
Health Declaration Form
Health Declaration Form
You might also like
- 2pac's BiographyDocument40 pages2pac's BiographyDelia Tanase100% (1)
- Lottery Scam EmailDocument6 pagesLottery Scam EmailMushtaq M.Chinoy90% (41)
- USPAP (Uniform Standards of Professional Appraisal Practice, The Appraisal Foundation) PDFDocument370 pagesUSPAP (Uniform Standards of Professional Appraisal Practice, The Appraisal Foundation) PDFMichael Smith0% (1)
- Health and Travel History Declaration Form PDFDocument1 pageHealth and Travel History Declaration Form PDFMeriel Ocbian100% (1)
- Evidence LawDocument467 pagesEvidence LawWylson Logisticals89% (35)
- Health and Travel History Declaration FormDocument1 pageHealth and Travel History Declaration Formvenus kay faderogNo ratings yet
- Health and Travel History Declaration Form: Please Check OneDocument1 pageHealth and Travel History Declaration Form: Please Check Onepaolo ledesmaNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJo Anth Bernabe BuenaventuraNo ratings yet
- Visitors Health Checklist Form (From DTI and DOLE)Document1 pageVisitors Health Checklist Form (From DTI and DOLE)melbaNo ratings yet
- Health ChecklistDocument14 pagesHealth ChecklistClark Kent BatucanNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlexander IgasanNo ratings yet
- Health Checklist PDFDocument2 pagesHealth Checklist PDFMarkNo ratings yet
- Crew Health Self-Declaration and Daily Temperature Record - Global - Onsigner Version OCT2020Document2 pagesCrew Health Self-Declaration and Daily Temperature Record - Global - Onsigner Version OCT2020Knowrain ParasNo ratings yet
- Health & Safety Check Declaration Form: TemperatureDocument1 pageHealth & Safety Check Declaration Form: TemperatureChy GomezNo ratings yet
- RFDGCDC Health and Safety Declaration FormDocument1 pageRFDGCDC Health and Safety Declaration FormChy GomezNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNaldrin RosalesNo ratings yet
- Health and Travel History Declaration Form: Please Check OneDocument1 pageHealth and Travel History Declaration Form: Please Check OneJC Valerio DelacruzNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Visitor Health Declaration FormDocument1 pageVisitor Health Declaration FormJo Anth Bernabe BuenaventuraNo ratings yet
- Phoa Health Declaration Form - TVHDocument1 pagePhoa Health Declaration Form - TVHCriszel Joy Atillano AseloNo ratings yet
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - ASharme Cagalawan AmahanNo ratings yet
- Health ChecklistDocument1 pageHealth ChecklistU N K O W N U N k o w nNo ratings yet
- Health Checklist: Masakitlumunok)Document4 pagesHealth Checklist: Masakitlumunok)Jaylou M. LigarayNo ratings yet
- Philippine Red Cross Registration Form: Camarines Sur Chapter Safety ServicesDocument2 pagesPhilippine Red Cross Registration Form: Camarines Sur Chapter Safety ServicesKyle VargasNo ratings yet
- Declaration FormDocument1 pageDeclaration FormJzelNo ratings yet
- Health Checklist Health ChecklistDocument2 pagesHealth Checklist Health ChecklistMaria Rhoda C. FontanillaNo ratings yet
- Visitors Health Check List: TemperatureDocument1 pageVisitors Health Check List: TemperatureSterben ShouchiNo ratings yet
- Health Checklist: NG:) Lumunok)Document2 pagesHealth Checklist: NG:) Lumunok)Rose Duron GumaNo ratings yet
- Barangay Employee Health Declaration FormDocument2 pagesBarangay Employee Health Declaration FormBarangay CentroNo ratings yet
- Self Declaration Form MeluhaDocument1 pageSelf Declaration Form MeluhaSandy BergerNo ratings yet
- Revised Health Declaration FormDocument1 pageRevised Health Declaration FormMei SasucaNo ratings yet
- ISO Health ChecklistDocument1 pageISO Health ChecklistRonnel SaludezNo ratings yet
