Download as pdf or txt
You might also like
- Burket's Oral Medicine 13th Ed Michael GlickDocument1,139 pagesBurket's Oral Medicine 13th Ed Michael Glickdrendodontist100% (14)
- Child Information Sheet: Male FemaleDocument2 pagesChild Information Sheet: Male FemaleBrgy. M. Parang88% (8)
- Clinical Practice Experience (CPE) Record 5 Phase 1Document11 pagesClinical Practice Experience (CPE) Record 5 Phase 1Sammy ChegeNo ratings yet
- Ey Value of Health Care Data v20 FinalDocument36 pagesEy Value of Health Care Data v20 FinalScott FanNo ratings yet
- Marketing Research Chapter Case Block-2 Ch.5Document4 pagesMarketing Research Chapter Case Block-2 Ch.5v_rat0% (1)
- Chronic Leg Edema Exercises Brochure - EN (LR) PDFDocument2 pagesChronic Leg Edema Exercises Brochure - EN (LR) PDFsilkofosNo ratings yet
- 41ST Annual Intensive Review of Internal Medicine PDFDocument3,817 pages41ST Annual Intensive Review of Internal Medicine PDFSundus S100% (2)
- Internet Based TreatmentDocument10 pagesInternet Based TreatmentnaveedNo ratings yet
- Concordance, Adherence and Compliance in Medicine TakingDocument16 pagesConcordance, Adherence and Compliance in Medicine TakingYikber GebremeskelNo ratings yet
- Value Based HealthcareDocument48 pagesValue Based HealthcareAsem Shadid100% (1)
- Utilizing Ehealth and Telemedicine Technologies To Enhance Access and Quality of Consultations: It'S Not What You Say, It'S The Way You Say ItDocument7 pagesUtilizing Ehealth and Telemedicine Technologies To Enhance Access and Quality of Consultations: It'S Not What You Say, It'S The Way You Say ItNoemi Salazar AbantoNo ratings yet
- 11 3 23 Tonya Project Themes PapenotesDocument32 pages11 3 23 Tonya Project Themes PapenotesGeoffrey OdhiamboNo ratings yet
- Capstone Project Report MBA 702A, 703A, 704A Indian Institute of Technology, KanpurDocument13 pagesCapstone Project Report MBA 702A, 703A, 704A Indian Institute of Technology, KanpurPrakhar DikshitNo ratings yet
- Comprehensive Care PhysicianDocument9 pagesComprehensive Care PhysiciannurNo ratings yet
- Disease Management For DiabetesDocument95 pagesDisease Management For DiabetesNational Pharmaceutical Council100% (6)
- Laude 2020Document9 pagesLaude 2020Heryanti PusparisaNo ratings yet
- UntitledDocument15 pagesUntitledMARTIN DANIEL COLMENAREZ RODRIGUEZNo ratings yet
- Patient Care Management 1 and 2Document128 pagesPatient Care Management 1 and 2Lantana MedikaNo ratings yet
- Journal Pone 0290976Document21 pagesJournal Pone 0290976torrechantehansangeloNo ratings yet
- Contingency Management Approach: Implementation and OutcomesDocument112 pagesContingency Management Approach: Implementation and OutcomesArun SharmaNo ratings yet
- Nurs 390 Group 2 Project 2Document33 pagesNurs 390 Group 2 Project 2api-621785757No ratings yet
- Surgical EpisodeDocument10 pagesSurgical EpisodeAimen NasirNo ratings yet
- Journal PneumoniaDocument1 pageJournal PneumoniaDerick Keith YawanNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- 2 PBDocument19 pages2 PBPralhad TalavanekarNo ratings yet
- Deloitte Uk Patient Support ProgrammesDocument15 pagesDeloitte Uk Patient Support Programmesvishwagreat24No ratings yet
- Oncology PDFDocument7 pagesOncology PDFYesi RestinaNo ratings yet
- Rea2004 PDFDocument7 pagesRea2004 PDFTisna WennyNo ratings yet
- JPM 12 00643Document12 pagesJPM 12 00643dw21541No ratings yet
- (1998) Chronic Disease Management What Will It Take To Improve Care For Chronic IllnessDocument3 pages(1998) Chronic Disease Management What Will It Take To Improve Care For Chronic IllnessDaniel MeloNo ratings yet
- A Model For The Implementation of Lean Improvements in Healthcare Environments As Applied in A Primary Care CenterDocument30 pagesA Model For The Implementation of Lean Improvements in Healthcare Environments As Applied in A Primary Care CenterJhonattan AntonNo ratings yet
