Download as pdf or txt
You might also like
- Siretokituzisi Kinobody Superhero Download Xonanub PDFDocument5 pagesSiretokituzisi Kinobody Superhero Download Xonanub PDFRafaela Gomes33% (3)
- Luborsky, Lester - Principles of Psychoanalytic Psychotherapy PDFDocument295 pagesLuborsky, Lester - Principles of Psychoanalytic Psychotherapy PDFMario Hernández Jr.No ratings yet
- Cardiology II WorkbookDocument70 pagesCardiology II WorkbookPharmacist Dina100% (1)
- Amlodipine AtenololDocument7 pagesAmlodipine AtenololBidhur Chakma 1935371673No ratings yet
- Antihypertensive Ef Cacy of The Angiotensin Receptor BlockerDocument8 pagesAntihypertensive Ef Cacy of The Angiotensin Receptor BlockerAlan Yaser GroChaNo ratings yet
- 12 - 2015 - LT Safety and Efficacy of Imatinib in PAH - IMPRES (10) 70Document10 pages12 - 2015 - LT Safety and Efficacy of Imatinib in PAH - IMPRES (10) 70edward the iiiNo ratings yet
- Amlodipine/Valsartan (Avsar®) : Efficacy in Hypertensive Patients - A Real World Observational Study (ALERT)Document6 pagesAmlodipine/Valsartan (Avsar®) : Efficacy in Hypertensive Patients - A Real World Observational Study (ALERT)Kamar OperasiNo ratings yet
- Adhrence 1Document9 pagesAdhrence 1nabilahbilqisNo ratings yet
- Prescription Patterns of Antihypertensives in A Community Health Centre in Mexico City: A Drug Utilization StudyDocument6 pagesPrescription Patterns of Antihypertensives in A Community Health Centre in Mexico City: A Drug Utilization StudyWendy Garduño SandovalNo ratings yet
- Prescribing Pattern of Antihypertensive Drugs in A Tertiary Care Hospital in Jammu-A Descriptive StudyDocument4 pagesPrescribing Pattern of Antihypertensive Drugs in A Tertiary Care Hospital in Jammu-A Descriptive StudyMahantesh NyayakarNo ratings yet
- Adequacy of Blood Pressure Control and Level of Adherence With Antihypertensive TherapyDocument8 pagesAdequacy of Blood Pressure Control and Level of Adherence With Antihypertensive TherapyDr YusufNo ratings yet
- Cost Effectiveness and Resource AllocationDocument7 pagesCost Effectiveness and Resource AllocationSarah AmeliaNo ratings yet
- The Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsDocument9 pagesThe Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsLucky PratamaNo ratings yet
- E2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Document1 pageE2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Sadam_fasterNo ratings yet
- Phco 23 15 1564 31963Document9 pagesPhco 23 15 1564 31963كسلان اكتب اسميNo ratings yet
- Telmisartan For Treatment of Covid-19 Patients: An Open Multicenter Randomized Clinical TrialDocument4 pagesTelmisartan For Treatment of Covid-19 Patients: An Open Multicenter Randomized Clinical TrialTeam - MEDICALSERVICESNo ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- Exercise Stress Test As An Antidote For Anxiety Ne PDFDocument2 pagesExercise Stress Test As An Antidote For Anxiety Ne PDFmehrshad Farahpour Gp5No ratings yet
- BPJ Vol 11 No 2 P 821-825Document5 pagesBPJ Vol 11 No 2 P 821-825hendriNo ratings yet
- Maroon and Teal Employee NewsletterDocument4 pagesMaroon and Teal Employee NewsletterMediception ScienceNo ratings yet
- Diagnosis and Management of Resistant Hypertension: State of The ArtDocument14 pagesDiagnosis and Management of Resistant Hypertension: State of The ArtMario HBNo ratings yet
- Testing For Primary Hyperaldosteronism and MRA TX Annals 2020Document10 pagesTesting For Primary Hyperaldosteronism and MRA TX Annals 2020Miri PravdaNo ratings yet
- Medication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsDocument10 pagesMedication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsmadhurocksktmNo ratings yet
- VHRM 7 085Document11 pagesVHRM 7 085AldiKurosakiNo ratings yet
- Arterial HypertensionDocument13 pagesArterial HypertensionZedodurex100% (1)