- Health Checklist Employees 1 Converted 1Document2 pagesHealth Checklist Employees 1 Converted 1the7thAliceNo ratings yet
- Temperature:: Signature Over Printed NameDocument2 pagesTemperature:: Signature Over Printed NameBarangay CentroNo ratings yet
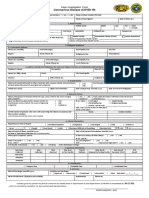
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- Health Questionnaire On Covid-19: Email AddressDocument2 pagesHealth Questionnaire On Covid-19: Email AddressMichael PlumaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAzri AzizNo ratings yet
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityDocument2 pagesHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormRONARD JUSTINE GRANADANo ratings yet
- Health Declaration Form Health Declaration Form: Respondent Information Respondent InformationDocument2 pagesHealth Declaration Form Health Declaration Form: Respondent Information Respondent InformationErnilyn Espinosa LiganNo ratings yet
- Health Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail TechDocument1 pageHealth Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail Techcindya jorduelaNo ratings yet
- Client/ Visitor Contact Tracing Form Client/ Visitor Contact Tracing FormDocument1 pageClient/ Visitor Contact Tracing Form Client/ Visitor Contact Tracing FormArrianne Aivoree FloraNo ratings yet
- Employee - Visitor Screening QuestionnaireDocument1 pageEmployee - Visitor Screening QuestionnaireDyne SabijonNo ratings yet
- Activity 6: Identification and Appropriate Management of Communicable DiseasesDocument2 pagesActivity 6: Identification and Appropriate Management of Communicable DiseasesA J FathimaNo ratings yet
- En-Covid-19 Health Declaration Form Ver 2Document1 pageEn-Covid-19 Health Declaration Form Ver 2Babar ArtsNo ratings yet
- Health DeclarationDocument1 pageHealth DeclarationMai ChannelNo ratings yet
- Bangsamoro Transition Authority: Reminders For Physical AttendeesDocument2 pagesBangsamoro Transition Authority: Reminders For Physical AttendeesShob SinsuatNo ratings yet
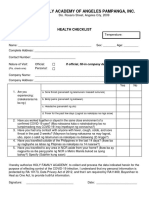
- Holy Family Academy of Angeles Pampanga, Inc.: Health ChecklistDocument1 pageHoly Family Academy of Angeles Pampanga, Inc.: Health ChecklistKarlNo ratings yet
- Form#1 - HDF - Consent Form For RT-PCRDocument1 pageForm#1 - HDF - Consent Form For RT-PCRdddzbdcmrkNo ratings yet
- In The Past1 4 Da S, Did You Have Any of Thefollowing:: SheetDocument1 pageIn The Past1 4 Da S, Did You Have Any of Thefollowing:: SheetLeoni FrancNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormRandy OpadiaNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageMiamor NatividadNo ratings yet
- Health Form For Civil Service ExamDocument1 pageHealth Form For Civil Service Examralph sabaNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageJoezerk CarpioNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PagemarieleNo ratings yet
- Health Declaration: YES NODocument1 pageHealth Declaration: YES NOEliezal Dean B. CardeñoNo ratings yet
- HDF PDFDocument1 pageHDF PDFJhon Rey GonsalezNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageFedelyn SemenianoNo ratings yet
- 2 - HEALTH DECLARATION FORM For New Hire 05292020 KTDocument1 page2 - HEALTH DECLARATION FORM For New Hire 05292020 KTpam01pamNo ratings yet
- Conquering COVID-19 with CHRIST: A Husband and His WifeaEUR(tm)s Account of a Physical Fight Versus a Spiritual Fight While Battling COVID-19From EverandConquering COVID-19 with CHRIST: A Husband and His WifeaEUR(tm)s Account of a Physical Fight Versus a Spiritual Fight While Battling COVID-19No ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Output No. 1Document2 pagesOutput No. 1Zyreane FernandezNo ratings yet
