2) as a treatment prior to
ing these gastrointestinal side effects surgery, often thymectomy, to produce
with agents such as loperamide is rapid improvement in an effort to re-
usually not beneficial. Rarely, patients duce perioperative morbidity; and (3) in
allergic to bromide may develop a skin
rash. These patients may be treated
with ambenonium chloride (Mytelase).
Immune-Directed Therapy
The goal of immune-directed therapy is
to induce remission or near remission 47
of symptoms in as timely a manner as
possible. Maintenance of remission is
then accomplished by slow tapering of
medications over many months until
the minimum dose of medication
required to maintain control of symp-
toms is identified (Figure 2-5). Immune- FIGURE 2-5 Diagrammatic representation of approach
to the immune-directed therapy of
directed therapy of MG may be divided myasthenia gravis.
into short-term (rapid onset) therapies Pred = prednisone; PE/IVIg = plasma exchange/IV
and long-term therapies. immunoglobulin; IDT = immune-directed therapy;
Short-term immune-directed ther- Inc = Increase.
apies. Plasma exchange (plasmaphere- Modified with permission from Richman DP, Agius MA. Treatment of autoimmune
myasthenia gravis. Neurology 2003;61(12):1652–1661. Copyright # 2003,
sis). Plasmapheresis or plasma exchange AAN Enterprises, Inc. All rights reserved.
(PE) is used in three main clinical situa-
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINTS
combination with high-dose daily pred- response when not combined with
A Plasma exchange
nisone as a strategy to prevent steroid- chronic immunosuppression is another
reduces the
circulating levels induced exacerbation. Chronic or serial limitation.
of autoantibodies PE treatments are rarely carried out in IV immunoglobulin. IV immuno-
and induces refractory patients when all other treat- globulin (IVIG) is a widely used treat-
improvement in a ment approaches have failed. ment for exacerbating MG. Support for
matter of days in PE temporarily reduces the levels of its use comes from randomized con-
the majority of circulating antibodies and produces im- trolled trials showing comparable effi-
patients with MG. provement in a matter of days in the cacy in treatment response compared
The benefit from vast majority of patients with acquired with PE (Gajdos et al, 2008) and a re-
a course of MG (Batocchi et al, 2000). A course of cent double-blind placebo-controlled
plasma exchange
PE usually consists of three to six ex- trial in MG patients with worsening
typically wears
changes administered on an every- weakness (Zinman et al, 2007). In the
off after 3 to
4 weeks.
other-day basis. Performing PE on a latter study, Zinman and colleagues
daily basis is not recommended since showed that IVIG induced rapid im-
A The indications this is usually not well tolerated and provement in muscle strength, particu-
for IVIG include may deplete serum clotting factors. larly in patients with moderate to severe
induction of rapid Maximum improvement is most often MG and worsening myasthenic symp-
improvement seen after four to six exchanges in toms. When patients with mild disease
in patients
which 50 mL/kg of plasma is removed at were included in the analysis, the
with a severe
each treatment. Improvement is occa- beneficial effect was modest (although
exacerbation or
crisis, reduction
sionally seen after the first or second statistically significant at 2 weeks) but
of perioperative exchange, particularly in MG patients likely not clinically meaningful. This
morbidity prior to with anti-MuSK antibodies. Decisions study therefore not only provided
surgery, and as regarding the total number of ex- evidence-based support for the use of
chronic therapy in changes depend on clinical response IVIG in MG, but also may have defined
selected patients and tolerability, but more than six the subset of patients in whom it should
with moderate to exchanges may be required in some not be used, namely patients with
severe refractory patients. On the other hand, there is no minor symptoms or with purely ocular
weakness. reason to continue treatments once the weakness.
maximal benefit is attained. The benefit Thus, IVIG should be considered in
from a course of PE typically begins to patients with worsening moderate to
wear off after 3 to 4 weeks, so longer- severe symptoms of MG, particularly if a
lasting immune therapy should be in rapid response to treatment is essential,
place to maintain control of symptoms. ie, evolving oropharyngeal or respiratory
48 Common side effects during PE in- symptoms. The indications for IVIG are
clude paresthesias from citrate-induced also similar to those for PE: inducing
hypocalcemia and symptomatic hypo- rapid improvement in patients with
tension. Although very effective in in- severe disease or crisis, reducing peri-
ducing clinical improvement, the general operative morbidity prior to surgery,
usefulness of PE is limited by its restric- and using as chronic therapy in selected
tion to major medical centers and the refractory patients. Although IVIG has
frequent need for large-bore venous demonstrated similar efficacy to PE in
catheters. Infections and thrombotic the treatment of MG exacerbations, it
complications related to indwelling cath- may be less effective than PE in true MG
eters placed to secure venous access crisis. The initial or ‘‘induction’’ IVIG
occur. PE can reduce coagulation factors, course is usually administered at a dose
particularly with repeated daily treat- of 2 g/kg, which is divided over 2 to 5
ments, leading to bleeding tendencies. days (depending on patient age, renal
The relatively brief duration of clinical function, and ability to tolerate a
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
volume load). Maintenance doses range tic option in anti–AChR-positive adult
A The only absolute
from 0.5 g/kg to 1 g/kg usually on a patients with generalized MG and dis-
indication for
monthly basis. The onset of improve- ease onset before the age of 50. thymectomy is
ment usually occurs within 7 to 10 days Thymectomy in these patients may the presence of
and lasts for 4 to 8 weeks, sometimes enhance the likelihood of spontaneous thymoma; it
longer. Common side effects include improvement or remission. Consider- should be
headaches, chills, and fever, which ation of thymectomy should involve a considered as
usually improve with slowing the rate frank discussion with the patient stating a therapeutic
of infusion. Serious side effects are rare that, while it is probably more likely option for
and include renal toxicity, stroke, and than not that improvement will occur long-term
aseptic meningitis. after the procedure, these potential immunomodulation
in patients
Long-term immune-directed ther- benefits have not been established by
without thymoma
apies. Thymectomy. Based on the pre- rigorous clinical studies, and remission
and with disease
sumed role of the thymus gland in the or improvement may also occur spon- onset prior to
development of MG, therapeutic re- taneously. Most patients tolerate the age 50.
moval of the thymus has been per- procedure quite well if the symptoms
formed in MG for nearly 70 years. An are well controlled prior to the proce- A Prednisone is the
evidence-based practice parameter that dure. The most common concern first choice for
immunosuppressive
analyzed all retrospective, controlled, following surgery is pain, and the use
therapy of MG,
nonrandomized studies of thymectomy of thoracic epidural analgesia maximizes
and its use is
in MG concluded that the benefit postoperative pain control. Pyridostig-
indicated when
associated with thymectomy was gener- mine may be given intramuscularly if generalized or
ally small, and results were confounded the patient is unable to swallow immedi- ocular symptoms
by baseline differences between the sur- ately after thymectomy (see Table 2-5 are not
gical and nonsurgical groups (Gronseth for dosing). adequately
and Barohn, 2000). On this basis, the Corticosteroids. Corticosteroids were controlled by
authors expressed uncertainty as to the first immunosuppressant medi- cholinesterase
whether the observed improvement cations to be widely used in MG and inhibitors.
was the result of thymectomy or could remain the most commonly used
be explained by differences in these immune-directed form of therapy to-
baseline characteristics. An international day. Although randomized controlled
prospective, single-blinded, randomized studies confirming their efficacy in MG
trial of thymectomy (controlling for are lacking, most experts consider cor-
medical therapy) in nonthymomatous ticosteroids a mainstay of therapy and
MG is currently ongoing and will hope- the most effective oral immunosuppres-
fully clarify this issue. sant agent for MG. In a large patient 49
Clinical indications for thymectomy. series, prednisone induced complete
The only absolute indication for thy- remission of symptoms in 28%, marked
mectomy is the presence of a thymoma, improvement (minor symptoms, normal
which is observed in approximately activities of daily living) in 53%, moderate
10% to 20% of patients with MG. Surgi- improvement in 15%, and no improve-
cal removal should be recommended in ment in only 5% (Pascuzzi et al, 1984).