- Providing Higher Value Care Through Population Health Management: What Is The Radiologist 'S Role?Document2 pagesProviding Higher Value Care Through Population Health Management: What Is The Radiologist 'S Role?Camilo SotomayorNo ratings yet
- Principles of The Patient-Centered Medical Home and Preventive Services DeliveryDocument9 pagesPrinciples of The Patient-Centered Medical Home and Preventive Services DeliverysudartoNo ratings yet
- 34 - 2013-14 Examples of Annual ObjectivesDocument5 pages34 - 2013-14 Examples of Annual ObjectivesMichael BatesNo ratings yet
- Intensive Care Unit Quality Improvement: A "How-To" Guide For The Interdisciplinary TeamDocument8 pagesIntensive Care Unit Quality Improvement: A "How-To" Guide For The Interdisciplinary TeamJosé Ignacio Cárdenas VásquezNo ratings yet
- NSQHS Standards Fact Sheet Standard 2Document2 pagesNSQHS Standards Fact Sheet Standard 2Annette LowryNo ratings yet
- Ward Round Report 0Document47 pagesWard Round Report 0Teena VajiNo ratings yet
- Cost Minimization of A Telehomecare Prog PDFDocument10 pagesCost Minimization of A Telehomecare Prog PDFRirin AptNo ratings yet
- HealthcareTransformers ValueBasedHealthcareDocument30 pagesHealthcareTransformers ValueBasedHealthcareamiraNo ratings yet
- Hex 21 41Document16 pagesHex 21 41fadedoyinNo ratings yet
- Case Study 1Document4 pagesCase Study 1languha NgatiNo ratings yet
- Planning and Designing Endocrinology ServicesDocument18 pagesPlanning and Designing Endocrinology ServicesAjul PNo ratings yet
- Evidence For Person-Centred Care in Chronic Wound Care: A Systematic Review and Recommendations For PracticeDocument24 pagesEvidence For Person-Centred Care in Chronic Wound Care: A Systematic Review and Recommendations For Practiceananda khairulNo ratings yet
- Quality and Outcomes Framework - What Have We Learnt?Document4 pagesQuality and Outcomes Framework - What Have We Learnt?Ana PaolaNo ratings yet
- Total Quality Management in Europe (Health Care)Document6 pagesTotal Quality Management in Europe (Health Care)nikki_ellaNo ratings yet
- Health Care Provider and Patient Preparedness ForDocument10 pagesHealth Care Provider and Patient Preparedness ForTJ LapuzNo ratings yet
- Effectiveness and Safety of Asynchronous Telemedicine Consultations in General Practice: A Systematic ReviewDocument13 pagesEffectiveness and Safety of Asynchronous Telemedicine Consultations in General Practice: A Systematic ReviewiboroniNo ratings yet
- JCI Whitepaper Cpgs Closing The GapDocument12 pagesJCI Whitepaper Cpgs Closing The GapMathilda UllyNo ratings yet
- Jope 38 SDocument6 pagesJope 38 SRhyka AchmadNo ratings yet
- Systems-Basedpracticein Burncare: Prevention, Management, and Economic Impact of Health Care-Associated InfectionsDocument8 pagesSystems-Basedpracticein Burncare: Prevention, Management, and Economic Impact of Health Care-Associated InfectionsanjarwatiNo ratings yet
- Atow 502 00Document9 pagesAtow 502 00hnzzn2bymdNo ratings yet
- Çevirilecek MetinDocument2 pagesÇevirilecek MetinSoner AkımalNo ratings yet
- A 2020 Vision of Patient CenteredDocument13 pagesA 2020 Vision of Patient CenteredElya Amaliia100% (1)
- Optimal EngDocument11 pagesOptimal EngIRENE ORTIZ LOPEZNo ratings yet
- Common Sense Approach To Managing SepsisDocument12 pagesCommon Sense Approach To Managing SepsiszepedrocorreiaNo ratings yet
- Experience of Long Term Life (CKD)Document15 pagesExperience of Long Term Life (CKD)Ririn Muthia ZukhraNo ratings yet
- BreatheDocument10 pagesBreathehealthcareisiNo ratings yet
- The Tender Process: Journal of Wound Care September 2012Document15 pagesThe Tender Process: Journal of Wound Care September 2012Le Thi Anh TuyetNo ratings yet
