
Patient Engagement in Research: A Systematic Review: Researcharticle Open Access
Patient Engagement in Research: A Systematic Review: Researcharticle Open Access
You might also like
- Astm C 423Document12 pagesAstm C 423Abhinav AcharyaNo ratings yet
- Jabsco 15780-0000 Parts ListDocument2 pagesJabsco 15780-0000 Parts ListClarence Clar100% (1)
- Detailed Lesson Plan in English IV - COMPOUND SENTENCEDocument12 pagesDetailed Lesson Plan in English IV - COMPOUND SENTENCEMadhie Gre Dela Provi94% (16)
- Chapter 005Document9 pagesChapter 005dtheart2821100% (1)
- Marketing Research Chapter Case Block-2 Ch.5Document4 pagesMarketing Research Chapter Case Block-2 Ch.5v_rat0% (1)
- The Prevalence of Patient Engagement in Published Trials: A Systematic ReviewDocument9 pagesThe Prevalence of Patient Engagement in Published Trials: A Systematic ReviewmilananandNo ratings yet
- Quality Indicators For Primary Health Care A Systematic Literature ReviewDocument10 pagesQuality Indicators For Primary Health Care A Systematic Literature ReviewafdtygyhkNo ratings yet
- Framing A Research Question and Generating A Research HypothesisDocument6 pagesFraming A Research Question and Generating A Research HypothesisOluwajuwon AdenugbaNo ratings yet
- Researching HealthDocument18 pagesResearching Healthericmaina042No ratings yet
- Patient Safety Full ReportDocument40 pagesPatient Safety Full ReportYudi Ariesta Chandra100% (1)
- Writing The Proposal For A Qualitative Research Methodology ProjectDocument41 pagesWriting The Proposal For A Qualitative Research Methodology Projectrcaba100% (1)
- Evidence-Based Health Care in Nepal: The Importance of Systematic ReviewsDocument5 pagesEvidence-Based Health Care in Nepal: The Importance of Systematic ReviewsDudiNo ratings yet
- Conjoint in HEALTH ResearchDocument17 pagesConjoint in HEALTH ResearchDiana Tan May KimNo ratings yet
- Interprofessional Collaboration and Patient-Reported Outcomes in Inpatient Care: A Systematic ReviewDocument25 pagesInterprofessional Collaboration and Patient-Reported Outcomes in Inpatient Care: A Systematic ReviewkhairulhusnizaharuddinNo ratings yet
- Tyra Jackson Workshop Draft 2 Research PapeDocument13 pagesTyra Jackson Workshop Draft 2 Research Papeapi-457810629No ratings yet
- HHS Public Access: Medication Adherence Outcomes of 771 Intervention Trials: Systematic Review and Meta-AnalysisDocument21 pagesHHS Public Access: Medication Adherence Outcomes of 771 Intervention Trials: Systematic Review and Meta-Analysisdaniela NeculmanNo ratings yet
- s12961-018-0304-2Document15 pagess12961-018-0304-2LUISA FERNANDA OCHOA VILLEGASNo ratings yet
- Final DraftDocument32 pagesFinal DraftShibanta SarenNo ratings yet
- MMC 2Document5 pagesMMC 2Ashraf AlbhlaNo ratings yet
- Newsletter - July10 - Version01 4Document4 pagesNewsletter - July10 - Version01 4Reid BeelsNo ratings yet
- Research Proposal - Anu ShankerDocument14 pagesResearch Proposal - Anu ShankerAnu ShankarNo ratings yet
- Critical Appraisal of A Cross-Sectional Study On Environmental HealthDocument2 pagesCritical Appraisal of A Cross-Sectional Study On Environmental HealthFaza Nurul WardhaniNo ratings yet
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- The Integration of Primary Health Care Services A Systematic Literature ReviewDocument5 pagesThe Integration of Primary Health Care Services A Systematic Literature ReviewrdssibwgfNo ratings yet
