Download as docx, pdf, or txt
You might also like
- F.H. Schweingruber Tree Rings. Basics and Applications of DendrochronologyDocument289 pagesF.H. Schweingruber Tree Rings. Basics and Applications of DendrochronologyLuis David Huayta100% (1)
- MTS Vocab 2023Document9 pagesMTS Vocab 2023Rahul Chauhan100% (1)
- Medicine Long Cases - DR - PraveenDocument118 pagesMedicine Long Cases - DR - Praveendileepa madurangaNo ratings yet
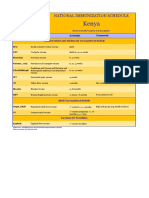
- Kenya Immunization ScheduleDocument1 pageKenya Immunization ScheduleDani AnyikaNo ratings yet
- MCQ Trop-Med All - KARUNDocument23 pagesMCQ Trop-Med All - KARUNDapot SianiparNo ratings yet
- Answers-: Review Exerc Se Nage To MeccaDocument9 pagesAnswers-: Review Exerc Se Nage To Meccafadly krNo ratings yet
- HepatitisDocument6 pagesHepatitisJulian VasquezNo ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- PyomeningitisDocument54 pagesPyomeningitisRiya BagdiNo ratings yet
- Hepatitis B: Steve HartDocument36 pagesHepatitis B: Steve HartangelinaNo ratings yet
- Bacterial InfectiousDocument7 pagesBacterial InfectioussamioNo ratings yet
- AnthraxDocument20 pagesAnthraxanemenyeeNo ratings yet
- Cap CPGDocument40 pagesCap CPGMary Joy Oros-VallejeraNo ratings yet
- Streptococci and Enterococci and OthersDocument11 pagesStreptococci and Enterococci and OthersthedarkwingNo ratings yet
- TB Guideline PregnancyDocument15 pagesTB Guideline PregnancyIsekai GamerNo ratings yet
- Foreign Body AspirationDocument3 pagesForeign Body AspirationAsiya ZaidiNo ratings yet
- Paediatric Antibiotic TeddyDocument1 pagePaediatric Antibiotic Teddyayu fitrianiNo ratings yet
- NELSON's HOUR Approach To FeverDocument30 pagesNELSON's HOUR Approach To FeverdessabalerosNo ratings yet
- Community Acquired Bacterial Meningitis in AdultsDocument45 pagesCommunity Acquired Bacterial Meningitis in AdultsDaniel Tettamanti MirandaNo ratings yet
- Respiratory Tract InfectionDocument6 pagesRespiratory Tract Infectionjovmac2uNo ratings yet
- Haematological Profile of Severe Acute Malnourished Children Admitted at Our InstitutionDocument4 pagesHaematological Profile of Severe Acute Malnourished Children Admitted at Our InstitutionIJAR JOURNALNo ratings yet
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDocument15 pagesCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarNo ratings yet
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Document38 pages2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNo ratings yet
- Acute Pneumonia: Richard T. Ellison III and Gerald R. DonowitzDocument30 pagesAcute Pneumonia: Richard T. Ellison III and Gerald R. DonowitzNilay ChatterjeeNo ratings yet
- Acute Management of Burns in ChildrenDocument52 pagesAcute Management of Burns in ChildrenJonie Vince SañosaNo ratings yet
- Bladder Cancer LancetDocument11 pagesBladder Cancer LancetYesenia HuertaNo ratings yet
- Cervical Pathology 4Document104 pagesCervical Pathology 4Arie PratamaNo ratings yet
- Antivirals & AntifungalsDocument51 pagesAntivirals & AntifungalsanojNo ratings yet
- 4 PEDIA 8 - Bleeding DisordersDocument5 pages4 PEDIA 8 - Bleeding DisordersRainy Liony DuhNo ratings yet
- Pediatric Palliative Care Referral CriteriaDocument7 pagesPediatric Palliative Care Referral Criteriaapi-197110397No ratings yet
- PSGNDocument23 pagesPSGNalpha mae beltranNo ratings yet
- Clinical Management: PGI Eileen Andres PediatricsDocument9 pagesClinical Management: PGI Eileen Andres PediatricsMichael BonillaNo ratings yet
- H.influenzae Modified 2012Document12 pagesH.influenzae Modified 2012MoonAIRNo ratings yet
