Download as docx, pdf, or txt
You might also like
- Mental Dental Oral SurgeryDocument21 pagesMental Dental Oral SurgeryAmanda AmaroNo ratings yet
- Quick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamDocument19 pagesQuick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamWyoXPat100% (12)
- Type 2 Diabetes MellitusDocument19 pagesType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Emerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesDocument9 pagesEmerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesIndrasuari Anak Agung AyuNo ratings yet
- Type 2 Diabetes Mellitus - Prevalence and Risk Factors - UpToDateDocument36 pagesType 2 Diabetes Mellitus - Prevalence and Risk Factors - UpToDateEver LuizagaNo ratings yet
- R VI W Li9'Ery1LqeDocument28 pagesR VI W Li9'Ery1LqeV.Bastin JeromeNo ratings yet
- Diabetes: Introduction and History of The Diabetes MellitusDocument6 pagesDiabetes: Introduction and History of The Diabetes Mellitusثہيہودور'ۦ شہوأنہﮩٰۧٛۗ ﮩٰۧٛNo ratings yet
- Classification, Pathophysiology, Diagnosis and Management of DiabetesDocument19 pagesClassification, Pathophysiology, Diagnosis and Management of DiabeteswakhidrizkaNo ratings yet
- Hypoglycemia in Diabetes: P E. C, S N. D, H SDocument11 pagesHypoglycemia in Diabetes: P E. C, S N. D, H SFabio FabbriNo ratings yet
- Levels of LDL Cholesterol, Triglyceride and Urate in Patients With Type 2 Diabetes MellitusDocument8 pagesLevels of LDL Cholesterol, Triglyceride and Urate in Patients With Type 2 Diabetes Mellitusstalker2222No ratings yet
- Gudoy, Charies Jamille 12-WeierstrassDocument4 pagesGudoy, Charies Jamille 12-WeierstrasschaNo ratings yet
- The Two-Way Relationship Between Diabetes and Periodontal DiseaseDocument12 pagesThe Two-Way Relationship Between Diabetes and Periodontal DiseaseDevi AlfianiNo ratings yet
- Imune DeseaseDocument6 pagesImune DeseaseGeorge NicoloiuNo ratings yet
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2Roland Jireh MarananNo ratings yet
- Definition of Diabetes Mellitus (DM)Document12 pagesDefinition of Diabetes Mellitus (DM)Romarc Owen CorpuzNo ratings yet
- Diabetic PatientDocument16 pagesDiabetic PatientGabii OrdoñezNo ratings yet
- Diabetes MellitusDocument43 pagesDiabetes MellitusRobi HSNo ratings yet
- 20200800.0-00029 Preoperative GlucosaDocument9 pages20200800.0-00029 Preoperative GlucosaLuis OrdóñezNo ratings yet
- Iabetes Ellitus: Section 7. Endocrinologic DisordersDocument24 pagesIabetes Ellitus: Section 7. Endocrinologic DisordersAyoe SemangatzNo ratings yet
- English Assignment Journal: Created By: Amalina Nur Fadhilah P1337420217061 IibDocument3 pagesEnglish Assignment Journal: Created By: Amalina Nur Fadhilah P1337420217061 IibAmalina Nur FadhilahNo ratings yet
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocument12 pagesPolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998No ratings yet
- Type 2 Diabetes MellitusDocument24 pagesType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (2)
- Korelasi Kadar Kolesterol Dengan Kejadian Diabetes Mellitus Tipe 2 Pada Laki-LakiDocument6 pagesKorelasi Kadar Kolesterol Dengan Kejadian Diabetes Mellitus Tipe 2 Pada Laki-LakiRengganis PutriNo ratings yet
- Clinical Review 102 Type 2 Diabetes Mellitus: Update On Diagnosis, Pathophysiology, and TreatmentDocument7 pagesClinical Review 102 Type 2 Diabetes Mellitus: Update On Diagnosis, Pathophysiology, and TreatmentWyn AgustinNo ratings yet
- Classification, Pathophysiology, Diagnosis and Management of Diabetes MellitusDocument3 pagesClassification, Pathophysiology, Diagnosis and Management of Diabetes MellitusIka HabelNo ratings yet
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2MTs MIFDANo ratings yet