- How To Prepare and Present La Evidencia A ConsumidoresDocument39 pagesHow To Prepare and Present La Evidencia A ConsumidoresogianneoNo ratings yet
- Reporting Guidelines For Implementation and Operational ResearchDocument7 pagesReporting Guidelines For Implementation and Operational ResearchDanNo ratings yet
- 2019 Bookmatter UsingNaturallyOccurringDataInQDocument20 pages2019 Bookmatter UsingNaturallyOccurringDataInQWAHYUHIDAYAT 2023058201No ratings yet
- Evidence-Based Public Health, by Ross C. Brownson, Elizabeth A. Baker, Terry L. Leet, Kathleen N. GillespieDocument3 pagesEvidence-Based Public Health, by Ross C. Brownson, Elizabeth A. Baker, Terry L. Leet, Kathleen N. GillespieheAdNo ratings yet
- Bridges, Hauber Et Al. 2011 - Conjoint Analysis Applications in Health-A PDFDocument11 pagesBridges, Hauber Et Al. 2011 - Conjoint Analysis Applications in Health-A PDFali rezaNo ratings yet
- 2013-Evidence Based Public HealthDocument15 pages2013-Evidence Based Public HealthEric Yesaya TanNo ratings yet
- The Role of Social Media in Enhancing Clinical TriDocument15 pagesThe Role of Social Media in Enhancing Clinical TriManjit SinghNo ratings yet
- PDF Public Health Research Methods Greg Guest Ebook Full ChapterDocument53 pagesPDF Public Health Research Methods Greg Guest Ebook Full Chapterdavid.muterspaw637100% (1)
- Pico, Picos, SpiderDocument10 pagesPico, Picos, SpiderramneekNo ratings yet
- Developing A Framework: Nursing ResearchDocument10 pagesDeveloping A Framework: Nursing Researchbombillode13No ratings yet
- Best Practices For Mixed Methods ResearchDocument39 pagesBest Practices For Mixed Methods Researchscribd104444No ratings yet
- Rs 3Document11 pagesRs 3Eshan ShahNo ratings yet
- s12910 020 00538 7Document11 pagess12910 020 00538 7Paz GonzálezNo ratings yet
- What Are Patients Expectations of Orthodontic TreDocument9 pagesWhat Are Patients Expectations of Orthodontic TreAly OsmanNo ratings yet
- Reena Review1Document19 pagesReena Review1Yeshwanth SesettyNo ratings yet
- Freeman Et Al 2018 Open Dialogue A Review of The EvidenceDocument14 pagesFreeman Et Al 2018 Open Dialogue A Review of The Evidenceapartamentos.sintraNo ratings yet
- Research in Health and Social Care - EditedDocument8 pagesResearch in Health and Social Care - EditedJannat ButtNo ratings yet
- jvp160174 RevisedCIOMSInternationalEthicalGuidelinesDocument2 pagesjvp160174 RevisedCIOMSInternationalEthicalGuidelinesZubair Mahmood KamalNo ratings yet
- Brainsci 10 00688 v2Document23 pagesBrainsci 10 00688 v2alehagernNo ratings yet
- 2014 Isaacs Overviewof QRMfor PHreseasrchersDocument7 pages2014 Isaacs Overviewof QRMfor PHreseasrchersShubham SharmaNo ratings yet
- BMC Health Services Research: Describing The Impact of Health Research: A Research Impact FrameworkDocument18 pagesBMC Health Services Research: Describing The Impact of Health Research: A Research Impact FrameworkDaniela HernandezNo ratings yet
- Add 2Document15 pagesAdd 2diana.alyNo ratings yet
- Barriers and Facilitators To Evidence-Use in Program Management - A Systematic Review of LiteratureDocument24 pagesBarriers and Facilitators To Evidence-Use in Program Management - A Systematic Review of Literaturetiago alvesNo ratings yet