- Output No. 3Document1 pageOutput No. 3Zyreane FernandezNo ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Output No. 2Document2 pagesOutput No. 2Zyreane FernandezNo ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Graduate Studies Final Examination in Research and StatisticsDocument4 pagesGraduate Studies Final Examination in Research and StatisticsZyreane FernandezNo ratings yet
- Fourth Quarter Nationwide Simultaneous Earthquake Drill 2021Document5 pagesFourth Quarter Nationwide Simultaneous Earthquake Drill 2021Zyreane FernandezNo ratings yet
- Oral Communication in Context 1Document7 pagesOral Communication in Context 1Zyreane FernandezNo ratings yet
- Guisguis National High School: Department of Education Region III Schools Division of Zambales Sta. Cruz DistrictDocument2 pagesGuisguis National High School: Department of Education Region III Schools Division of Zambales Sta. Cruz DistrictZyreane FernandezNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesZyreane FernandezNo ratings yet
- GRADES 1-12 Daily Lesson LOG School Grade Level Teacher Learning Area Teaching Dates and Time QuarterDocument2 pagesGRADES 1-12 Daily Lesson LOG School Grade Level Teacher Learning Area Teaching Dates and Time QuarterZyreane FernandezNo ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Curriculum and Instruction Checklist: Indicator Level of PracticeDocument5 pagesCurriculum and Instruction Checklist: Indicator Level of PracticeZyreane FernandezNo ratings yet
- Summary All Individual Development PlanDocument12 pagesSummary All Individual Development PlanZyreane FernandezNo ratings yet
- Table of Specification: Summative TestDocument2 pagesTable of Specification: Summative TestZyreane FernandezNo ratings yet
- Class Program: GRADE 11 - TVL-HE - CookeryDocument1 pageClass Program: GRADE 11 - TVL-HE - CookeryZyreane FernandezNo ratings yet
- English 8: Department of EducationDocument3 pagesEnglish 8: Department of EducationZyreane FernandezNo ratings yet
- Sa GNHS G10 1Document2 pagesSa GNHS G10 1Zyreane FernandezNo ratings yet
- Weekly Home Learning Plan: Guisguis National High SchoolDocument2 pagesWeekly Home Learning Plan: Guisguis National High SchoolZyreane FernandezNo ratings yet
- O o o o O: Pls. Check On The Item Below That May Descried To Your StrategiesDocument1 pageO o o o O: Pls. Check On The Item Below That May Descried To Your StrategiesZyreane FernandezNo ratings yet
- WHLP Individual Earth and Life Oral Com PR2 Nov. 11 15 Week 5 With ActivitiesDocument4 pagesWHLP Individual Earth and Life Oral Com PR2 Nov. 11 15 Week 5 With ActivitiesZyreane FernandezNo ratings yet
- Summative Examination Cookery SY 2020-2021 I. Multiple Choice. Select The Best AnswerDocument2 pagesSummative Examination Cookery SY 2020-2021 I. Multiple Choice. Select The Best AnswerZyreane FernandezNo ratings yet
- RJSC Schedule XDocument3 pagesRJSC Schedule XNafisur Rahman100% (1)
- AutoInvoiceExecution - Auto Invoice Execution ReportDocument7 pagesAutoInvoiceExecution - Auto Invoice Execution ReportTommy AgustioNo ratings yet
- Every Nation Language Institute (Enli) and Ralph Martin Ligon, V. Maria Minelliedela CruzDocument2 pagesEvery Nation Language Institute (Enli) and Ralph Martin Ligon, V. Maria Minelliedela CruzMark Anthony ReyesNo ratings yet
- Offering SlipDocument6 pagesOffering SlipTanao TaoNo ratings yet
- Turkish Economy (1980-1989)Document15 pagesTurkish Economy (1980-1989)ademNo ratings yet
- Hisa PresentationDocument12 pagesHisa Presentationapi-631631105No ratings yet
- Jaiib 10 Weeks Study Plan Nov 2020Document11 pagesJaiib 10 Weeks Study Plan Nov 2020Siva BantuNo ratings yet
- David Hume My Own LifeDocument8 pagesDavid Hume My Own Lifeoolong9No ratings yet
- First Division: Charben Duarte Y Oliveros, Petitioner, vs. People of The Philippines, Respondent. DecisionDocument6 pagesFirst Division: Charben Duarte Y Oliveros, Petitioner, vs. People of The Philippines, Respondent. DecisionMarian Dominique AuroraNo ratings yet