- Medically Significant BacteriaDocument4 pagesMedically Significant BacteriaKaren SanrilleNo ratings yet
- Treatment of Acute PharyngitisDocument4 pagesTreatment of Acute PharyngitisZafira Ananda RaishaNo ratings yet
- Pertussis: 1. Disease ReportingDocument18 pagesPertussis: 1. Disease Reportingzenagit123456No ratings yet
- Anti Microbial NotesDocument10 pagesAnti Microbial NotesMohammed Faisal UddinNo ratings yet
- Bordetella Pertussis and Whooping CoughDocument22 pagesBordetella Pertussis and Whooping CoughDian TikaNo ratings yet
- Pneumonia Template 1Document1 pagePneumonia Template 1洪靖儀No ratings yet
- Role of Homeopathy in Infectious Diseases Rajeev Saxena.03949 - 1contents PDFDocument4 pagesRole of Homeopathy in Infectious Diseases Rajeev Saxena.03949 - 1contents PDFTaani ChakrabortyNo ratings yet
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 pagesRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueNo ratings yet
- K.6 PicoDocument9 pagesK.6 PicoSteven FongNo ratings yet
- 5.0orthomyxoviruses 3.1Document41 pages5.0orthomyxoviruses 3.1Jiya MuhammadNo ratings yet
- Recent Update in The Management of Invasive Fungal InfectionDocument30 pagesRecent Update in The Management of Invasive Fungal Infectionanoop61100% (3)
- Gyne - Hepa BDocument17 pagesGyne - Hepa BonijinoNo ratings yet
- 1.basic Final McqsDocument78 pages1.basic Final McqsPrabhat KcNo ratings yet
- Malaria Treatment TableDocument9 pagesMalaria Treatment Tableاحمد عرفاتNo ratings yet
- Shanz - Pedia Ii 2.05Document3 pagesShanz - Pedia Ii 2.05Petrina XuNo ratings yet
- Infectious Diseases - Infective EndocarditisDocument41 pagesInfectious Diseases - Infective Endocarditisfire_n_iceNo ratings yet
- Patient With Fever PDFDocument46 pagesPatient With Fever PDFNosheen hafeez100% (1)
- Refkas CondylomaAccuminataDocument18 pagesRefkas CondylomaAccuminatamichelle1945No ratings yet
- Mycobacteria BPTDocument26 pagesMycobacteria BPTbpt2No ratings yet
- Clinical Examination of The Abdomen in Adult CattleDocument15 pagesClinical Examination of The Abdomen in Adult CattleStefanySalasNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Otitis Externa: Straight To The Point of CareDocument45 pagesOtitis Externa: Straight To The Point of CareNana OkujavaNo ratings yet
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- Blood and Tissue ProtozoaDocument32 pagesBlood and Tissue ProtozoaFort SalvadorNo ratings yet
- PSM Golden PointsDocument43 pagesPSM Golden PointsRutujaNo ratings yet
- Pneumonia: Submitted To:Ms Lisette Cruz Submitted By: Ms. Mely Rose AbanadorDocument26 pagesPneumonia: Submitted To:Ms Lisette Cruz Submitted By: Ms. Mely Rose AbanadorJoyce Catherine Buquing UysecoNo ratings yet
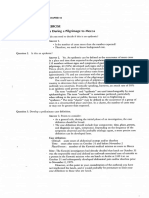
- An Outbreak of Enteritis During A Pilgrimage To MeccaDocument16 pagesAn Outbreak of Enteritis During A Pilgrimage To MeccaDannyNo ratings yet
- 2.epidemiology and Diseases TransmissionDocument28 pages2.epidemiology and Diseases TransmissionahmadwaluyoNo ratings yet
- Natural History and Spectrum of DiseaseDocument3 pagesNatural History and Spectrum of DiseaseEvans MogakaNo ratings yet
- Corak Penafsiran Al-Qur'An Periode Klasik Hingga Modern: DanialDocument33 pagesCorak Penafsiran Al-Qur'An Periode Klasik Hingga Modern: Danialyudha agustriNo ratings yet
- TGS 11Document2 pagesTGS 11yudha agustriNo ratings yet
- Appositive ExerciseDocument1 pageAppositive Exerciseyudha agustriNo ratings yet
- Exercise 4Document1 pageExercise 4yudha agustriNo ratings yet
- 4th Meeting Exercise AnswerDocument2 pages4th Meeting Exercise Answeryudha agustriNo ratings yet