- Chapter 3 STEM 11 4 Group 1Document7 pagesChapter 3 STEM 11 4 Group 1Christianzzz CalibsNo ratings yet
- 48 FullDocument6 pages48 FullFuraya FuisaNo ratings yet
- Impact of Social Media On Nurses Service Delivery - EditedDocument14 pagesImpact of Social Media On Nurses Service Delivery - EditedMaina PeterNo ratings yet
- The Effectiveness of Interventions To Improve Laboratory Requesting Patterns Among Primary Care Physicians: A Systematic ReviewDocument13 pagesThe Effectiveness of Interventions To Improve Laboratory Requesting Patterns Among Primary Care Physicians: A Systematic ReviewGNo ratings yet
- Smo Journal TaskDocument3 pagesSmo Journal TaskaaNo ratings yet
- Policy and Practice Impacts of Applied Research A Case Study Analysis of The New South Wales Health PromotiDocument15 pagesPolicy and Practice Impacts of Applied Research A Case Study Analysis of The New South Wales Health PromotiMauro Rojas ZúñigaNo ratings yet
- ABOELELA, S. Et Al. Defining Interdisciplinary ResearchDocument18 pagesABOELELA, S. Et Al. Defining Interdisciplinary ResearchdanielmvsouzaNo ratings yet
- The Relationship Between Characteristics of Context and Research Utilization in A Pediatric SettingDocument10 pagesThe Relationship Between Characteristics of Context and Research Utilization in A Pediatric SettingReynaldi Esa RamadhanNo ratings yet
- Genomic Research Biobanking Incidental FindingsDocument6 pagesGenomic Research Biobanking Incidental FindingsJulius Caesar ColladoNo ratings yet
- Early Discharge Hospital at Home As Alternative To Routine Hospital Care For Older People: A Systematic Review and Meta AnalysisDocument15 pagesEarly Discharge Hospital at Home As Alternative To Routine Hospital Care For Older People: A Systematic Review and Meta Analysissoy_humanaNo ratings yet
- tmpF56 TMPDocument3 pagestmpF56 TMPFrontiers0% (1)
- Benchmark Evidence BasedDocument11 pagesBenchmark Evidence BasedPeterNo ratings yet
- Qualitative Research in Epidemiology: March 2012Document23 pagesQualitative Research in Epidemiology: March 2012Husain PanggiNo ratings yet
- PublicDocument12 pagesPublicJayapriya jayaramanNo ratings yet
- Systematic Literature Review EpidemiologyDocument6 pagesSystematic Literature Review Epidemiologyc5qx9hq5100% (1)
- Ethics, Qualitative And Quantitative Methods In Public Health ResearchFrom EverandEthics, Qualitative And Quantitative Methods In Public Health ResearchNo ratings yet
- Case Demand Measurement and Forecasting Block-2 Ch.4Document3 pagesCase Demand Measurement and Forecasting Block-2 Ch.4v_ratNo ratings yet
- Quantification of Health Commodities - RMNCH SupplementDocument173 pagesQuantification of Health Commodities - RMNCH Supplementv_ratNo ratings yet
- of E-Aushadi FinalDocument48 pagesof E-Aushadi Finalv_ratNo ratings yet
- Access To Quality Medicines: Rajasthan Model: "Reaching The Unreached"Document7 pagesAccess To Quality Medicines: Rajasthan Model: "Reaching The Unreached"v_ratNo ratings yet
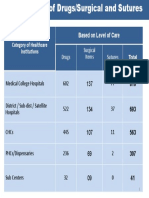
- Category of Healthcare Institutions Based On Level of Care: Drugs Surgical Items SuturesDocument1 pageCategory of Healthcare Institutions Based On Level of Care: Drugs Surgical Items Suturesv_ratNo ratings yet