- Legal Regulation of Cyber Crimes in IndiaDocument9 pagesLegal Regulation of Cyber Crimes in IndiaSwarnaprava DashNo ratings yet
- Introducing Tort Law in BangladeshDocument10 pagesIntroducing Tort Law in BangladeshArs Khan100% (2)
- Income ExemptDocument25 pagesIncome Exemptapi-3832224No ratings yet
- Pindi Yulinar Rosita - 008201905023 - Session 5Document7 pagesPindi Yulinar Rosita - 008201905023 - Session 5Pindi YulinarNo ratings yet
- Bernard of Clairvaux LettersDocument4 pagesBernard of Clairvaux Lettersoliver.johnson578No ratings yet
- StoppardDocument6 pagesStoppardCharlie FuentesNo ratings yet
- Iowa Supreme Court Ruling in Paternity Fraud CaseDocument27 pagesIowa Supreme Court Ruling in Paternity Fraud CaseGazetteonlineNo ratings yet
- Stuvia 1968904 lcp4807 Exam Pack Questions and Answers For 2018 2022 Download FileDocument42 pagesStuvia 1968904 lcp4807 Exam Pack Questions and Answers For 2018 2022 Download FilebchiceleganceNo ratings yet
- AZURE ACCESS AND SecurityDocument20 pagesAZURE ACCESS AND Securityamit kaishverNo ratings yet
- Leaf Obd Readthedocs Io en LatestDocument29 pagesLeaf Obd Readthedocs Io en LatestodipasNo ratings yet
- Rosh and CompanyDocument2 pagesRosh and CompanyAli KhanNo ratings yet
- Partnership ACTDocument73 pagesPartnership ACTTushar SharmaNo ratings yet
- CmmaDocument8 pagesCmmamg504100% (1)
- 201 Scra 210Document4 pages201 Scra 210Camille Grande100% (1)
- 1 XXX Vs People G.R. No. 252087Document13 pages1 XXX Vs People G.R. No. 252087ahmadjibrail dianangNo ratings yet
- MyApplication Unisa Forms M30Document1 pageMyApplication Unisa Forms M30MbaliNo ratings yet
- Speed, Time, and Distance Worksheet: Name: - DateDocument2 pagesSpeed, Time, and Distance Worksheet: Name: - Datehendrik koesumaNo ratings yet









































































































Download as docx, pdf, or txt
You might also like
- 2pac's BiographyDocument40 pages2pac's BiographyDelia Tanase100% (1)
- Lottery Scam EmailDocument6 pagesLottery Scam EmailMushtaq M.Chinoy90% (41)
- USPAP (Uniform Standards of Professional Appraisal Practice, The Appraisal Foundation) PDFDocument370 pagesUSPAP (Uniform Standards of Professional Appraisal Practice, The Appraisal Foundation) PDFMichael Smith0% (1)
- Health and Travel History Declaration Form PDFDocument1 pageHealth and Travel History Declaration Form PDFMeriel Ocbian100% (1)
- Evidence LawDocument467 pagesEvidence LawWylson Logisticals89% (35)
- Health and Travel History Declaration FormDocument1 pageHealth and Travel History Declaration Formvenus kay faderogNo ratings yet
- Health and Travel History Declaration Form: Please Check OneDocument1 pageHealth and Travel History Declaration Form: Please Check Onepaolo ledesmaNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJo Anth Bernabe BuenaventuraNo ratings yet
- Visitors Health Checklist Form (From DTI and DOLE)Document1 pageVisitors Health Checklist Form (From DTI and DOLE)melbaNo ratings yet
- Health ChecklistDocument14 pagesHealth ChecklistClark Kent BatucanNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlexander IgasanNo ratings yet
- Health Checklist PDFDocument2 pagesHealth Checklist PDFMarkNo ratings yet
- Crew Health Self-Declaration and Daily Temperature Record - Global - Onsigner Version OCT2020Document2 pagesCrew Health Self-Declaration and Daily Temperature Record - Global - Onsigner Version OCT2020Knowrain ParasNo ratings yet
- Health & Safety Check Declaration Form: TemperatureDocument1 pageHealth & Safety Check Declaration Form: TemperatureChy GomezNo ratings yet