- Eiu Health System Preparedness FinalDocument63 pagesEiu Health System Preparedness FinalFamilia En AcNo ratings yet
- Characteristics of Case Management in Primary Care PDFDocument11 pagesCharacteristics of Case Management in Primary Care PDFCamila AlmeidaNo ratings yet
- Reiss Sandborn 2015 Role of Psychosocial CareDocument6 pagesReiss Sandborn 2015 Role of Psychosocial CareAgata AgniNo ratings yet
- s6 Clinical HandoverDocument26 pagess6 Clinical HandoverirenediahjNo ratings yet
- Health Care Professionals' Experiences and Perspectives On Using Telehealth For Home-Based Palliative Care: Protocol For A Scoping ReviewDocument7 pagesHealth Care Professionals' Experiences and Perspectives On Using Telehealth For Home-Based Palliative Care: Protocol For A Scoping Reviewshaza ameliaNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- Comprehensive Care Coordination for Chronically Ill AdultsFrom EverandComprehensive Care Coordination for Chronically Ill AdultsCheryl SchraederNo ratings yet
- of E-Aushadi FinalDocument48 pagesof E-Aushadi Finalv_ratNo ratings yet
- Case Demand Measurement and Forecasting Block-2 Ch.4Document3 pagesCase Demand Measurement and Forecasting Block-2 Ch.4v_ratNo ratings yet
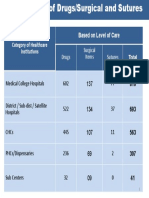
- Category of Healthcare Institutions Based On Level of Care: Drugs Surgical Items SuturesDocument1 pageCategory of Healthcare Institutions Based On Level of Care: Drugs Surgical Items Suturesv_ratNo ratings yet
- Inv. Mgt. Procurement & DistributionDocument78 pagesInv. Mgt. Procurement & Distributionv_ratNo ratings yet
- Drugs Store Management: Dr. Nirmal GurbaniDocument94 pagesDrugs Store Management: Dr. Nirmal Gurbaniv_ratNo ratings yet
- Access To Quality Medicines: Rajasthan Model: "Reaching The Unreached"Document7 pagesAccess To Quality Medicines: Rajasthan Model: "Reaching The Unreached"v_ratNo ratings yet
- Quantification of Health Commodities - RMNCH SupplementDocument173 pagesQuantification of Health Commodities - RMNCH Supplementv_ratNo ratings yet
- UNFPA RFQ QA Framework - Low - V11Document32 pagesUNFPA RFQ QA Framework - Low - V11v_ratNo ratings yet
- Day 4 - ReliabilityDocument11 pagesDay 4 - Reliabilityv_ratNo ratings yet
- A Strategic Essential in Healthcare Systems OutsourcingDocument22 pagesA Strategic Essential in Healthcare Systems Outsourcingv_ratNo ratings yet
- Day 8 Inventory ManagementDocument56 pagesDay 8 Inventory Managementv_ratNo ratings yet
- Day 2 - Equipment Preventive MaintenanceDocument29 pagesDay 2 - Equipment Preventive Maintenancev_ratNo ratings yet
- The Case-Study Approach: Lucy GilsonDocument74 pagesThe Case-Study Approach: Lucy Gilsonv_ratNo ratings yet
- Day 3 - Equipment Disposal, Audit, T&DDocument35 pagesDay 3 - Equipment Disposal, Audit, T&Dv_ratNo ratings yet
- Day 1 - Equipment-Mohan-1Document22 pagesDay 1 - Equipment-Mohan-1v_ratNo ratings yet
- Day 4 - CQI in Stores ManagementDocument8 pagesDay 4 - CQI in Stores Managementv_ratNo ratings yet
- Patient Engagement in Research: A Systematic Review: Researcharticle Open AccessDocument9 pagesPatient Engagement in Research: A Systematic Review: Researcharticle Open Accessv_ratNo ratings yet
- Logistics Management Information Systems (LMIS)Document25 pagesLogistics Management Information Systems (LMIS)v_ratNo ratings yet
- Introduction To Epidemiology: Cohort StudiesDocument32 pagesIntroduction To Epidemiology: Cohort Studiesv_ratNo ratings yet
- Patient Engagement Planning Checklist: Planning Component Key Questions To ConsiderDocument2 pagesPatient Engagement Planning Checklist: Planning Component Key Questions To Considerv_ratNo ratings yet
- Assessment of Patient Engagement With A Mobile Application Among Service Members in TransitionDocument9 pagesAssessment of Patient Engagement With A Mobile Application Among Service Members in Transitionv_ratNo ratings yet