- Drugs Store Management: Dr. Nirmal GurbaniDocument94 pagesDrugs Store Management: Dr. Nirmal Gurbaniv_ratNo ratings yet
- UNFPA RFQ QA Framework - Low - V11Document32 pagesUNFPA RFQ QA Framework - Low - V11v_ratNo ratings yet
- Inv. Mgt. Procurement & DistributionDocument78 pagesInv. Mgt. Procurement & Distributionv_ratNo ratings yet
- Day 8 Inventory ManagementDocument56 pagesDay 8 Inventory Managementv_ratNo ratings yet
- Day 4 - ReliabilityDocument11 pagesDay 4 - Reliabilityv_ratNo ratings yet
- A Strategic Essential in Healthcare Systems OutsourcingDocument22 pagesA Strategic Essential in Healthcare Systems Outsourcingv_ratNo ratings yet
- Day 2 - Equipment Preventive MaintenanceDocument29 pagesDay 2 - Equipment Preventive Maintenancev_ratNo ratings yet
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument9 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribev_ratNo ratings yet
- Day 3 - Equipment Disposal, Audit, T&DDocument35 pagesDay 3 - Equipment Disposal, Audit, T&Dv_ratNo ratings yet
- Logistics Management Information Systems (LMIS)Document25 pagesLogistics Management Information Systems (LMIS)v_ratNo ratings yet
- The Case-Study Approach: Lucy GilsonDocument74 pagesThe Case-Study Approach: Lucy Gilsonv_ratNo ratings yet
- Day 4 - CQI in Stores ManagementDocument8 pagesDay 4 - CQI in Stores Managementv_ratNo ratings yet
- Introduction To Epidemiology: Cohort StudiesDocument32 pagesIntroduction To Epidemiology: Cohort Studiesv_ratNo ratings yet
- Day 1 - Equipment-Mohan-1Document22 pagesDay 1 - Equipment-Mohan-1v_ratNo ratings yet
- Assessment of Patient Engagement With A Mobile Application Among Service Members in TransitionDocument9 pagesAssessment of Patient Engagement With A Mobile Application Among Service Members in Transitionv_ratNo ratings yet
- Patient Engagement Planning Checklist: Planning Component Key Questions To ConsiderDocument2 pagesPatient Engagement Planning Checklist: Planning Component Key Questions To Considerv_ratNo ratings yet
- Stable Fixed Points of Card Trick FunctionsDocument10 pagesStable Fixed Points of Card Trick FunctionsDerekNo ratings yet
- Exercises in RussianDocument270 pagesExercises in RussiansuzzixxNo ratings yet
- Chroma Bidirectional DC Power Supply Model 62000D SeriesDocument12 pagesChroma Bidirectional DC Power Supply Model 62000D SeriesaboofazilNo ratings yet
- Parent Involvement in Education: Kathleen Cotton and Karen Reed WikelundDocument17 pagesParent Involvement in Education: Kathleen Cotton and Karen Reed WikelundMohsin khaliqNo ratings yet
- September 23, Infer The Purpose of The Poem Listened ToDocument4 pagesSeptember 23, Infer The Purpose of The Poem Listened ToLouelle GonzalesNo ratings yet
- XXX (Topic) 好处影响1 相反好处 2. 你⾃自⼰己的观点,后⾯面会展开的Document3 pagesXXX (Topic) 好处影响1 相反好处 2. 你⾃自⼰己的观点,后⾯面会展开的Miyou KwanNo ratings yet
- Panasonic TH-P42C10M, S, T, K, DDocument122 pagesPanasonic TH-P42C10M, S, T, K, DEliel PinheiroNo ratings yet
- Optimal Design of Low-Cost and Reliable Hybrid Renewable Energy System Considering Grid BlackoutsDocument7 pagesOptimal Design of Low-Cost and Reliable Hybrid Renewable Energy System Considering Grid BlackoutsNelson Andres Entralgo MaldonadoNo ratings yet
- 115 Ballard Tommelein 2021 LPS Benchmark 2020 2Document125 pages115 Ballard Tommelein 2021 LPS Benchmark 2020 2ATDNo ratings yet