- RFDGCDC Health and Safety Declaration FormDocument1 pageRFDGCDC Health and Safety Declaration FormChy GomezNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNaldrin RosalesNo ratings yet
- Health and Travel History Declaration Form: Please Check OneDocument1 pageHealth and Travel History Declaration Form: Please Check OneJC Valerio DelacruzNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Visitor Health Declaration FormDocument1 pageVisitor Health Declaration FormJo Anth Bernabe BuenaventuraNo ratings yet
- Phoa Health Declaration Form - TVHDocument1 pagePhoa Health Declaration Form - TVHCriszel Joy Atillano AseloNo ratings yet
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - ASharme Cagalawan AmahanNo ratings yet
- Health ChecklistDocument1 pageHealth ChecklistU N K O W N U N k o w nNo ratings yet
- Health Checklist: Masakitlumunok)Document4 pagesHealth Checklist: Masakitlumunok)Jaylou M. LigarayNo ratings yet
- Philippine Red Cross Registration Form: Camarines Sur Chapter Safety ServicesDocument2 pagesPhilippine Red Cross Registration Form: Camarines Sur Chapter Safety ServicesKyle VargasNo ratings yet
- Declaration FormDocument1 pageDeclaration FormJzelNo ratings yet
- Health Checklist Health ChecklistDocument2 pagesHealth Checklist Health ChecklistMaria Rhoda C. FontanillaNo ratings yet
- Visitors Health Check List: TemperatureDocument1 pageVisitors Health Check List: TemperatureSterben ShouchiNo ratings yet
- Health Checklist: NG:) Lumunok)Document2 pagesHealth Checklist: NG:) Lumunok)Rose Duron GumaNo ratings yet
- Barangay Employee Health Declaration FormDocument2 pagesBarangay Employee Health Declaration FormBarangay CentroNo ratings yet
- Self Declaration Form MeluhaDocument1 pageSelf Declaration Form MeluhaSandy BergerNo ratings yet
- Revised Health Declaration FormDocument1 pageRevised Health Declaration FormMei SasucaNo ratings yet
- ISO Health ChecklistDocument1 pageISO Health ChecklistRonnel SaludezNo ratings yet
- Health Checklist Employees 1 Converted 1Document2 pagesHealth Checklist Employees 1 Converted 1the7thAliceNo ratings yet
- Temperature:: Signature Over Printed NameDocument2 pagesTemperature:: Signature Over Printed NameBarangay CentroNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- Health Questionnaire On Covid-19: Email AddressDocument2 pagesHealth Questionnaire On Covid-19: Email AddressMichael PlumaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAzri AzizNo ratings yet
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityDocument2 pagesHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormRONARD JUSTINE GRANADANo ratings yet
- Health Declaration Form Health Declaration Form: Respondent Information Respondent InformationDocument2 pagesHealth Declaration Form Health Declaration Form: Respondent Information Respondent InformationErnilyn Espinosa LiganNo ratings yet
- Health Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail TechDocument1 pageHealth Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail Techcindya jorduelaNo ratings yet
- Client/ Visitor Contact Tracing Form Client/ Visitor Contact Tracing FormDocument1 pageClient/ Visitor Contact Tracing Form Client/ Visitor Contact Tracing FormArrianne Aivoree FloraNo ratings yet
- Employee - Visitor Screening QuestionnaireDocument1 pageEmployee - Visitor Screening QuestionnaireDyne SabijonNo ratings yet
- Activity 6: Identification and Appropriate Management of Communicable DiseasesDocument2 pagesActivity 6: Identification and Appropriate Management of Communicable DiseasesA J FathimaNo ratings yet
- En-Covid-19 Health Declaration Form Ver 2Document1 pageEn-Covid-19 Health Declaration Form Ver 2Babar ArtsNo ratings yet
- Health DeclarationDocument1 pageHealth DeclarationMai ChannelNo ratings yet