- Pos-676 Exploratory Study To Assess The Safety of Sublingual Oil Based Medical Cannabis Bol-Dp-O-04 in Dialysis Patients Who Have Chronic PainDocument1 pagePos-676 Exploratory Study To Assess The Safety of Sublingual Oil Based Medical Cannabis Bol-Dp-O-04 in Dialysis Patients Who Have Chronic PainDavids MarinNo ratings yet
- JJJGJHGJHGHDocument6 pagesJJJGJHGJHGHTaufik NurohmanNo ratings yet
- 8400-Article Text-50016-1-10-20090108Document5 pages8400-Article Text-50016-1-10-20090108Dammi LauNo ratings yet
- Review of LiteratureDocument9 pagesReview of LiteratureJEMY JOSENo ratings yet
- CPG Management of Hypertension (3rd Edition)Document44 pagesCPG Management of Hypertension (3rd Edition)patricktiew100% (2)
- HYVET Pilot. JHypertens Dec 2003.Document9 pagesHYVET Pilot. JHypertens Dec 2003.Irma SetiawatiNo ratings yet
- Byrd 2019Document22 pagesByrd 2019Miriam TorresNo ratings yet
- Evidence-Based Medical Treatment of Peripheral Arterial Disease: A Rapid ReviewDocument14 pagesEvidence-Based Medical Treatment of Peripheral Arterial Disease: A Rapid ReviewLeo OoNo ratings yet
- Prehypertensive State, Mild Hypertension, Metabolic Syndrome and Cardiovascular Risk Factors Among Young Adults in Rural MalaysiaDocument8 pagesPrehypertensive State, Mild Hypertension, Metabolic Syndrome and Cardiovascular Risk Factors Among Young Adults in Rural MalaysiaIndah SundariNo ratings yet
- Full Text 01Document8 pagesFull Text 01febyNo ratings yet
- 10 1177@1074248418769054Document11 pages10 1177@1074248418769054Bidhur Chakma 1935371673No ratings yet
- Evaluation of Medication Adherence in Lebanese Hypertensive PatientsDocument11 pagesEvaluation of Medication Adherence in Lebanese Hypertensive PatientsDoddo IndrayanaNo ratings yet
- Norepinefri in AritmiaDocument8 pagesNorepinefri in AritmiaANISA RACHMITA ARIANTI 2020No ratings yet
- Interaction of Coadministered Amlodipine and Atorvastatin in 1660 Patients With ConcomitantDocument16 pagesInteraction of Coadministered Amlodipine and Atorvastatin in 1660 Patients With ConcomitantLuciana OliveiraNo ratings yet
- HepaDocument10 pagesHepaJohana Zamudio RojasNo ratings yet
- Fifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDocument6 pagesFifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDavid RamirezNo ratings yet
- SA Hypertension GuidelinesDocument26 pagesSA Hypertension GuidelinesMaleehaNo ratings yet
- 14 - Mazandarani2012Document7 pages14 - Mazandarani2012TandeanTommyNovenantoNo ratings yet
- 2016 Article 42 PDFDocument8 pages2016 Article 42 PDFSandhya kumarNo ratings yet
- Tsuyuki 2002Document7 pagesTsuyuki 2002Basilharbi HammadNo ratings yet
- Risk Factors and Complications of Subconjunctival Hemorrhages in Patients Taking WarfarinDocument5 pagesRisk Factors and Complications of Subconjunctival Hemorrhages in Patients Taking WarfarinSyafar Agus Al-Fath MukminNo ratings yet
- A Comparison of The Efficacy and Safety of irbesartan/HCTZ Combination Therapy With Irbesartan and HCTZ Monotherapy in The Treatment of Moderate HypertensionDocument9 pagesA Comparison of The Efficacy and Safety of irbesartan/HCTZ Combination Therapy With Irbesartan and HCTZ Monotherapy in The Treatment of Moderate HypertensionBarbara Sakura RiawanNo ratings yet
- Cost-Minimization and The Number Needed To Treat in Uncomplicated HypertensionDocument12 pagesCost-Minimization and The Number Needed To Treat in Uncomplicated HypertensionIndermeet Singh AnandNo ratings yet
- Assessment of Patient's Knowledge, Attitude and Practice Regarding HypertensionDocument6 pagesAssessment of Patient's Knowledge, Attitude and Practice Regarding HypertensionScintya NasutionNo ratings yet
- 35th Vicenza Course On Aki & CRRT: Selected Abstracts From TheDocument27 pages35th Vicenza Course On Aki & CRRT: Selected Abstracts From TheMARIA LEIVANo ratings yet
- HiertensiDocument2 pagesHiertensiCindy AmeLiyana Part IINo ratings yet
- JR BM Dok HartonoDocument1 pageJR BM Dok Hartonofadhil mar'ie muhammadNo ratings yet
- XimlagaltranDocument9 pagesXimlagaltranDQ DQNo ratings yet