- MAD Practical 6Document15 pagesMAD Practical 6DIVYESH PATELNo ratings yet
- Building 7Document1 pageBuilding 7Arshad AlamNo ratings yet
- Dungeon 190Document77 pagesDungeon 190Helmous100% (4)
- Jadwal Pertandingan Liga Inggris 2009-2010Document11 pagesJadwal Pertandingan Liga Inggris 2009-2010Adjie SatryoNo ratings yet
- Taylor Swift LyricsDocument2 pagesTaylor Swift LyricsElsie DomeNo ratings yet
- Quiz For Western Lit.Document25 pagesQuiz For Western Lit.donnie4workingNo ratings yet
- Simulation and ModulationDocument89 pagesSimulation and ModulationGuruKPO67% (6)
- Chapter 1 Peanut Growing and HarvestingDocument18 pagesChapter 1 Peanut Growing and HarvestingKapil BhattNo ratings yet
- Company Profile For ICB TechnimontDocument4 pagesCompany Profile For ICB TechnimontShankarMukherjeeNo ratings yet
- Name:: Nyoman Gede Abhyasa Class: X Mipa 2 Absent: 25 AnswersDocument2 pagesName:: Nyoman Gede Abhyasa Class: X Mipa 2 Absent: 25 AnswersRetrify - Random ContentNo ratings yet
- How To Download A Windows 10 ISO File - PCWorldDocument3 pagesHow To Download A Windows 10 ISO File - PCWorldRajeev BatraNo ratings yet
- Muac MunichaccDocument24 pagesMuac MunichaccDelavillièreNo ratings yet
- Fs Tco Battery Diesel Delivery Trucks Jun2022Document3 pagesFs Tco Battery Diesel Delivery Trucks Jun2022The International Council on Clean TransportationNo ratings yet
- Physical Pendulum - Angular SHM - Solved ProblemsDocument7 pagesPhysical Pendulum - Angular SHM - Solved ProblemsHomayoon GeramifarNo ratings yet
- Dezvoltare Sustenabila in Zonele RuraleDocument20 pagesDezvoltare Sustenabila in Zonele RuraleAdrian BuțaNo ratings yet
- HG-G9 Module 7 RTP PDFDocument10 pagesHG-G9 Module 7 RTP PDFDaniel Robert BuccatNo ratings yet
- ACCA P5 Question 2 June 2013 QaDocument4 pagesACCA P5 Question 2 June 2013 QaFarhan AlchiNo ratings yet
- MC&OB Unit 4Document17 pagesMC&OB Unit 4Tanya MalviyaNo ratings yet















































































































Download as pdf or txt
You might also like
- Astm C 423Document12 pagesAstm C 423Abhinav AcharyaNo ratings yet
- Jabsco 15780-0000 Parts ListDocument2 pagesJabsco 15780-0000 Parts ListClarence Clar100% (1)
- Detailed Lesson Plan in English IV - COMPOUND SENTENCEDocument12 pagesDetailed Lesson Plan in English IV - COMPOUND SENTENCEMadhie Gre Dela Provi94% (16)
- Chapter 005Document9 pagesChapter 005dtheart2821100% (1)
- Marketing Research Chapter Case Block-2 Ch.5Document4 pagesMarketing Research Chapter Case Block-2 Ch.5v_rat0% (1)
- The Prevalence of Patient Engagement in Published Trials: A Systematic ReviewDocument9 pagesThe Prevalence of Patient Engagement in Published Trials: A Systematic ReviewmilananandNo ratings yet
- Quality Indicators For Primary Health Care A Systematic Literature ReviewDocument10 pagesQuality Indicators For Primary Health Care A Systematic Literature ReviewafdtygyhkNo ratings yet
- Framing A Research Question and Generating A Research HypothesisDocument6 pagesFraming A Research Question and Generating A Research HypothesisOluwajuwon AdenugbaNo ratings yet
- Researching HealthDocument18 pagesResearching Healthericmaina042No ratings yet
- Patient Safety Full ReportDocument40 pagesPatient Safety Full ReportYudi Ariesta Chandra100% (1)