all patients with thymoma, understand- Prednisone has generally been used as
ing that thymectomy is not an emer- the first choice for immunosuppressive
gent or urgent procedure, and should therapy in MG, and its use is indicated
be undertaken only after treatment of when generalized or ocular symptoms of
MG is optimized. Despite the current MG are not adequately controlled by
uncertainty regarding the efficacy of cholinesterase inhibitors alone.
thymectomy in nonthymomatous MG, Prednisone is usually administered at
most experts consider it as a therapeu- high doses for several months during
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINT
the initial treatment of MG, and then it ately one-third to one-half of patients
A The risk of
is gradually tapered off or continued at treated with high-dose daily predni-
steroid-induced
exacerbation may low doses for many years. The clinical sone, with the severity of worsening
be lessened by response is relatively rapid with im- requiring intubation in 8.6% (Pascuzzi
administering provement observed within 2 to 4 et al, 1984). It is therefore advised that
IVIG or plasma weeks when a dose of approximately 1 patients be hospitalized for 5 to 7 days
exchange in mg/kg/d to 1.5 mg/kg/d is used. Once a during initiation of high-dose daily
combination with positive response is achieved, patients prednisone, particularly in the setting
the initiation of may be switched to an alternate-day of significant oropharyngeal or respi-
steroid therapy. regimen of 1.5 mg every other day. ratory symptoms. Alternatively, these
More refractory patients often require patients may receive PE or IVIG prior
daily dosing for 2 to 3 months before to or during steroid initiation in an ef-
initiating a slower alternate-day taper. fort to induce a prompt improvement,
In ocular MG or mild generalized MG, a thereby lessening the risk of steroid-
somewhat lower initial dose of predni- induced exacerbation.
sone (30 mg/d to 40 mg/d) may be as Prednisone is inexpensive, has a
effective in producing marked improve- quick onset of response, and has an
ment or remission. Although it is ac- established track record in MG. Despite
ceptable and recommended by some these advantages, the use of prednisone
experts to start prednisone at very low is limited by the numerous and fre-
doses (10 mg/d) and then build up the quently encountered side effects. The
dose gradually, the onset of improve- common side effects of corticosteroids
ment will be significantly prolonged. are listed in (Table 2-6). Side effects
However, the risk of transient worsen- occur in up to two-thirds of patients.
ing (see below) may be lessened using Although side effects cannot be entirely
this approach. avoided, specific measures may be taken
Transient worsening of weakness has to minimize them. A calorie-restricted,
been reported to occur in approxim- high-protein, low-carbohydrate, low-fat,
TABLE 2-6 Common Corticosteroid Side Effects
Side Effect Prevention
Sodium/fluid retention Sodium-restricted diet
50
Obesity Low-calorie, low-fat diet; exercise
Potassium loss Supplementation as needed
Hypertension Monthly checks, treatment
Impaired glucose tolerance Fasting blood glucose monitored, treated
Osteoporosis Calcium/vitamin D supplementation, bone
density evaluation, bisphosphonates, female
hormone replacement
Cataracts/glaucoma At least yearly ophthalmic evaluation
Steroid myopathy Exercise, high-protein diet
Suppression of growth (children) Minimum effective dose used
Peptic ulcer Treatment if symptoms occur
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINT
low-sodium diet can minimize weight patients with milder disease without
A Azathioprine is an
gain and fluid retention. All patients risk factors for steroid-associated mor-
effective immune-
should be placed on calcium (1200 mg bidity may be started on corticosteroid directed therapy
to 1500 mg a day) and vitamin D (600 monotherapy and then AZA may be for MG, but the
international units to 800 international added, if necessary. onset of benefit
units per day) supplementation to AZA therapy is initiated at 50 mg per may be delayed
minimize bone loss. Bone density day. In the absence of systemic side for as long as 12
should be measured at baseline and effects the dose is then gradually ti- months.
repeated every 6 to 12 months. Post- trated upward by 50 mg per week until
menopausal women and all patients a dose of 2 mg/kg/d to 3 mg/kg/d is
developing osteopenia should also be reached. AZA is usually well tolerated,
treated with bisphosphonates. Hista- but 10% to 15% of patients develop an
mine blockers or proton pump inhib- idiosyncratic reaction characterized by
itors are usually not prescribed routinely fever, nausea, vomiting, and abdominal
but may be used if symptoms of gastric pain or a skin rash, which are reasons to
irritation develop. Monitoring of serum permanently discontinue AZA as these
electrolytes, glucose, weight, and blood symptoms resolve quickly with stopping
pressure should occur on a regular the drug but recur upon rechallenge.
basis. Hepatotoxicity and leukopenia are
Nonsteroidal immune-directed important adverse effects but are re-
therapies. Azathioprine. Azathioprine versible if detected and the dose of
(AZA) (Imuran) is a purine antimetab- AZA is adjusted or discontinued. White
olite that interferes with T-cell and B- blood cell counts and liver enzymes
cell proliferation. It has been used as an should be monitored at least monthly.
immunosuppressant agent in MG since Long-term use of AZA may increase the
1970. risk of developing certain malignancies.
It is used most often as a steroid- This risk is likely dose and duration
sparing agent in patients who remain dependent, so the minimal mainte-
dependent on moderate to high doses nance dose of AZA required to keep
of prednisone, but it is also used in the MG in control should be used.
patients who have an inadequate re- Mycophenolate mofetil. Mycopheno-
sponse to prednisone, and occasionally late mofetil (MMF) selectively blocks
as a stand-alone immunomodulating purine synthesis, thereby suppressing
agent. both T-cell and B-cell proliferation. It
Retrospective studies indicate that has been used increasingly as both a
AZA is effective in 70% to 90% of steroid-sparing agent and a stand-alone 51
patients with MG, but the onset of immune modulator in the treatment of
benefit may be delayed for as long as 12 MG. Clinical efficacy in MG has been
months (Sathasivam, 2008). A double- suggested by a case series and a
blind study comparing oral predniso- retrospective analysis of 85 MG patients
lone with prednisolone plus AZA treated with MMF (Meriggioli et al,
showed that patients receiving AZA 2003) In the latter, 73% of patients were
had fewer relapses and a higher inci- observed to improve using the Myas-
dence of remission and could be thenia Gravis Foundation of America
maintained on a lower prednisolone postintervention classification. Patients
dose, but these beneficial effects were with severe weakness were less likely to
not seen for 18 months (Palace et al, respond, and the onset of benefit was
1998). Patients are frequently pre- observed at a mean of 9 to 11 weeks,
scribed corticosteroids in combination although the initial response was ob-
with AZA on the basis of this study, but served to lag as long as 40 weeks in
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINTS
some patients. Data from two recently steroid-sparing agent (Ciafaloni et al,
A Mycophenolate
completed controlled trials of MMF in 2000). Cyclosporine has been used
mofetil is widely
used as a MG failed to (1) show additional benefit mainly as a steroid-sparing agent in
steroid-sparing of MMF over 20-mg daily prednisone patients in whom AZA is either ineffec-
agent in MG, given as initial immunotherapy, and (2) tive or not tolerated. The recommen-
despite recent show a significant steroid-sparing effect ded initial dose of cyclosporine is 4 mg/
negative of MMF in patients on prednisone. A kg/d to 6 mg/kg/d in two divided doses,
randomized number of factors have been cited to but maintenance dosing of 3 mg/kg/d
clinical trials, explain these negative results, including to 4 mg/kg/d or less is often adequate
largely because the generally mild disease status of the to maintain the effect. The onset of
of its favorable patients, the better-than-expected re- beneficial response may be expected 1
side effect profile
sponse to relatively low-dose daily pred- to 2 months after starting cyclosporine.