- Case StudiesDocument5 pagesCase Studiespragna novaNo ratings yet
- VHRM 5 1043Document16 pagesVHRM 5 1043AldiKurosakiNo ratings yet
- Laprosy Research Paper (Ahmed Tanjimul Islam)Document7 pagesLaprosy Research Paper (Ahmed Tanjimul Islam)AHMED TANJIMUL ISLAMNo ratings yet
- 1 s2.0 S0007091217542075 MainDocument11 pages1 s2.0 S0007091217542075 Maineny_sumaini65No ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Hypertension in High Risk African Americans: Current Concepts, Evidence-based Therapeutics and Future ConsiderationsFrom EverandHypertension in High Risk African Americans: Current Concepts, Evidence-based Therapeutics and Future ConsiderationsNo ratings yet
- Sigma Theta Tau InternationalDocument10 pagesSigma Theta Tau InternationalpsubetasigmaNo ratings yet
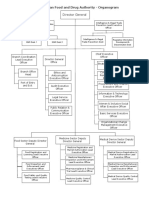
- EFDA Organogram English VersionDocument6 pagesEFDA Organogram English VersionRobsan YasinNo ratings yet
- Utk Thesis DefenseDocument5 pagesUtk Thesis Defenseafcnwwgnt100% (2)
- Match The Words On The Left With The Words On The Right To Form CollocationsDocument2 pagesMatch The Words On The Left With The Words On The Right To Form CollocationsirmaNo ratings yet
- Trauma Triad of DeathDocument5 pagesTrauma Triad of DeathTomNo ratings yet
- Informative SpeechDocument3 pagesInformative Speechapi-534130899No ratings yet
- Pathologists AssistaDocument2 pagesPathologists AssistamabrieNo ratings yet
- BASC-2 Q Global Score Summary SampleDocument11 pagesBASC-2 Q Global Score Summary SamplegenacartaNo ratings yet
- Open University Isced Department of Education Sciences Portuguese Teaching Degree CourseDocument14 pagesOpen University Isced Department of Education Sciences Portuguese Teaching Degree CourseValdemiro NhantumboNo ratings yet
- 2ND Quarterly Meeting For BbiDocument4 pages2ND Quarterly Meeting For BbiRuth PerezNo ratings yet
- Urokinase Dosage WheelDocument2 pagesUrokinase Dosage WheelNidhiNo ratings yet
- Cont EduDocument18 pagesCont EduShilu Mathai PappachanNo ratings yet
- Women and Birth: Olivia Tierney, Linda Sweet, Don Houston, Lyn EbertDocument6 pagesWomen and Birth: Olivia Tierney, Linda Sweet, Don Houston, Lyn EbertputrigunawanNo ratings yet
- Sam Josh SMP SlidesDocument17 pagesSam Josh SMP SlidesJpt YapNo ratings yet
- Mary Janet C. Gorriceta Blk. 21 Zone 3 Bo - Obrero Iloilo City Mobile #: 09302029037 E-Mail AddressDocument8 pagesMary Janet C. Gorriceta Blk. 21 Zone 3 Bo - Obrero Iloilo City Mobile #: 09302029037 E-Mail AddressDick Morgan FerrerNo ratings yet
- Dry Socket ManagementDocument7 pagesDry Socket ManagementNuzhat Noor AyeshaNo ratings yet
- SSRSDocument20 pagesSSRSElle ManalangNo ratings yet
- Occimun Sanctum Tulsi DeviDocument9 pagesOccimun Sanctum Tulsi DeviBenancio DorantessNo ratings yet
- Reflection 4Document2 pagesReflection 4api-276689443No ratings yet
- Are The Foods You Are Eating Today Starving Your Brain by Eugene Schwartz PDFDocument1 pageAre The Foods You Are Eating Today Starving Your Brain by Eugene Schwartz PDFBrian ColborneNo ratings yet
- Gout - Anusha V HDocument11 pagesGout - Anusha V HAnusha VhNo ratings yet
- Hygienic Requirements of Food and Drink EstablishmentsDocument25 pagesHygienic Requirements of Food and Drink Establishmentssneh7335No ratings yet
- Haider AliDocument10 pagesHaider Aliareeb078No ratings yet
- Examples of IELTS Speaking Part 1 QuestionsDocument15 pagesExamples of IELTS Speaking Part 1 QuestionsThanh TrầnNo ratings yet
- Well Prolong Long Started Subjects Find Extent: Set/groupDocument7 pagesWell Prolong Long Started Subjects Find Extent: Set/groupJohnny JohnnieeNo ratings yet
- Diverticulitis: Clinical PracticeDocument10 pagesDiverticulitis: Clinical PracticeZilvia EhrlichNo ratings yet
- Nursing Student's Anxiety About Career During The Pandemic Covid-19Document5 pagesNursing Student's Anxiety About Career During The Pandemic Covid-19Popi SopiahNo ratings yet