- Writing The Proposal For A Qualitative Research Methodology ProjectDocument41 pagesWriting The Proposal For A Qualitative Research Methodology Projectrcaba100% (1)
- Evidence-Based Health Care in Nepal: The Importance of Systematic ReviewsDocument5 pagesEvidence-Based Health Care in Nepal: The Importance of Systematic ReviewsDudiNo ratings yet
- Conjoint in HEALTH ResearchDocument17 pagesConjoint in HEALTH ResearchDiana Tan May KimNo ratings yet
- Interprofessional Collaboration and Patient-Reported Outcomes in Inpatient Care: A Systematic ReviewDocument25 pagesInterprofessional Collaboration and Patient-Reported Outcomes in Inpatient Care: A Systematic ReviewkhairulhusnizaharuddinNo ratings yet
- Tyra Jackson Workshop Draft 2 Research PapeDocument13 pagesTyra Jackson Workshop Draft 2 Research Papeapi-457810629No ratings yet
- HHS Public Access: Medication Adherence Outcomes of 771 Intervention Trials: Systematic Review and Meta-AnalysisDocument21 pagesHHS Public Access: Medication Adherence Outcomes of 771 Intervention Trials: Systematic Review and Meta-Analysisdaniela NeculmanNo ratings yet
- s12961-018-0304-2Document15 pagess12961-018-0304-2LUISA FERNANDA OCHOA VILLEGASNo ratings yet
- Final DraftDocument32 pagesFinal DraftShibanta SarenNo ratings yet
- MMC 2Document5 pagesMMC 2Ashraf AlbhlaNo ratings yet
- Newsletter - July10 - Version01 4Document4 pagesNewsletter - July10 - Version01 4Reid BeelsNo ratings yet
- Research Proposal - Anu ShankerDocument14 pagesResearch Proposal - Anu ShankerAnu ShankarNo ratings yet
- Critical Appraisal of A Cross-Sectional Study On Environmental HealthDocument2 pagesCritical Appraisal of A Cross-Sectional Study On Environmental HealthFaza Nurul WardhaniNo ratings yet
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- The Integration of Primary Health Care Services A Systematic Literature ReviewDocument5 pagesThe Integration of Primary Health Care Services A Systematic Literature ReviewrdssibwgfNo ratings yet
- How To Prepare and Present La Evidencia A ConsumidoresDocument39 pagesHow To Prepare and Present La Evidencia A ConsumidoresogianneoNo ratings yet
- Reporting Guidelines For Implementation and Operational ResearchDocument7 pagesReporting Guidelines For Implementation and Operational ResearchDanNo ratings yet
- 2019 Bookmatter UsingNaturallyOccurringDataInQDocument20 pages2019 Bookmatter UsingNaturallyOccurringDataInQWAHYUHIDAYAT 2023058201No ratings yet
- Evidence-Based Public Health, by Ross C. Brownson, Elizabeth A. Baker, Terry L. Leet, Kathleen N. GillespieDocument3 pagesEvidence-Based Public Health, by Ross C. Brownson, Elizabeth A. Baker, Terry L. Leet, Kathleen N. GillespieheAdNo ratings yet
- Bridges, Hauber Et Al. 2011 - Conjoint Analysis Applications in Health-A PDFDocument11 pagesBridges, Hauber Et Al. 2011 - Conjoint Analysis Applications in Health-A PDFali rezaNo ratings yet
- 2013-Evidence Based Public HealthDocument15 pages2013-Evidence Based Public HealthEric Yesaya TanNo ratings yet
- The Role of Social Media in Enhancing Clinical TriDocument15 pagesThe Role of Social Media in Enhancing Clinical TriManjit SinghNo ratings yet
- PDF Public Health Research Methods Greg Guest Ebook Full ChapterDocument53 pagesPDF Public Health Research Methods Greg Guest Ebook Full Chapterdavid.muterspaw637100% (1)