and a general
nisone, and the short duration of the Side effects are common and include
agreement of
its clinical
studies (Sanders and Siddiqui, 2008). hirsutism, tremor, gum hyperplasia, and
effectiveness The clinical efficacy of MMF in MG re- anemia, but hypertension and nephro-
among some mains an open question, but it contin- toxicity are the main treatment-limiting
experts. ues to be widely used in the treatment adverse reactions. Over one-quarter
of MG, particularly as a steroid-sparing of patients will develop increases in
A Cyclosporine is
agent, mainly because many experts are serum creatinine between 30% and
mainly used as a
convinced that it is effective and it has 70% of baseline levels (Ciafaloni et al,
steroid-sparing
a favorable side effect profile. 2000). Blood pressure, renal function,
agent in patients
in whom The standard MMF dose is 1000 mg and serum cyclosporine trough levels
azathioprine or twice daily, but doses up to 3000 mg a should be monitored monthly. The
mycophenolate day have been used. Higher doses are risk of certain malignancies (melanoma,
mofetil is either associated with myelosuppression, and lymphoma) may be increased with long-
ineffective or complete blood counts should be term use.
poorly tolerated. monitored at least monthly. In general, Cyclophosphamide. The use of the
side effects are relatively mild, most alkylating agent cyclophosphamide is
A The use of
cyclophosphamide commonly including diarrhea, nausea, reserved for patients with severe gen-
in MG is reserved and abdominal pain. Long-term use eralized MG refractory to conventional
for patients may be associated with an increased therapies. Experience with use of this
with severe risk for certain malignancies, and this agent in MG is very limited. However,
generalized risk is most likely dose and duration in a placebo-controlled double-blind
disease dependent. Further caution results study, monthly IV pulses of cyclophos-
refractory to from recent reports of progressive phamide (500 mg/m2) given to MG
52 all conventional multifocal leukoencephalopathy occur- patients with refractory disease improved
therapies. ring in patients treated with MMF, muscle strength and lowered steroid
although all of these patients were on requirement (De Feo et al, 2002).
multiple nonsteroidal immunosuppres- Remarkable therapy responses have
sant medications. also been reported in three refractory
Cyclosporine. Cyclosporine inhibits patients with MG receiving a one-time
T-cell proliferation via disruption of high-dose (50 mg/kg) IV course of cy-
calcineurin signaling, which blocks the clophosphamide for 4 days followed
synthesis of interleukin (IL)-2 and other by rescue therapy (Drachman et al,
proteins essential to the function of 2003). Benefit persisted for several years
CD4+ T cells. Its efficacy in MG has without relapse. Reported side effects
been suggested by a small, randomized, of cyclophosphamide are common
placebo-controlled clinical trial (Tindall and potentially serious, including mye-
et al, 1993), and larger retrospective losuppression, hemorrhagic cystitis,
studies have supported its use as a and an increased risk of malignancy.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
Obviously, the high rate and severity their disease severity, coexistent ill-
A Tacrolimus may
of toxicity of cyclophosphamide limits nesses, and therapeutic goals. Most
be considered as
its use to only the most refractory patients improve, usually markedly, in a steroid-sparing
patients where the potential benefit response to appropriate treatment. The agent in patients
may outweigh the risks. aim is to achieve complete or near- intolerant or
Newer or evolving immune- complete remission of symptoms. My- unresponsive to
directed treatments. Tacrolimus. A asthenic symptoms should be initially azathioprine,
number of recent reports have indi- managed with a cholinesterase inhibitor mycophenolate
cated that tacrolimus (FK506) may be with dose optimization until it is clear mofetil, and/or
effective in the treatment of MG, that either complete control of symp- cyclosporine.
including a randomized, though un- toms is not possible or the required A Most patients
blinded, study in 36 de novo patients doses are intolerable. The patient with MG
with MG (Nagane et al, 2005). Doses should then be started on high-dose improve, usually
ranging from 3 mg/d to 5 mg/d have (1 mg/kg) daily prednisone. Patients markedly, with
been used in various studies, and a with more than mild weakness affecting appropriate
favorable side effect profile has been oropharyngeal and respiratory muscles immunotherapy.
observed. Tacrolimus belongs to the should be treated with a course of PE or Improvement
same class of immunosuppressant med- IVIG in combination with initiation of induced by
immunotherapy
ications as cyclosporine and has a steroid therapy to mitigate steroid-
rarely persists if all
similar mechanism of action. It appears induced disease worsening. Patients
immunotherapy is
to be less nephrotoxic compared with with mild or purely ocular MG may be discontinued.
cyclosporine, at least at doses used in initially treated with lower daily doses of
published MG reports, but hyperglyce- prednisone (30 mg to 40 mg). Once
mia, because of transcriptional inhibi- remission or significant improvement is
tion of insulin, is a relatively common observed, the prednisone dose is ta-
side effect in transplant patients. Large- pered, aiming for a low-dose alternate-
scale controlled studies of tacrolimus in day (15 mg to 20 mg every other day or
MG are underway in Japan and may less) schedule. Early addition of a
better clarify the role of this agent in steroid-sparing agent (AZA or MMF) is
MG therapy. Until then, it should be considered for patients with moderate
considered in patients who are intoler- or severe disease, particularly those
ant or unresponsive to AZA, MMF, and/ with an incomplete response to high-
or cyclosporine. dose daily prednisone. In patients with
Rituximab. Rituximab is a chimeric milder disease, a steroid-sparing agent
monoclonal antibody directed against may be added after failure of predni-
the B-cell surface marker CD20. It effec- sone tapering. In patients with disease 53
tively reduces circulating B-cell counts onset prior to age 50, thymectomy and
and, based on its potential for elimina- possibly enrollment in the ongoing
tion of autoreactive B-cell clones, may multinational thymectomy trial should
have a therapeutic role in antibody- be considered as a long-term option for
mediated autoimmune diseases, such as immune modulation. If the prednisone
MG. Reported effectiveness of rituximab can eventually be tapered to zero, the
in MG is mainly limited to case reports in dose of the steroid-sparing agent may
patients with refractory MG and in be reduced very slowly to determine
patients who are anti-MuSK antibody the minimum required dose. Improve-
positive (Evoli et al, 2008). ment induced by immunotherapy rarely
persists if all immune-directed treat-
Therapeutic Strategy ments are completely discontinued. As
For all patients, the treatment plan patient response to therapy is variable
chosen must be tailored according to in MG, a hierarchy of treatment choices
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
is necessary in the event that standard necessitate intubation for ventilatory
drugs are either ineffective or not support or airway protection. It is
tolerated (Table 2-7). estimated that one of every five patients
with MG will suffer myasthenic crisis at
some point during their illness (Jani-
Special Therapeutic Situations Ascadi and Lisak, 2007). All patients
Myasthenic crisis. The classic defini- with severe MG exacerbations, produc-
tion of myasthenic crisis is weakness ing prominent oropharyngeal and res-
from MG that is severe enough to piratory muscle symptoms, should be
TABLE 2-7 Treatment of Myasthenia Gravis
Therapeutic
Agent Dosing Comments
First Line Pyridostigmine 30 mg to Symptomatic
90 mg every management only; no
4 to 5 hours effect on disease course
Prednisone 40 mg/d to First line for short-term
80 mg/d immunotherapy
Thymectomy – Option for long-term
immune modulation
Second Line Azathioprine (AZA) 2 mg/kg/d to Steroid-sparing agent
3 mg/kg/d and initial immunotherapy
in selected patients
Mycophenolate 2 g/d to 3 g/d Favorable adverse-effect
mofetil (MMF) profile
IV immunoglobulin 0.75 g/kg to Cost may prohibit serial
(serial treatment) 1.0 g/kg use
Third Line Cyclosporine (CYC) 4 mg/kg/d to Toxicity limits use
5 mg/kg/d in
two divided
doses
54 Tacrolimus (FK506) 2 mg/d to
3 mg/d
Consider when AZA,
MMF, CYC ineffective
or not tolerated
Fourth Line Plasmapheresisa ? 1 to 3 Cost and complications
(serial treatments) exchanges every limit serial use
2 to 4 weeks
Rituximab 1000 mg IV X 2 Promising but minimal
treatments evidence, prohibitive
(separated by cost
2 weeks)
Cyclophosphamide 500 mg/m2 Severe potential toxicity
IV monthly
a
Consider only in moderate to severe patients with significant bulbar and respiratory weakness
refractory to first-line and second-line agents. Used in combination with prednisone for initial (short
term) treatment of moderate to severe myasthenia gravis.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
managed in an intensive care setting alternate-day schedule is typically given.