- Review of Literature On Diabetes, Self-Care, Quality of Life, and Psychosocial IssuesDocument8 pagesReview of Literature On Diabetes, Self-Care, Quality of Life, and Psychosocial IssuesGitaq Tri YatmaNo ratings yet
- REVIEWED Team, ch1, ch2, ch3Document20 pagesREVIEWED Team, ch1, ch2, ch3ibrahimNo ratings yet
- Management of Blood GlucoseDocument8 pagesManagement of Blood GlucoseerwanNo ratings yet
- Dia Care 2009 Kitabchi 1335 43crisis HiperglicemicasDocument9 pagesDia Care 2009 Kitabchi 1335 43crisis HiperglicemicassstdocNo ratings yet
- Guideline ADA 2010 in Hyperglicemia CrisisDocument9 pagesGuideline ADA 2010 in Hyperglicemia CrisisAissyiyah Nur An NisaNo ratings yet
- Diabetes Mellitus Its Complications Factors Influencing Complications and Prevention An Overview PDFDocument36 pagesDiabetes Mellitus Its Complications Factors Influencing Complications and Prevention An Overview PDFsarah dibaNo ratings yet
- Assessment & Treatment of Diabetic Emergencies: Paramedic LevelDocument12 pagesAssessment & Treatment of Diabetic Emergencies: Paramedic LevelSarah-kate PatersonNo ratings yet
- Heart Failure in Type 2 Diabetes Mellitus.2019Document21 pagesHeart Failure in Type 2 Diabetes Mellitus.2019Anonymous RJntvnNo ratings yet
- Update On Diabetes Mellitus: Prevention, Treatment, and Association With Oral DiseasesDocument10 pagesUpdate On Diabetes Mellitus: Prevention, Treatment, and Association With Oral DiseasesAlexandra NinaNo ratings yet
- Pathophysiology of Prediabetes and Treatment Implications For The Prevention of Type 2 Diabetes MellitusDocument10 pagesPathophysiology of Prediabetes and Treatment Implications For The Prevention of Type 2 Diabetes MellitusSamir BenmouffokNo ratings yet
- Anexo 6. UpToDate - 2022 - PrevenciónDocument32 pagesAnexo 6. UpToDate - 2022 - PrevenciónRubiNo ratings yet
- Diabetes Mellitus Type 2Document3 pagesDiabetes Mellitus Type 2Licio LentimoNo ratings yet
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataNo ratings yet
- Diabetology & Metabolic Syndrome: Post-Transplant Diabetes MellitusDocument4 pagesDiabetology & Metabolic Syndrome: Post-Transplant Diabetes MellitusVmiguel LcastilloNo ratings yet
- Metabolic Syndrome-Driving The CVD Epidemic: Diabetes: A Growing ThreatDocument6 pagesMetabolic Syndrome-Driving The CVD Epidemic: Diabetes: A Growing ThreatdoublejaydNo ratings yet
- Diabetic Research 22Document33 pagesDiabetic Research 22Hakim KhanNo ratings yet
- Prediabetes dmt2 PDFDocument10 pagesPrediabetes dmt2 PDFARIA MINDNo ratings yet
- Estado Hiperosomolar No CetósicoDocument20 pagesEstado Hiperosomolar No CetósicoilgarciaNo ratings yet
- DM Type 2 Practice EssentialsDocument31 pagesDM Type 2 Practice Essentialskuchaibaru90No ratings yet
- Ojo 2019Document6 pagesOjo 2019Marci MunirNo ratings yet
- Some Common Antidiabetic Plants of The IDocument51 pagesSome Common Antidiabetic Plants of The Icharanmann9165No ratings yet
- Diabetes Mellitus Type 2Document10 pagesDiabetes Mellitus Type 2Exia QuinagonNo ratings yet
- Diabetes Mellitus: Group 3ADocument8 pagesDiabetes Mellitus: Group 3AAradhanaRamchandaniNo ratings yet
- Diabetes Emergencia Umpierrez 2016Document11 pagesDiabetes Emergencia Umpierrez 2016Nathalie GandoNo ratings yet
- Dr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United KingdomDocument37 pagesDr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United Kingdomdwi istutikNo ratings yet
- DKD in DM2Document9 pagesDKD in DM2drjalalofficialNo ratings yet
- Hypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FDocument6 pagesHypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FHervi LaksariNo ratings yet
- Kidney ObeseDocument18 pagesKidney ObeseIrene KristiantiNo ratings yet