- Pico, Picos, SpiderDocument10 pagesPico, Picos, SpiderramneekNo ratings yet
- Developing A Framework: Nursing ResearchDocument10 pagesDeveloping A Framework: Nursing Researchbombillode13No ratings yet
- Best Practices For Mixed Methods ResearchDocument39 pagesBest Practices For Mixed Methods Researchscribd104444No ratings yet
- Rs 3Document11 pagesRs 3Eshan ShahNo ratings yet
- s12910 020 00538 7Document11 pagess12910 020 00538 7Paz GonzálezNo ratings yet
- What Are Patients Expectations of Orthodontic TreDocument9 pagesWhat Are Patients Expectations of Orthodontic TreAly OsmanNo ratings yet
- Reena Review1Document19 pagesReena Review1Yeshwanth SesettyNo ratings yet
- Freeman Et Al 2018 Open Dialogue A Review of The EvidenceDocument14 pagesFreeman Et Al 2018 Open Dialogue A Review of The Evidenceapartamentos.sintraNo ratings yet
- Research in Health and Social Care - EditedDocument8 pagesResearch in Health and Social Care - EditedJannat ButtNo ratings yet
- jvp160174 RevisedCIOMSInternationalEthicalGuidelinesDocument2 pagesjvp160174 RevisedCIOMSInternationalEthicalGuidelinesZubair Mahmood KamalNo ratings yet
- Brainsci 10 00688 v2Document23 pagesBrainsci 10 00688 v2alehagernNo ratings yet
- 2014 Isaacs Overviewof QRMfor PHreseasrchersDocument7 pages2014 Isaacs Overviewof QRMfor PHreseasrchersShubham SharmaNo ratings yet
- BMC Health Services Research: Describing The Impact of Health Research: A Research Impact FrameworkDocument18 pagesBMC Health Services Research: Describing The Impact of Health Research: A Research Impact FrameworkDaniela HernandezNo ratings yet
- Add 2Document15 pagesAdd 2diana.alyNo ratings yet
- Barriers and Facilitators To Evidence-Use in Program Management - A Systematic Review of LiteratureDocument24 pagesBarriers and Facilitators To Evidence-Use in Program Management - A Systematic Review of Literaturetiago alvesNo ratings yet
- Chapter 3 STEM 11 4 Group 1Document7 pagesChapter 3 STEM 11 4 Group 1Christianzzz CalibsNo ratings yet
- 48 FullDocument6 pages48 FullFuraya FuisaNo ratings yet
- Impact of Social Media On Nurses Service Delivery - EditedDocument14 pagesImpact of Social Media On Nurses Service Delivery - EditedMaina PeterNo ratings yet
- The Effectiveness of Interventions To Improve Laboratory Requesting Patterns Among Primary Care Physicians: A Systematic ReviewDocument13 pagesThe Effectiveness of Interventions To Improve Laboratory Requesting Patterns Among Primary Care Physicians: A Systematic ReviewGNo ratings yet
- Smo Journal TaskDocument3 pagesSmo Journal TaskaaNo ratings yet
- Policy and Practice Impacts of Applied Research A Case Study Analysis of The New South Wales Health PromotiDocument15 pagesPolicy and Practice Impacts of Applied Research A Case Study Analysis of The New South Wales Health PromotiMauro Rojas ZúñigaNo ratings yet
- ABOELELA, S. Et Al. Defining Interdisciplinary ResearchDocument18 pagesABOELELA, S. Et Al. Defining Interdisciplinary ResearchdanielmvsouzaNo ratings yet
- The Relationship Between Characteristics of Context and Research Utilization in A Pediatric SettingDocument10 pagesThe Relationship Between Characteristics of Context and Research Utilization in A Pediatric SettingReynaldi Esa RamadhanNo ratings yet