A Myasthenic crisis
with frequent and close monitoring. As noted, reports suggest a similar ef-
refers to
Indications for intubation generally ficacy of IVIG compared with PE, but weakness from
include evidence of respiratory muscle other reports and personal experience MG involving
fatigue with increasing tachypnea and suggest that it is less effective in MG oropharyngeal
declining tidal volumes, hypoxemia, crisis. Since the effect of PE is short- and respiratory
hypercapnia, and difficulty with secre- term, longer-acting immune-directed muscles that is
tions. In general patients with a forced treatments (usually high-dose daily severe enough to
vital capacity of below 1L and a negative prednisone) should be added to confer necessitate
inspiratory force of 20 cm H2O or less a more prolonged therapeutic effect. intubation for
will require mechanical ventilatory sup- Weaning trials should begin after ventilatory
port. Noninvasive mechanical ventila- support or airway
patients demonstrate a clear trend of
protection.
tion utilizing bilevel positive pressure improved respiratory muscle strength
ventilation may circumvent the need (usually at a vital capacity greater than A Once intubated,
for intubation in selected myasthenic 15 mL/kg). The trial should be termi- all cholinesterase
patients who have not developed hy- nated if the patient exhibits any sign of inhibitors should
percapnia (PCO2 greater than 50 mm respiratory fatigue (tachypnea, tachy- be stopped in
Hg), thereby reducing pulmonary com- cardia, diaphoresis, or agitation). It is patients with MG
plications and lengths of intensive care crisis and a course
important to understand that bedside
of plasma
unit and hospital stay (Seneviratne et al, spirometry testing is not perfect and
exchange should
2008). This approach is likely to be may indicate favorable respiratory
be initiated. Since
most effective in patients with promi- muscle function, but significant oro- the effects of
nent oropharyngeal weakness and less pharyngeal weakness may persist, com- plasma exchange
severe diaphragmatic impairment. promising the upper airway. Often, are short-lived,
A precipitating factor can be iden- improvement in surrogate muscles, longer-acting
tified in most cases of myasthenic cri- such as neck flexors, will be observed immunosuppressive
sis and most commonly include one to improve in correlation with respira- medications
or more of the following: broncho- tory and bulbar muscle strength and aid should be started
pulmonary infections, aspiration, surgi- in the clinical assessment. (or optimized)
cal procedures including thymectomy, Ocular myasthenia gravis. Ocular to confer a
long-lasting
corticosteroid-induced worsening, rapid MG is the designation given to patients
therapeutic
tapering of immune modulators, and who have signs and symptoms solely in
effect.
exposure to drugs that may increase the ocular muscles (eyelid elevators
myasthenic weakness. Excessive dosing and extraocular muscles). Ptosis and/
of cholinesterase inhibitors can poten- or diplopia are the initial symptoms of
tially increase weakness due to depo- MG in up to 85% of patients (Grob et al, 55
larization blockade. In addition to 2008), and almost all patients have both
weakness, signs of cholinergic hyperac- symptoms within 2 years of disease
tivity will be present, such as excessive onset. If weakness remains limited to
salivation, increased bronchial secre- the ocular muscles (17% of patients)
tions, muscle fasciculations, and ab- after 2 years, there is a 90% likelihood
dominal cramping. It is recommended that the disease will not generalize. If
practice to discontinue the use of ocular symptoms are adequately con-
cholinesterase inhibitors following in- trolled with cholinesterase inhibitors,
tubation to reduce these symptoms, as these patients may be reassured that
they may complicate the management immunosuppressive medications and
of airway secretions. Because of its thymectomy may be avoided. Confir-
rapid onset of action, PE is the fa- mation of the clinical diagnosis of
vored treatment for myasthenic crisis. A ocular MG may be a challenge as RNS
course of four to six exchanges on an studies and anti-AChR antibodies are
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
KEY POINT
often negative, and, as noted, interpre- in all patients who do not achieve
A Treatment of
tation of the edrophonium test may be complete control of symptoms with
ocular MG
requires an difficult. In many cases the diagnosis is cholinesterase inhibitors. Obviously,
accurate made on the basis of SFEMG testing. Up the decision to initiate steroid therapy
assessment of to 50% of patients with ocular MG may will depend on the risk-benefit assess-
the patient’s have anti-AChR antibodies, and a similar ment, which is significantly different if
functional percentage have abnormal SFEMG in a steroids are being considered in pa-
impairment and limb muscle, but these findings do not tients for purely cosmetic reasons ver-
its effects on predict generalization. sus patients in whom diplopia has a
daily life. Treatment of ocular MG requires an profound bearing on their livelihood
accurate assessment of the patient’s (pilots, surgeons, etc). There is some
functional impairment and its effects evidence to suggest that prednisone
on daily life. While cholinesterase inhib- treatment may delay or reduce the fre-
itors may control symptoms adequately quency of progression of ocular MG to
in some patients, the benefit is often generalized disease (Kupersmith et al,
partial and not long-lived, and predni- 2003). As illustrated in Case 2-2, the
sone is often quite effective. Treatment visual symptoms of ocular MG may
with prednisone should be considered respond poorly to anticholinesterase
Case 2-2
A 52-year-old man reported diplopia and left ptosis for the past 18 months.
A diagnosis of MG was made on the basis of a positive edrophonium test.
He was initially treated with pyridostigmine by his ophthalmologist with
initial resolution of symptoms, but subsequently he experienced return and
then worsening of ocular symptoms. The dose of pyridostigmine was
increased to 120 mg every 3 to 4 hours, which only slightly improved his
symptoms but caused severe diarrhea, which he treated with loperamide.
On examination he had bilateral medial rectus weakness and left
greater than right ptosis that was fatigable with sustained upgaze. Facial,
oropharyngeal, and extremity strength were normal.
Anti-AChR antibodies were negative, but the diagnosis of MG was
confirmed with SFEMG, which showed abnormal jitter in the left extensor
digitorum communis muscle. He was started on 40 mg of prednisone and
noted a complete remission of symptoms 10 days later. Prednisone was
gradually tapered and maintained at 7.5 mg every other day with no
56 symptom recurrence. He gained 2.3 kg after beginning prednisone but had
no other side effects.
Comment. Patients with ocular MG who have an incomplete response to
cholinesterase inhibitors and/or worsening of symptoms (even if remaining
limited to the ocular muscles) should, in most instances, be started on
immunomodulatory (prednisone) treatment. This decision will obviously
depend on the severity of the real and perceived disability caused by the
ocular symptoms and must be individualized. At some point, the physician
has to decide whether to treat the disease definitively rather than simply
manage the symptoms. In ocular MG, a gratifying response can be achieved
with low or moderate doses of prednisone, and the treatment benefit is
often maintained with doses of corticosteroids that do not significantly
suppress the immune system and cause few major systemic adverse effects.