- Seminar: Christopher J Nolan, Peter Damm, Marc PrentkiDocument13 pagesSeminar: Christopher J Nolan, Peter Damm, Marc Prentkidanu20No ratings yet
- Evaluation of Diabetes Mellitus Type 2 Effects On Kidney FunctionDocument7 pagesEvaluation of Diabetes Mellitus Type 2 Effects On Kidney FunctionMediterr J Pharm Pharm SciNo ratings yet
- 1999-The Diabetes Prevention Program- Design and methods for a clinical trial in the prevention of type 2 diabetesDocument23 pages1999-The Diabetes Prevention Program- Design and methods for a clinical trial in the prevention of type 2 diabetesluizfernandosellaNo ratings yet
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachFrom EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachNo ratings yet
- Fast Facts: Type 2 Diabetes: Identify early, intervene effectively, make every contact countFrom EverandFast Facts: Type 2 Diabetes: Identify early, intervene effectively, make every contact countNo ratings yet
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalFrom EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalNo ratings yet
- Discover Natural -Alternative Therapies for Managing Type 2 DiabetesFrom EverandDiscover Natural -Alternative Therapies for Managing Type 2 DiabetesNo ratings yet
- Conquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsFrom EverandConquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsNo ratings yet
- How To Write An Essay: Preparation Stage (Prewriting)Document2 pagesHow To Write An Essay: Preparation Stage (Prewriting)Hannah VueltaNo ratings yet
- Drafting StageDocument2 pagesDrafting StageHannah VueltaNo ratings yet
- Narrative Essays: The Narrative Essay Focuses On A Specific Plot. It InvolvesDocument2 pagesNarrative Essays: The Narrative Essay Focuses On A Specific Plot. It InvolvesHannah VueltaNo ratings yet
- How A Visit To A Bread Factory in Mongolia Led To A Reduction in Salt OvernightDocument1 pageHow A Visit To A Bread Factory in Mongolia Led To A Reduction in Salt OvernightHannah VueltaNo ratings yet
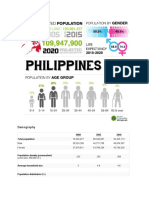
- Demography: 2000 2007 2010 Total PopulationDocument2 pagesDemography: 2000 2007 2010 Total PopulationHannah VueltaNo ratings yet
- How A Visit To A Bread Factory in Mongolia Led To A Reduction in Salt OvernightDocument1 pageHow A Visit To A Bread Factory in Mongolia Led To A Reduction in Salt OvernightHannah VueltaNo ratings yet
- A Bread Factory in Mongolia Led To A Reduction in Salt OvernightDocument2 pagesA Bread Factory in Mongolia Led To A Reduction in Salt OvernightHannah VueltaNo ratings yet
- Mitchell Greene: St. Petersburg, FlaDocument5 pagesMitchell Greene: St. Petersburg, FlaHannah VueltaNo ratings yet
- Led To A Reduction in Salt OvernightDocument1 pageLed To A Reduction in Salt OvernightHannah VueltaNo ratings yet
- Key Topics by Field: Sociocultural: LinguisticDocument3 pagesKey Topics by Field: Sociocultural: LinguisticHannah VueltaNo ratings yet
- On The Origin of Species: Review, Hunt Stressed The Work of Waitz, Adopting His Definitions As A StandardDocument2 pagesOn The Origin of Species: Review, Hunt Stressed The Work of Waitz, Adopting His Definitions As A StandardHannah VueltaNo ratings yet
- Mongolia Led To A Reduction in Salt OvernightDocument1 pageMongolia Led To A Reduction in Salt OvernightHannah VueltaNo ratings yet
- ScribdDocument2 pagesScribdHannah VueltaNo ratings yet
- Sage Tzamouranis: Ridgefield, ConnDocument5 pagesSage Tzamouranis: Ridgefield, ConnHannah VueltaNo ratings yet
- Sociocultural: Cultural Anthropology Social Anthropology Sociocultural AnthropologyDocument1 pageSociocultural: Cultural Anthropology Social Anthropology Sociocultural AnthropologyHannah VueltaNo ratings yet
- Dylan Morse: Ithaca, N.YDocument5 pagesDylan Morse: Ithaca, N.YHannah VueltaNo ratings yet