- Bangsamoro Transition Authority: Reminders For Physical AttendeesDocument2 pagesBangsamoro Transition Authority: Reminders For Physical AttendeesShob SinsuatNo ratings yet
- Holy Family Academy of Angeles Pampanga, Inc.: Health ChecklistDocument1 pageHoly Family Academy of Angeles Pampanga, Inc.: Health ChecklistKarlNo ratings yet
- Form#1 - HDF - Consent Form For RT-PCRDocument1 pageForm#1 - HDF - Consent Form For RT-PCRdddzbdcmrkNo ratings yet
- In The Past1 4 Da S, Did You Have Any of Thefollowing:: SheetDocument1 pageIn The Past1 4 Da S, Did You Have Any of Thefollowing:: SheetLeoni FrancNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormRandy OpadiaNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageMiamor NatividadNo ratings yet
- Health Form For Civil Service ExamDocument1 pageHealth Form For Civil Service Examralph sabaNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageJoezerk CarpioNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PagemarieleNo ratings yet
- Health Declaration: YES NODocument1 pageHealth Declaration: YES NOEliezal Dean B. CardeñoNo ratings yet
- HDF PDFDocument1 pageHDF PDFJhon Rey GonsalezNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageFedelyn SemenianoNo ratings yet
- 2 - HEALTH DECLARATION FORM For New Hire 05292020 KTDocument1 page2 - HEALTH DECLARATION FORM For New Hire 05292020 KTpam01pamNo ratings yet
- Conquering COVID-19 with CHRIST: A Husband and His WifeaEUR(tm)s Account of a Physical Fight Versus a Spiritual Fight While Battling COVID-19From EverandConquering COVID-19 with CHRIST: A Husband and His WifeaEUR(tm)s Account of a Physical Fight Versus a Spiritual Fight While Battling COVID-19No ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Output No. 1Document2 pagesOutput No. 1Zyreane FernandezNo ratings yet
- Output No. 3Document1 pageOutput No. 3Zyreane FernandezNo ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Output No. 2Document2 pagesOutput No. 2Zyreane FernandezNo ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Graduate Studies Final Examination in Research and StatisticsDocument4 pagesGraduate Studies Final Examination in Research and StatisticsZyreane FernandezNo ratings yet
- Fourth Quarter Nationwide Simultaneous Earthquake Drill 2021Document5 pagesFourth Quarter Nationwide Simultaneous Earthquake Drill 2021Zyreane FernandezNo ratings yet
- Oral Communication in Context 1Document7 pagesOral Communication in Context 1Zyreane FernandezNo ratings yet
- Guisguis National High School: Department of Education Region III Schools Division of Zambales Sta. Cruz DistrictDocument2 pagesGuisguis National High School: Department of Education Region III Schools Division of Zambales Sta. Cruz DistrictZyreane FernandezNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesZyreane FernandezNo ratings yet
- GRADES 1-12 Daily Lesson LOG School Grade Level Teacher Learning Area Teaching Dates and Time QuarterDocument2 pagesGRADES 1-12 Daily Lesson LOG School Grade Level Teacher Learning Area Teaching Dates and Time QuarterZyreane FernandezNo ratings yet
- Guisguis, Sta. Cruz, ZambalesDocument3 pagesGuisguis, Sta. Cruz, ZambalesZyreane FernandezNo ratings yet
- Curriculum and Instruction Checklist: Indicator Level of PracticeDocument5 pagesCurriculum and Instruction Checklist: Indicator Level of PracticeZyreane FernandezNo ratings yet
- Summary All Individual Development PlanDocument12 pagesSummary All Individual Development PlanZyreane FernandezNo ratings yet
- Table of Specification: Summative TestDocument2 pagesTable of Specification: Summative TestZyreane FernandezNo ratings yet
- Class Program: GRADE 11 - TVL-HE - CookeryDocument1 pageClass Program: GRADE 11 - TVL-HE - CookeryZyreane FernandezNo ratings yet
- English 8: Department of EducationDocument3 pagesEnglish 8: Department of EducationZyreane FernandezNo ratings yet