Thus, although prolonged treatment is usually required, the long-term risk
associated with such treatment can be minimized.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
agents and nonpharmacologic therapy, patient series. Thymectomy is of ques-
A Patients with
while corticosteroids are usually effec- tionable value in anti–MuSK-positive
anti-AChR-
tive. Prednisone may be started at an patients because their thymi lack the negative MG
initial dose of 20 mg/d with gradual hyperplastic changes seen in patients are clinically
increases every 3 to 5 days until a clinical with anti-AChR antibodies. Recent stud- heterogeneous
response is achieved. In ocular MG, the ies indicate that the actual frequency of and include
treatment benefit is often maintained double seronegativity (undetectable patients with
with doses of corticosteroids that do AChR or MuSK antibodies) may be as ocular, mild
not significantly suppress the immune low as 5% (Chan et al, 2007). generalized,
system and cause few major systemic Childhood myasthenia gravis. and severe
adverse effects. A steroid-sparing agent The occurrence of autoimmune MG generalized MG.
may be considered if this is not the case. prior to age 18 is well established. A Children with MG
Thymectomy is generally not consid- Diagnostic confirmation of the clinical are more likely to
ered in purely ocular MG. suspicion of autoimmune MG is com- be seronegative,
Seronegative myasthenia gravis. plicated by the fact that up to 50% of making the
Until recently, the term seronegative patients with childhood MG may be distinction
MG referred to patients who have a antibody negative. The highest pro- between
myasthenic illness but do not have portion of anti-AChR seronegativity oc- autoimmune MG
and a congenital
antibodies to the AChR. These patients curs among the youngest (prepubertal)
myasthenic
are clinically heterogeneous and may patients, and it is precisely these
syndrome more
include patients with ocular, mild patients in whom the distinction from difficult, particular
generalized, or severe generalized MG. a congenital myasthenic syndrome (see in younger
At least for mild or purely ocular cases, the chapter ‘‘Congenital Myasthenic patients.
the explanation for seronegativity may Syndrome’’) is most relevant. Electro-
be that titers of anti-AChR antibodies diagnostic studies may identify a defect A The options for
management of
are simply below the limits of detection in neuromuscular transmission but
childhood MG are
of currently available assays. Similar to cannot always distinguish between an
not significantly
patients who are anti-AChR positive, se- autoimmune and congenital cause. In different from
ronegative patients have been reported particularly difficult cases, a beneficial those for the
to improve with corticosteroids, immu- response to PE or IVIG may help to es- adult disease,
nosuppressive treatments, plasmaphe- tablish a diagnosis of autoimmune MG. although the
resis, and even thymectomy. The options for management of precautions and
Approximately 40% of patients with childhood MG are not significantly ramifications
anti–AChR-negative MG harbor anti- different from those for the adult may be more
MuSK antibodies. These patients often disease, although the precautions and significant.
have prominent axial, bulbar, and ramifications may be more significant. Spontaneous 57
respiratory muscle weakness and may Spontaneous remissions are relatively remissions
are relatively
be refractory to some conventional common, particularly in prepubertal
common,
treatments (Case 2-3). A poor response patients, and this must be kept in mind
particularly in
to anticholinesterase agents has been when considering treatment, particu- prepubertal
reported in up to 70% of patients. larly long-term therapies. Pyridostig- patients, and
Effective therapies reported in clinical mine may be initiated at a dose of 0.5 this must be
series of patients with anti-MuSK MG mg/kg to 1.0 mg/kg every 4 to 6 hours. kept in mind
include PE, prednisone, cyclosporine, The liquid form is dispensed at 60 mg/ when considering
MMF, and rituximab (Evoli et al, 2008). 5 mL and may be useful, particularly in treatment,
A dramatic response to PE (sometimes younger children. For patients who particularly
after one or two exchanges) and a rela- remain symptomatic despite optimal long-term
tively poor response to AZA and IVIG dosing of cholinesterase inhibitors, therapies.
have been reported, but these observa- prednisone may be used and is effi-
tions need to be confirmed in larger cacious and cost-effective. As noted,
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
Case 2-3
A 26-year-old woman initially presented with a 3-month history of
severe dysphagia, nasal speech, and neck weakness with head drop.
An edrophonium test was performed and resulted in worsening of
dysarthria and transient dyspnea.
Electrodiagnostic studies showed normal nerve conduction studies
and no significant decrement on RNS of the ulnar and spinal accessory
nerves. SFEMG of the extensor digitorum communis was reportedly
normal. Conventional EMG showed no spontaneous activity but revealed
short-duration motor unit action potentials with mildly increased
complexity and an early recruitment pattern consistent with myopathy.
Anti-AChR antibodies were negative. She was empirically placed on
moderate-dose daily prednisone.
Two weeks later, she was hospitalized with a severe exacerbation
of bulbar weakness and new reports of exertional shortness of breath.
She received a course of IVIG but deteriorated and was intubated.
Anti-AChR antibodies were repeated and reportedly were ‘‘borderline
positive.’’ After repeated IVIG treatments and the initiation of high-dose
daily prednisone and AZA, her condition improved only mildly but
stabilized.
She was referred for a second opinion, at which time she reported
frequent exacerbations of bulbar and respiratory weakness despite
treatment with steroids, AZA, cyclosporine, and serial IVIG. Examination
showed severe facial and moderately severe oropharyngeal weakness,
neck extension greater than neck flexion weakness, and mild (5-/5)
proximal limb weakness. She had mild bilateral ptosis without significant
fatigability and no significant extraocular muscle weakness. SFEMG of
the orbicularis oculi showed increased jitter with blocking. Conventional
EMG was consistent with myopathy without spontaneous activity. The
patient underwent a course of plasmapheresis, which resulted in a marked
clinical improvement after the second exchange. The prednisone dose
was optimized (1 mg/kg/d), and MMF was added at a dose of 2.5 g/d.
Anti-MuSK antibody testing was positive. After 11 months, the patient
had minimal disease manifestations on prednisone (30 mg every other day)
and MMF.
Comment. This case illustrates a number of important points
58 regarding anti–MuSK-positive MG. First, patients may present atypically
with severe bulbar, respiratory, and axial muscle weakness, sometimes
with relative sparing of ocular muscles as in this patient. The diagnosis
of MG may be difficult since electrophysiologic abnormalities may
be limited to facial, bulbar, and axial muscles, so that RNS and even
SFEMG studies in limb muscles are often completely normal despite
the severe clinical phenotype. ‘‘Myopathic’’ changes on electrodiagnostic
studies have also been reported in these patients and further complicate
the diagnostic picture. A lack of response or even worsening in
response to cholinesterase inhibitors may be observed as well. Most
patients with anti–MuSK-positive MG eventually respond to aggressive
immunomodulation, and corticosteroids and MMF are among the
agents that have been noted to be effective. A dramatic response to
PE, as observed in this patient, is also a reported clinical feature of
anti–MuSK-positive MG.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
however, the chronic side effects of Fetal and transient neonatal my-
A Corticosteroids,
prednisone are numerous and signifi- asthenia gravis. Approximately 10%
plasma exchange,
cant and potentially have a long-term to 20% of infants born to mothers with and IVIG have
impact in children (growth stunting, MG develop transient neonatal MG, been used safely
weight gain, mood alteration, hypergly- which may occur in both anti–AChR- in pregnancy and
cemia, hypertension, etc). A suggested positive and anti–AChR-negative moth- are the agents
starting dose is 0.5 mg/kg/d, with a ers. Symptoms of transient neonatal of choice for
maximum starting dose in older chil- MG usually develop a few hours after treatment of MG
dren of 30 mg/d. Steroid-sparing immu- birth and, as the name suggests, are in a pregnant
nosuppressive drugs should be used in self-limited, resolving within 1 month. woman.
more severe or refractory cases in a Treatment is supportive, including ven- A Transient
manner similar to that described in tilator support and nasogastric feed- neonatal MG
adult MG. PE and IVIG are effective ings, if needed. Pyridostigmine (0.5 mg/ usually develops
short-term therapies in childhood MG. kg to 1.0 mg/kg) in divided doses a few hours after
Thymectomy has been performed with administered 30 minutes prior to feed- birth in infants
reported favorable results in childhood ing may be useful. born to mothers
MG, even in patients less than 5 years of Muscle weakness due to transplacen- with MG.
age, but the effects on the immune tal passage of maternal pathogenic Pyridostigmine
may be useful
system of removing the thymus at this autoantibodies may also manifest in
to manage
early age is not clear. With regard to its utero, producing arthrogryposis, re-
symptoms, which
effectiveness, the high rates of sponta- duced fetal movements, polyhydram- usually resolve
neous remission in childhood MG nios, and stillbirth. This risk may be within 1 month.
make this assessment difficult. Thy- increased when maternal antibodies are
moma is very rare in juvenile MG. directed against the fetal AChR. Since
Myasthenia gravis in pregnancy. mothers may be asymptomatic, the
Pregnancy may affect the course of MG diagnosis may be difficult. It is not
in an unpredictable way. Generally known whether treatment of the mother
speaking, worsening of symptoms most with PE-reducing maternal antibody
frequently occurs in the first trimester, concentrations can reduce the risk of
or in the first 3 to 4 weeks postpartum. transient neonatal or fetal myasthenia.