- Addison Amadeck: Kirkland, WashDocument4 pagesAddison Amadeck: Kirkland, WashHannah Vuelta100% (1)
- 20th and 21st CenturiesDocument1 page20th and 21st CenturiesHannah VueltaNo ratings yet
- Alexander Mclaughlin: Lexington, MassDocument4 pagesAlexander Mclaughlin: Lexington, MassHannah VueltaNo ratings yet
- A Killer First Sentence. You've Heard It Before, And: 22 First Sentences From Stanford ApplicantsDocument5 pagesA Killer First Sentence. You've Heard It Before, And: 22 First Sentences From Stanford ApplicantsHannah VueltaNo ratings yet
- Epi ReviewerDocument4 pagesEpi ReviewerHannah VueltaNo ratings yet
- A Reflection AbDocument1 pageA Reflection AbHannah VueltaNo ratings yet
- Lab Activity PcolDocument15 pagesLab Activity PcolHannah VueltaNo ratings yet
- Receptor ProteinDocument7 pagesReceptor Proteinandrej.gregorcicNo ratings yet
- Aminoglycosides AntibioticsDocument2 pagesAminoglycosides AntibioticsHlaSoe WinNo ratings yet
- 4 November 2004 DR - Supparearg DisayabutrDocument38 pages4 November 2004 DR - Supparearg DisayabutrDonnaya KrajangwittayaNo ratings yet
- AComprehensive Algorithm For Management of Neuropathic Pain PDFDocument15 pagesAComprehensive Algorithm For Management of Neuropathic Pain PDFSussan AguedoNo ratings yet
- NeuropsychiatryDocument5 pagesNeuropsychiatryNicole TangcoNo ratings yet
- Fundamentals in NursingDocument15 pagesFundamentals in NursingAngie Bucio MiraNo ratings yet
- ARNI in Cardiovascular, Current UpdateDocument12 pagesARNI in Cardiovascular, Current Updatefazlur risyad laochiNo ratings yet
- MEDICAL MYCOLOGY Dr. Caligagan 2017 HP PDFDocument23 pagesMEDICAL MYCOLOGY Dr. Caligagan 2017 HP PDFROSEMARIE ONGNo ratings yet
- Hypertension: EpidemiologyDocument4 pagesHypertension: Epidemiologyu105022301No ratings yet
- Anemia - WikipediaDocument36 pagesAnemia - WikipediaAbebe TadesseNo ratings yet
- 5-Heart FailureDocument12 pages5-Heart FailureJericho De GuzmanNo ratings yet
- Metal Poisoning - Mercury, Lead, Cadmium: Lecture No. 9Document19 pagesMetal Poisoning - Mercury, Lead, Cadmium: Lecture No. 9lauraNo ratings yet
- Management of Kidney Diseases 2023Document579 pagesManagement of Kidney Diseases 2023Mauricio LopezNo ratings yet
- Worksheet 7 Endocrine Digestive Urinary Repro Eehhh Final PDFDocument31 pagesWorksheet 7 Endocrine Digestive Urinary Repro Eehhh Final PDFkaejane gonzagaNo ratings yet
- Gejala Gangguan JiwaDocument8 pagesGejala Gangguan Jiwakevin stefanoNo ratings yet
- CD RationalizationDocument19 pagesCD RationalizationAnastasya Gishella RorongNo ratings yet
- Summary of DrugsDocument19 pagesSummary of DrugsAthena BendoNo ratings yet
- Flovent (Fluticasone)Document3 pagesFlovent (Fluticasone)Adrianne BazoNo ratings yet
- Prometric Mcqs Plus CaculationsDocument147 pagesPrometric Mcqs Plus CaculationsShanaz KhanNo ratings yet
- 311-Article Text-307-1-10-20140612Document6 pages311-Article Text-307-1-10-20140612Shaun TylerNo ratings yet
- Syncope: Global Cerebral Blood FlowDocument7 pagesSyncope: Global Cerebral Blood FlowChananNo ratings yet
- Students Medical Record Form Updated 12-15-23 2Document2 pagesStudents Medical Record Form Updated 12-15-23 2Kim SosaNo ratings yet
- HAAD Exam SampleDocument14 pagesHAAD Exam SampleSAHYA TRADCONo ratings yet
- Sas 17Document3 pagesSas 17Sistine Rose LabajoNo ratings yet
- Respi Hema NotesDocument16 pagesRespi Hema NotesLucky GomezNo ratings yet
- APGT Laser Procedures - CH IVDocument31 pagesAPGT Laser Procedures - CH IV_ele_mentalNo ratings yet
- Management of Patients With Renal DisordersDocument29 pagesManagement of Patients With Renal DisordersokaciaNo ratings yet
- Common Causes of HypoxemiaDocument6 pagesCommon Causes of HypoxemiaSamantha LuiNo ratings yet