- Pemaknaan Iklan Djarum 76 Versi Teman Hidup (Analisis Semiotika Roland Barthes) Oleh: Rudi KurniawanDocument15 pagesPemaknaan Iklan Djarum 76 Versi Teman Hidup (Analisis Semiotika Roland Barthes) Oleh: Rudi Kurniawanyudha agustriNo ratings yet
- Business Customer Information FormDocument6 pagesBusiness Customer Information FormFaith Anne LuenaNo ratings yet
- Fellowship Cover LetterDocument5 pagesFellowship Cover Letterxjfahwegf100% (1)
- Historical Issues in The Book of Daniel (Review) - Thomas Gaston PDFDocument2 pagesHistorical Issues in The Book of Daniel (Review) - Thomas Gaston PDFDave MoreNo ratings yet
- Blank Noise Ass TemplateDocument16 pagesBlank Noise Ass TemplateDucVikingNo ratings yet
- Science and Civilisation in China Needham 3 - 1 PDFDocument500 pagesScience and Civilisation in China Needham 3 - 1 PDFКалин Константин100% (1)
- Modifiers - Misplaced & Dangling 036 KeyDocument4 pagesModifiers - Misplaced & Dangling 036 KeyynahNo ratings yet
- Towards A Radical RizalDocument34 pagesTowards A Radical RizalBryle CamaroteNo ratings yet
- OOP With C++Document8 pagesOOP With C++Vikram RaoNo ratings yet
- Yfm70Ry Yfm70Ry Yfm70Ry: (1S3R) (1S3V) (1S3L)Document76 pagesYfm70Ry Yfm70Ry Yfm70Ry: (1S3R) (1S3V) (1S3L)Ventas CaliNo ratings yet
- An Intro To NTDocument6 pagesAn Intro To NTmylove777No ratings yet
- SANICO, MARY CONIE T. Financial Statements of Sakag-Kabuhi Inc.Document12 pagesSANICO, MARY CONIE T. Financial Statements of Sakag-Kabuhi Inc.Luigi Enderez BalucanNo ratings yet
- Racquet Sports IndustryDocument44 pagesRacquet Sports IndustryLiya DavidovNo ratings yet
- Chapter 3 Lesson 1Document64 pagesChapter 3 Lesson 1Catherine PilipasNo ratings yet
- S.S.C Public Examination: Model Paper-1 General Science Paper - 1Document4 pagesS.S.C Public Examination: Model Paper-1 General Science Paper - 1Dhatri Subasri Navya KNo ratings yet
- Lightning and LWC Interview QuestionsDocument9 pagesLightning and LWC Interview QuestionslakshmiumaNo ratings yet
- 30 IELTS Writing Band 8.0Document31 pages30 IELTS Writing Band 8.0Elize WillyNo ratings yet
- Group 7 Selecting Channel PartnersDocument24 pagesGroup 7 Selecting Channel PartnersJillian Salipande AbulenciaNo ratings yet
- Piping Materials Match Chart (ASTM) - ProjectmaterialsDocument14 pagesPiping Materials Match Chart (ASTM) - ProjectmaterialsdhurjatibhuteshNo ratings yet
- 1 - Legal Environment of BusinessDocument20 pages1 - Legal Environment of BusinessTonmoy (123011100)No ratings yet
- 1 A Story of A Failure: Management's Summary: A Worker Drilled Into The Top of A 5 GallonDocument32 pages1 A Story of A Failure: Management's Summary: A Worker Drilled Into The Top of A 5 GallonRauf HuseynovNo ratings yet
- Notice of Entry of Appearance As Attorney or Accredited RepresentativeDocument4 pagesNotice of Entry of Appearance As Attorney or Accredited Representativeyefreson9417No ratings yet
- Mca54 55 E4Document2 pagesMca54 55 E4amitnpatel1No ratings yet
- TAMIFLUDocument21 pagesTAMIFLUjaphetnwapiNo ratings yet
- How To Write An EssayDocument4 pagesHow To Write An EssayShah BaibrassNo ratings yet
- "You Shall Not Take The Name of The Lord Your God in Vain": Anger Coarse Vulgar Speech, ProfanityDocument10 pages"You Shall Not Take The Name of The Lord Your God in Vain": Anger Coarse Vulgar Speech, ProfanityMarvin MonterosoNo ratings yet
- Biochem 12th Sept Amino AcidDocument4 pagesBiochem 12th Sept Amino AcidShreeraj BadgujarNo ratings yet
- Skripsi #2 HyperlinkDocument19 pagesSkripsi #2 HyperlinkAnisah RachmawatiNo ratings yet
- The Gorgon's HeadDocument3 pagesThe Gorgon's HeadReden Macaraeg Juego100% (1)