Corticosteroids, PE, and IVIG have been
used safely during pregnancy and are PROGNOSIS AND
the agents of choice for treatment of LONG-TERM OUTLOOK
MG exacerbation in a pregnant woman. Early in the course of MG, symptoms
The overuse of cholinesterase inhibi- may fluctuate and remissions lasting
tors should be avoided as they may months or longer are not uncommon, 59
induce uterine contractions. In general, although rarely permanent. Maximum
immunosuppressant medications have disease severity is reached within 2
potential teratogenic effects, and their years of disease onset in two-thirds of
use should preferably be discontinued patients (Grob et al, 2008). In most
4 to 6 months prior to conceiving. The patients, the active stage of disease,
decision to discontinue these agents characterized by relapses and remis-
once a woman is already pregnant will sion, may last 7 to 8 years. This is
involve careful assessment of the tera- followed by a relatively inactive stage
togenic risks versus the risk of MG lasting approximately 10 years and a
exacerbation. Regional anesthesia is final stage of ‘‘burned out’’ disease (Juel
preferred for delivery or cesarean and Massey, 2007). It is important to
section. Magnesium sulfate should not recognize that during the ‘‘inactive’’
be used to manage preeclampsia be- stage, disease exacerbations may still be
cause of its adverse effects on the NMJ. precipitated by intercurrent illness,
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
exposure to drugs that adversely affect tensive care and immunotherapy have
neuromuscular transmission, or preg- contributed to a very favorable progno-
nancy. The amount of fixed weakness sis for MG in most patients. Although
experienced in the ultimate stage of once a severe and often fatal illness,
disease may be dependent on the ef- MG can now be treated effectively in
fectiveness of immunotherapy during most patients with minimal long-term
the active stage. Recent advances in in- morbidity.
REFERENCES
Batocchi AP, Evoli A, Dischino C, et al. Therapeutic apheresis in myasthenia gravis.
Ther Apher 2000;4(4):275–279.
Chan KH, Lachance DH, Harper CM, Lennon VA. Frequency of seronegativity in
adult-acquired generalized myasthenia gravis. Muscle Nerve 2007;36(5):651–658.
Ciafaloni E, Nikhar NK, Massey JM, Sanders DB. Retrospective analysis of the use of
cyclosporine in myasthenia gravis. Neurology 2000;55(3):448–450.
Conti-Fine BM, Milani M, Kaminski HJ. Myasthenia gravis: past, present and future.
J Clin Invest 2006;116(11):2843–2854.
De Feo LG, Schottlender J, Martelli NA, Molfino NA. Use of intravenous pulsed
cyclophosphamide in severe, generalized myasthenia gravis. Muscle Nerve
2002;26(1):31–36.
Drachman DB, Jones RJ, Brodsky RA. Treatment of refractory myasthenia: ‘‘rebooting’’
with high-dose cyclophosphamide. Ann Neurol 2003;53(1):29–34.
Evoli A, Bianchi MR, Riso R, et al. Response to therapy in myasthenia gravis with
anti-MuSK antibodies. Ann NY Acad Sci 2008;1132:76–83.
Evoli A, Tonali PA, Padua L, et al. Clinical correlates with anti-MuSK antibodies in
generalized seronegative myasthenia gravis. Brain 2003;126(pt 10):2304–2311.
60
Gajdos P, Chevret S, Toyka K. Intravenous immunoglobulin for myasthenia gravis.
Cochrane Database Syst Rev 2008;(1):CD002277.
Grob D, Brunner N, Namba T, Pagala M. Lifetime course of myasthenia gravis.
Muscle Nerve 2008;37(2):141–149.
Gronseth GS, Barohn RJ. Practice parameter: thymectomy for autoimmune
myasthenia gravis (an evidence-based review): report of the Quality Standards
Subcommittee of the American Academy of Neurology. Neurology 2000;55(1):
7–15.
Hatanaka Y, Hemmi S, Morgan MB, et al. Nonresponsiveness to anticholinesterase
agents in patients with MuSK-positive MG. Neurology 2005;65(9):1508–1509.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Hoch W, McConville J, Helms S, et al. Auto-antibodies to the receptor tyrosine
kinase MuSK in patients with myasthenia gravis without acetylcholine receptor
antibodies. Nature Medicine 2001;7(3):365–368.
Jani-Ascadi A, Lisak RP. Myasthenic crisis: guidelines for prevention and treatment.
J Neurol Sci 2007;261(1–2):127–133.
Jaretski A 3rd, Barohn RJ, Ernstoff RM, et al. Myasthenia gravis: recommendations
for clinical research standards. Task force of the Medical Scientific Advisory
Board of the Myasthenia Gravis Foundation of America. Neurology 2000;55(1):
16–23.
Juel VC, Massey JM. Myasthenia gravis. Orphanet J Rare Dis 2007;2:44.
Keesey JC. Clinical evaluation and management of myasthenia gravis. Muscle
Nerve 2004;29(4):484–505.
Kouyoumdjian JA, Stålberg EV. Reference jitter values for concentric needle
electrodes in voluntarily activated extensor digitorum communis muscle and
orbicularis oculi muscles. Muscle Nerve 2008;376):694–699.
Kupersmith MJ, Latknay R, Homel P. Development of generalized disease at 2 years
in patients with ocular myasthenia gravis. Arch Neurol 2003;60(2):243–248.
Le Panse R, Cizeron-Clairac G, Cuvelier M, et al. Regulatory and pathogenic mechanisms
in human autoimmune myasthenia gravis. Ann NY Acad Sci 2008;1132:135–142.
McConville J, Farrugia ME, Beeson D, et al. Detection and characterization of
MuSK antibodies in seronegative myasthenia gravis. Ann Neurol 2004;55(4):
580–584.
Meriggioli MN, Ciafaloni E, Al-Hayk KA, et al. Mycophenolate mofetil in the
treatment of myasthenia gravis: an analysis of efficacy, safety and tolerability.
Neurology 2003;61(10):1438–1440.
Meriggioli MN, Sanders DB. Advances in the diagnosis of neuromuscular disorders.
Am J Phys Med Rehabil 2005;84(8):627–638.
Nagane Y, Utsugisawa K, Obara D, et al. Efficacy of low-dose FK-506 in the
treatment of myasthenia gravis—a randomized pilot study. Eur Neurol 2005;53(3):
146–150.
61
Palace J, Newsom-Davis J, Lecky B. A randomized double-blind trial of prednisone
alone or with azathioprine in myasthenia gravis. Myasthenia Gravis Study Group.
Neurology 1998;50(6):1778–1783.
Pascuzzi RM. The edrophonium test. Semin Neurol 2003;23(1):83–88.
Pascuzzi RM, Coslett HB, Johns TR. Long-term corticosteroid treatment of
myasthenia gravis: report of 116 patients. Ann Neurol 1984;15(3):291–298.
Phillips LH 2nd. The epidemiology of myasthenia gravis. Ann N Y Acad Sci 2003;
998:407–412.
Richman DP, Agius MA. Treatment of autoimmune myasthenia gravis. Neurology
2003;61(12):1652–1661.