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument9 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribev_ratNo ratings yet
- WLP - Q4 - Health 7 - Week 4Document8 pagesWLP - Q4 - Health 7 - Week 4Gladys GutierrezNo ratings yet
- Sarker Maruf - Final DraftDocument6 pagesSarker Maruf - Final DraftSarker MarufNo ratings yet
- Nitrat Levophed: Rumus ..... Cc/jamDocument8 pagesNitrat Levophed: Rumus ..... Cc/jamRufiahNo ratings yet
- STARCEF Cefixime 100 MG 200 MG Dry SyrupDocument1 pageSTARCEF Cefixime 100 MG 200 MG Dry SyrupAndri FauzanNo ratings yet
- Hypoglycemia (DR Fatimah) PDFDocument23 pagesHypoglycemia (DR Fatimah) PDFriopratamasNo ratings yet
- A Nursing Case Study On EctopicPregnancy PDFDocument60 pagesA Nursing Case Study On EctopicPregnancy PDFSteffiNo ratings yet
- Denisa - 2 Exemplare - AN - F-VDocument93 pagesDenisa - 2 Exemplare - AN - F-VAdrian PetrosNo ratings yet
- Saliers V Walmart:Hy-VeeDocument43 pagesSaliers V Walmart:Hy-VeeUncoverDCNo ratings yet
- Hydrogen Peroxide TherapyDocument7 pagesHydrogen Peroxide Therapyrichardjoost100% (2)
- MBB and DR PG Data2kDocument143 pagesMBB and DR PG Data2kYogesh PalNo ratings yet
- Breast CNC PDFDocument16 pagesBreast CNC PDFmizart rnaNo ratings yet
- ResMed-AirSense-10-for Her PDFDocument44 pagesResMed-AirSense-10-for Her PDFOmiNo ratings yet
- Hypertensive Vascular DiseaseDocument5 pagesHypertensive Vascular DiseaseGenoMacaraanNo ratings yet
- Impact of Technology To A Healthy Lifestyle (Gaya Hidup Sihat) - Texting, Playing Games, Watching Movies, Social Media, Typing, ResearchDocument3 pagesImpact of Technology To A Healthy Lifestyle (Gaya Hidup Sihat) - Texting, Playing Games, Watching Movies, Social Media, Typing, ResearchSyahrilNo ratings yet
- D-KEFS Validity - An Update (Pearson Clinical UK, 2008)Document9 pagesD-KEFS Validity - An Update (Pearson Clinical UK, 2008)Anonymous tFZP10dVRUNo ratings yet
- Urinary - Tract - Infection 3Document35 pagesUrinary - Tract - Infection 3DEARY BERRYNo ratings yet
- How To Download Gordis Epidemiology E Book 6Th Edition Ebook PDF Ebook PDF Docx Kindle Full ChapterDocument36 pagesHow To Download Gordis Epidemiology E Book 6Th Edition Ebook PDF Ebook PDF Docx Kindle Full Chapterandrew.taylor131100% (34)
- Correlation of Procalcitonin Level With NLR in Patient With SIRSDocument1 pageCorrelation of Procalcitonin Level With NLR in Patient With SIRSNisa UcilNo ratings yet
- SRJI 3-4-2014 English Language Paperback Books in Acupuncture and Acupressure A 5-Year AnalysisDocument5 pagesSRJI 3-4-2014 English Language Paperback Books in Acupuncture and Acupressure A 5-Year AnalysisDr. Krishna N. SharmaNo ratings yet
- Postherpetic Neuralgia NerissaDocument18 pagesPostherpetic Neuralgia Nerissanerissa rahadianthiNo ratings yet
- Labor Epidural Analgesia With Severe ThrombocytopeniaDocument2 pagesLabor Epidural Analgesia With Severe Thrombocytopeniasand52525No ratings yet
- 412 Lecture 1 3 Introduction To PathogenesisDocument49 pages412 Lecture 1 3 Introduction To PathogenesisAnik Saha Toni 1912619643No ratings yet
- Factors Associated With Severe Malaria in Children Under Five Years of Age at Mbarara Regional Referral Hospital, UgandaDocument12 pagesFactors Associated With Severe Malaria in Children Under Five Years of Age at Mbarara Regional Referral Hospital, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Failures in FPDDocument30 pagesFailures in FPDMayank Aggarwal100% (1)
- 2017 - Curse of FluorosisDocument9 pages2017 - Curse of FluorosisjaynajNo ratings yet
- Oxylog 3000plus Guia Ajustes InicialesDocument3 pagesOxylog 3000plus Guia Ajustes InicialesFrancisco José Lencina SalarNo ratings yet