- Sa GNHS G10 1Document2 pagesSa GNHS G10 1Zyreane FernandezNo ratings yet
- Weekly Home Learning Plan: Guisguis National High SchoolDocument2 pagesWeekly Home Learning Plan: Guisguis National High SchoolZyreane FernandezNo ratings yet
- O o o o O: Pls. Check On The Item Below That May Descried To Your StrategiesDocument1 pageO o o o O: Pls. Check On The Item Below That May Descried To Your StrategiesZyreane FernandezNo ratings yet
- WHLP Individual Earth and Life Oral Com PR2 Nov. 11 15 Week 5 With ActivitiesDocument4 pagesWHLP Individual Earth and Life Oral Com PR2 Nov. 11 15 Week 5 With ActivitiesZyreane FernandezNo ratings yet
- Summative Examination Cookery SY 2020-2021 I. Multiple Choice. Select The Best AnswerDocument2 pagesSummative Examination Cookery SY 2020-2021 I. Multiple Choice. Select The Best AnswerZyreane FernandezNo ratings yet
- RJSC Schedule XDocument3 pagesRJSC Schedule XNafisur Rahman100% (1)
- AutoInvoiceExecution - Auto Invoice Execution ReportDocument7 pagesAutoInvoiceExecution - Auto Invoice Execution ReportTommy AgustioNo ratings yet
- Every Nation Language Institute (Enli) and Ralph Martin Ligon, V. Maria Minelliedela CruzDocument2 pagesEvery Nation Language Institute (Enli) and Ralph Martin Ligon, V. Maria Minelliedela CruzMark Anthony ReyesNo ratings yet
- Offering SlipDocument6 pagesOffering SlipTanao TaoNo ratings yet
- Turkish Economy (1980-1989)Document15 pagesTurkish Economy (1980-1989)ademNo ratings yet
- Hisa PresentationDocument12 pagesHisa Presentationapi-631631105No ratings yet
- Jaiib 10 Weeks Study Plan Nov 2020Document11 pagesJaiib 10 Weeks Study Plan Nov 2020Siva BantuNo ratings yet
- David Hume My Own LifeDocument8 pagesDavid Hume My Own Lifeoolong9No ratings yet
- First Division: Charben Duarte Y Oliveros, Petitioner, vs. People of The Philippines, Respondent. DecisionDocument6 pagesFirst Division: Charben Duarte Y Oliveros, Petitioner, vs. People of The Philippines, Respondent. DecisionMarian Dominique AuroraNo ratings yet
- Legal Regulation of Cyber Crimes in IndiaDocument9 pagesLegal Regulation of Cyber Crimes in IndiaSwarnaprava DashNo ratings yet
- Introducing Tort Law in BangladeshDocument10 pagesIntroducing Tort Law in BangladeshArs Khan100% (2)
- Income ExemptDocument25 pagesIncome Exemptapi-3832224No ratings yet
- Pindi Yulinar Rosita - 008201905023 - Session 5Document7 pagesPindi Yulinar Rosita - 008201905023 - Session 5Pindi YulinarNo ratings yet
- Bernard of Clairvaux LettersDocument4 pagesBernard of Clairvaux Lettersoliver.johnson578No ratings yet
- StoppardDocument6 pagesStoppardCharlie FuentesNo ratings yet
- Iowa Supreme Court Ruling in Paternity Fraud CaseDocument27 pagesIowa Supreme Court Ruling in Paternity Fraud CaseGazetteonlineNo ratings yet
- Stuvia 1968904 lcp4807 Exam Pack Questions and Answers For 2018 2022 Download FileDocument42 pagesStuvia 1968904 lcp4807 Exam Pack Questions and Answers For 2018 2022 Download FilebchiceleganceNo ratings yet
- AZURE ACCESS AND SecurityDocument20 pagesAZURE ACCESS AND Securityamit kaishverNo ratings yet
- Leaf Obd Readthedocs Io en LatestDocument29 pagesLeaf Obd Readthedocs Io en LatestodipasNo ratings yet
- Rosh and CompanyDocument2 pagesRosh and CompanyAli KhanNo ratings yet
- Partnership ACTDocument73 pagesPartnership ACTTushar SharmaNo ratings yet
- CmmaDocument8 pagesCmmamg504100% (1)
- 201 Scra 210Document4 pages201 Scra 210Camille Grande100% (1)
- 1 XXX Vs People G.R. No. 252087Document13 pages1 XXX Vs People G.R. No. 252087ahmadjibrail dianangNo ratings yet
- MyApplication Unisa Forms M30Document1 pageMyApplication Unisa Forms M30MbaliNo ratings yet
- Speed, Time, and Distance Worksheet: Name: - DateDocument2 pagesSpeed, Time, and Distance Worksheet: Name: - Datehendrik koesumaNo ratings yet