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
" MYASTHENIA GRAVIS
Sanders DB, Siddiqui ZA. Lessons from two trials of mycophenolate mofetil in
myasthenia gravis. Ann N Y Acad Sci 2008;1132:249–253.
Sathasivam S. Steroids and immunosuppressant drugs in myasthenia gravis. Nature
Clin Pract Neurol 2008;4(6):317–327.
Seneviratne J, Mandrekar J, Wijdicks EF, Rabinstein AA. Noninvasive ventilation
in myasthenic crisis. Arch Neurol 2008;65(1):54–58.
Tindall RS, Phillips JT, Rollins JA, et al. A clinical therapeutic trial of cyclosporine
in myasthenia gravis. Ann N Y Acad Sci 1993;681:539–551.
Zinman L, Ng E, Bril V. IV immunoglobulin in patients with myasthenia gravis:
a randomized controlled trial. Neurology 2007;68(11):837–841.
62
Continuum Lifelong Learning Neurol 2009;15(1)
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- Day 1 - Well Bore PositioningV2Document64 pagesDay 1 - Well Bore PositioningV2wwwNo ratings yet
- Miastenia GravisDocument28 pagesMiastenia Gravismariateresajijon7No ratings yet
- PBL - NervousDocument2 pagesPBL - Nervousgie sarcedaNo ratings yet
- NEJMra 1602678Document12 pagesNEJMra 1602678Olga Manco GuzmánNo ratings yet
- Neuromuscular Junction DisorderDocument10 pagesNeuromuscular Junction DisorderZosmita Shane GalgaoNo ratings yet
- Myasthenia Gravis: Murali Thavasothy DCH MRCP FRCA Nicholas Hirsch FRCADocument3 pagesMyasthenia Gravis: Murali Thavasothy DCH MRCP FRCA Nicholas Hirsch FRCAMirela CiobanescuNo ratings yet
- Rle (NCM 116) CasesDocument12 pagesRle (NCM 116) CasesLaurence ZernaNo ratings yet
- Myasthenia Gravis Presentation and Treatment Variations: A Case Study ApproachDocument5 pagesMyasthenia Gravis Presentation and Treatment Variations: A Case Study ApproachLiyasariNo ratings yet
- MG-New and Emerging Treatments (Bmjmed-2023)Document6 pagesMG-New and Emerging Treatments (Bmjmed-2023)Apostolos T.No ratings yet
- Review: Myasthenic CrisisDocument11 pagesReview: Myasthenic CrisisRaisha TriasariNo ratings yet
- Bja MGDocument6 pagesBja MGVignesh VenkatesanNo ratings yet
- Myasthenia Gravis and Lambert-Eaton Myasthenic Syndrome - Continuum December 2016Document28 pagesMyasthenia Gravis and Lambert-Eaton Myasthenic Syndrome - Continuum December 2016Habib G. Moutran BarrosoNo ratings yet
- CrossDocument10 pagesCrossvalentinaro73No ratings yet
- The Pharmacologic Treatement of Muscle PainDocument32 pagesThe Pharmacologic Treatement of Muscle PainLissaBrNo ratings yet
- Acute Compartment Syndrome in Lower Extremity.3Document9 pagesAcute Compartment Syndrome in Lower Extremity.3marsss.medNo ratings yet
- A Symptoms and Signs Approach To The Patient With.4Document16 pagesA Symptoms and Signs Approach To The Patient With.4pondebernardoNo ratings yet
- Jvim 34 1707Document11 pagesJvim 34 1707Juan DuasoNo ratings yet
- Medicine Case SeriesDocument4 pagesMedicine Case SeriesSwapnil BelsareNo ratings yet
- Maddison 2006Document10 pagesMaddison 2006Mayara MoraisNo ratings yet
- Intravenous Sub-Anesthetic Ketamine For Perioperative AnalgesiaDocument8 pagesIntravenous Sub-Anesthetic Ketamine For Perioperative AnalgesiaAraNo ratings yet
- Myotonic Muscle Disorders and Periodic Paralysis SyndromesDocument20 pagesMyotonic Muscle Disorders and Periodic Paralysis SyndromesIzabella MihályNo ratings yet
- Myasthenia Gravis: A Review: Hideyuki Matsumoto, MD, PHD and Yoshikazu Ugawa, MD, PHDDocument7 pagesMyasthenia Gravis: A Review: Hideyuki Matsumoto, MD, PHD and Yoshikazu Ugawa, MD, PHDZainal AbidinNo ratings yet
- Myasthenia GravisDocument2 pagesMyasthenia GravisAlly JuanezaNo ratings yet
- Intravenous Sub-Anesthetic Ketamine For Perioperative AnalgesiaDocument8 pagesIntravenous Sub-Anesthetic Ketamine For Perioperative AnalgesiaTommy ArisandyNo ratings yet
- Corticospinal SBG BiomarkerDocument8 pagesCorticospinal SBG Biomarkeraria tristayanthiNo ratings yet
- Management of Acute Ischemic Stroke Specific Focus.21Document11 pagesManagement of Acute Ischemic Stroke Specific Focus.21Marina SolansNo ratings yet
- Relação Estrutura AtividadeDocument25 pagesRelação Estrutura AtividadeFábioNo ratings yet
- The Effectiveness of Neural Mobilization For Neuromusculoskeletal Conditions: A Systematic Review and Meta-AnalysisDocument29 pagesThe Effectiveness of Neural Mobilization For Neuromusculoskeletal Conditions: A Systematic Review and Meta-AnalysisAnonymous GzRz4H50FNo ratings yet
- 4.effects of Electrical and Electromagnetic Stimulation After Anteriro Cruciate Ligament ReconstructionDocument8 pages4.effects of Electrical and Electromagnetic Stimulation After Anteriro Cruciate Ligament Reconstructionf.mariajdbNo ratings yet
- MuSK Muscle Specific Kinase Positive Myasthenia .12 PDFDocument6 pagesMuSK Muscle Specific Kinase Positive Myasthenia .12 PDFjuan calrosNo ratings yet
- Myasthenia GravisDocument25 pagesMyasthenia GravisIka Wulan PermataNo ratings yet
- Tema NeurodinámicaDocument30 pagesTema NeurodinámicaisetisNo ratings yet
- Congenital Myasthenic Syndromes Recent Advances.6Document7 pagesCongenital Myasthenic Syndromes Recent Advances.6Elif Tugce AydinNo ratings yet
- Myasthenia Gravis - A Review of Current TherapeutiDocument7 pagesMyasthenia Gravis - A Review of Current TherapeutiZainal AbidinNo ratings yet
- Skeletal Muscle Relaxant (Lecture Notes QIUP 2017)Document9 pagesSkeletal Muscle Relaxant (Lecture Notes QIUP 2017)Monissha ThiaguNo ratings yet
- Autoimmune Neurological Diseases: Ni Made SusilawathiDocument30 pagesAutoimmune Neurological Diseases: Ni Made SusilawathiAprilliexxNo ratings yet
- JPM 2017 0344Document3 pagesJPM 2017 0344Abbey WaltzNo ratings yet
- JCM 11 01597Document23 pagesJCM 11 01597rafael rocha novaesNo ratings yet
- Myesthenia Gravis MedscapeDocument8 pagesMyesthenia Gravis MedscapeSarah OvinithaNo ratings yet
- The Effectiveness of Neural Mobilization For Neuromusculoskeletal Conditions: A Systematic Review and Meta-AnalysisDocument29 pagesThe Effectiveness of Neural Mobilization For Neuromusculoskeletal Conditions: A Systematic Review and Meta-AnalysisRegarNo ratings yet
- Protocol For The Impact of CBT For Insomnia On Pain Symptoms and Central Sensitisation in Fibromyalgia A Randomised Controlled TrialDocument14 pagesProtocol For The Impact of CBT For Insomnia On Pain Symptoms and Central Sensitisation in Fibromyalgia A Randomised Controlled TrialMário Márcio da Matta LopesNo ratings yet
- Imágenes de RM de Trauma MuscularDocument23 pagesImágenes de RM de Trauma Muscularmicamart.94No ratings yet
- 2019 Role of The Extracellular Matrix in Muscle InjuriesDocument3 pages2019 Role of The Extracellular Matrix in Muscle InjuriesPhysio AcademyNo ratings yet
- Myasthenia Gravis (Primer)Document20 pagesMyasthenia Gravis (Primer)Phoebe CoolerNo ratings yet
- Spinal Segmental Sensitization As A Common OriginDocument8 pagesSpinal Segmental Sensitization As A Common OriginRossangel Huapaya RomeroNo ratings yet
- Greene, S. A. Chronic Pain Pathophysiology and Treatment Implications. Topics in Companion Animal Medicine, v.25, n.1, p.5-9. 2010 PDFDocument5 pagesGreene, S. A. Chronic Pain Pathophysiology and Treatment Implications. Topics in Companion Animal Medicine, v.25, n.1, p.5-9. 2010 PDFFran WermannNo ratings yet
- 51.differential Diagnosis of Myasthenia Gravis - A ReviewDocument11 pages51.differential Diagnosis of Myasthenia Gravis - A ReviewSeptime TyasNo ratings yet
- Tong2018 Durere Si SimturiDocument8 pagesTong2018 Durere Si SimturiMunteanu AlexandruNo ratings yet
- RJN 2017 2 Art-04Document3 pagesRJN 2017 2 Art-04Ana GabrielaNo ratings yet
- Motor Cortex and Deep Brain Stimulation For The Treatment of Intractable Neuropathic Face PainDocument7 pagesMotor Cortex and Deep Brain Stimulation For The Treatment of Intractable Neuropathic Face PainT.U. Pai João da Caridade & Caboclo FlechasNo ratings yet
- Myasthenia Gravis: Newer Therapies Offer Sustained ImprovementDocument11 pagesMyasthenia Gravis: Newer Therapies Offer Sustained ImprovementSiti NofriansyahNo ratings yet
- Effects of Electrical Stimulation in Spastic Muscles After StrokeDocument25 pagesEffects of Electrical Stimulation in Spastic Muscles After StrokeRenzo Flores CuadraNo ratings yet
- PDF 20230724 005934 0000Document4 pagesPDF 20230724 005934 0000Bos AseNo ratings yet
- Muscle Relaxants and Antispasticity AgenDocument13 pagesMuscle Relaxants and Antispasticity AgenDarasimiNo ratings yet
- Ashkenazi 2007Document10 pagesAshkenazi 2007Ecaterina PozdircăNo ratings yet
- Facial Nerve Trauma Clinical Evaluation And.41Document15 pagesFacial Nerve Trauma Clinical Evaluation And.41Razaria DailyneNo ratings yet
- Clinphar MidtermDocument51 pagesClinphar MidtermGolden MaknaeNo ratings yet
- 2 Myasthenia Gravis and MS 2Document50 pages2 Myasthenia Gravis and MS 2Rawbeena RamtelNo ratings yet
- Repetitive Transcranial Magnetic Stimulation and Pain Management: Systemic Narrative ReviewDocument19 pagesRepetitive Transcranial Magnetic Stimulation and Pain Management: Systemic Narrative ReviewJoão Francisco AbrantesNo ratings yet
- Muscle and Nerve - 2023 - Claytor - Myasthenic Crisis BESTDocument12 pagesMuscle and Nerve - 2023 - Claytor - Myasthenic Crisis BESTAdreanNo ratings yet
- Case Studies of Lower Respiratory Tract InfectionsDocument25 pagesCase Studies of Lower Respiratory Tract InfectionsMarianNo ratings yet
- The Giver by Lois Lowry - ExcerptDocument15 pagesThe Giver by Lois Lowry - ExcerptHoughton Mifflin Harcourt100% (1)
- Lesson 1 Principles and TheoriesDocument11 pagesLesson 1 Principles and TheoriesJoycee BoNo ratings yet
- Pure Potency EnergyDocument6 pagesPure Potency EnergyLongicuspis100% (3)
- Resignation LetterDocument1 pageResignation LetterJerel John CalanaoNo ratings yet
- Eating Disorder PPT by Shreyasi MittalDocument35 pagesEating Disorder PPT by Shreyasi MittalPrachi gattaniNo ratings yet
- Step 7 Err Code125936644Document37 pagesStep 7 Err Code125936644mohammadNo ratings yet
- Eco Map 3Document1 pageEco Map 3Ferent Diana-roxanaNo ratings yet
- SysDocument6 pagesSysRaja ReeganNo ratings yet
- 16SEE - Schedule of PapersDocument36 pages16SEE - Schedule of PapersPiyush Jain0% (1)
- (Lesson2) Cultural, Social, and Political Institutions: Kinship, Marriage, and The HouseholdDocument5 pages(Lesson2) Cultural, Social, and Political Institutions: Kinship, Marriage, and The HouseholdPlat JusticeNo ratings yet
- Disturbed Sleep PatternDocument2 pagesDisturbed Sleep Patternmaria_magno_6100% (1)
- Day 1 NotesDocument4 pagesDay 1 NotesPawan KumarNo ratings yet
- Vocabulary + Grammar Unit 3 Test ADocument3 pagesVocabulary + Grammar Unit 3 Test AJoana FernandesNo ratings yet
- Case Study RubricDocument2 pagesCase Study RubricShainaNo ratings yet
- After Eating Lunch at The Cheesecake FactoryDocument3 pagesAfter Eating Lunch at The Cheesecake FactoryRahisya MentariNo ratings yet
- Use of Realism in Mulk Raj Anand's Novels: Karan SharmaDocument2 pagesUse of Realism in Mulk Raj Anand's Novels: Karan SharmasirajahmedsNo ratings yet
- Web Mining PPT 4121Document18 pagesWeb Mining PPT 4121Rishav SahayNo ratings yet
- C1 - U5 - Grammar - Revision (1) - CONDITIONALSDocument2 pagesC1 - U5 - Grammar - Revision (1) - CONDITIONALSAdriana Merlos CasadoNo ratings yet
- IntrotovedicmathDocument3 pagesIntrotovedicmathmathandmultimediaNo ratings yet
- Final Project ThermalDocument21 pagesFinal Project ThermalArizap MoltresNo ratings yet
- Judge Merchan Order To Show Cause New York Truth PostsDocument2 pagesJudge Merchan Order To Show Cause New York Truth PostsRobert GouveiaNo ratings yet
- LLLT in Skin - PINAR Avci PDFDocument12 pagesLLLT in Skin - PINAR Avci PDFBrunoNo ratings yet
- Practice Test Cao Hoc 2012Document9 pagesPractice Test Cao Hoc 2012SeaBlueNo ratings yet
- W.B. Yeats A Critical Study: BY Reid, Forrest, 1875-1947Document71 pagesW.B. Yeats A Critical Study: BY Reid, Forrest, 1875-1947safdarNo ratings yet
- Managing Human Resources 7th Edition Gomez-Mejia Solutions Manual DownloadDocument12 pagesManaging Human Resources 7th Edition Gomez-Mejia Solutions Manual DownloadVera Roth100% (26)
- Research Article: Minimum Weight Design of Sinusoidal Corrugated Web Beam Using Real-Coded Genetic AlgorithmsDocument14 pagesResearch Article: Minimum Weight Design of Sinusoidal Corrugated Web Beam Using Real-Coded Genetic AlgorithmsTamir EnkhNo ratings yet
- Sustainable Project ManagementDocument4 pagesSustainable Project ManagementafirulNo ratings yet
- The Passion of Jesus Christ: BY Saint Alphonsus de LiguoriDocument67 pagesThe Passion of Jesus Christ: BY Saint Alphonsus de Liguorisatya0988No ratings yet