- Genomic Research Biobanking Incidental FindingsDocument6 pagesGenomic Research Biobanking Incidental FindingsJulius Caesar ColladoNo ratings yet
- Early Discharge Hospital at Home As Alternative To Routine Hospital Care For Older People: A Systematic Review and Meta AnalysisDocument15 pagesEarly Discharge Hospital at Home As Alternative To Routine Hospital Care For Older People: A Systematic Review and Meta Analysissoy_humanaNo ratings yet
- tmpF56 TMPDocument3 pagestmpF56 TMPFrontiers0% (1)
- Benchmark Evidence BasedDocument11 pagesBenchmark Evidence BasedPeterNo ratings yet
- Qualitative Research in Epidemiology: March 2012Document23 pagesQualitative Research in Epidemiology: March 2012Husain PanggiNo ratings yet
- PublicDocument12 pagesPublicJayapriya jayaramanNo ratings yet
- Systematic Literature Review EpidemiologyDocument6 pagesSystematic Literature Review Epidemiologyc5qx9hq5100% (1)
- Ethics, Qualitative And Quantitative Methods In Public Health ResearchFrom EverandEthics, Qualitative And Quantitative Methods In Public Health ResearchNo ratings yet
- Case Demand Measurement and Forecasting Block-2 Ch.4Document3 pagesCase Demand Measurement and Forecasting Block-2 Ch.4v_ratNo ratings yet
- Quantification of Health Commodities - RMNCH SupplementDocument173 pagesQuantification of Health Commodities - RMNCH Supplementv_ratNo ratings yet
- of E-Aushadi FinalDocument48 pagesof E-Aushadi Finalv_ratNo ratings yet
- Access To Quality Medicines: Rajasthan Model: "Reaching The Unreached"Document7 pagesAccess To Quality Medicines: Rajasthan Model: "Reaching The Unreached"v_ratNo ratings yet
- Category of Healthcare Institutions Based On Level of Care: Drugs Surgical Items SuturesDocument1 pageCategory of Healthcare Institutions Based On Level of Care: Drugs Surgical Items Suturesv_ratNo ratings yet
- Drugs Store Management: Dr. Nirmal GurbaniDocument94 pagesDrugs Store Management: Dr. Nirmal Gurbaniv_ratNo ratings yet
- UNFPA RFQ QA Framework - Low - V11Document32 pagesUNFPA RFQ QA Framework - Low - V11v_ratNo ratings yet
- Inv. Mgt. Procurement & DistributionDocument78 pagesInv. Mgt. Procurement & Distributionv_ratNo ratings yet
- Day 8 Inventory ManagementDocument56 pagesDay 8 Inventory Managementv_ratNo ratings yet
- Day 4 - ReliabilityDocument11 pagesDay 4 - Reliabilityv_ratNo ratings yet
- A Strategic Essential in Healthcare Systems OutsourcingDocument22 pagesA Strategic Essential in Healthcare Systems Outsourcingv_ratNo ratings yet
- Day 2 - Equipment Preventive MaintenanceDocument29 pagesDay 2 - Equipment Preventive Maintenancev_ratNo ratings yet
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument9 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribev_ratNo ratings yet
- Day 3 - Equipment Disposal, Audit, T&DDocument35 pagesDay 3 - Equipment Disposal, Audit, T&Dv_ratNo ratings yet
- Logistics Management Information Systems (LMIS)Document25 pagesLogistics Management Information Systems (LMIS)v_ratNo ratings yet
- The Case-Study Approach: Lucy GilsonDocument74 pagesThe Case-Study Approach: Lucy Gilsonv_ratNo ratings yet
- Day 4 - CQI in Stores ManagementDocument8 pagesDay 4 - CQI in Stores Managementv_ratNo ratings yet
- Introduction To Epidemiology: Cohort StudiesDocument32 pagesIntroduction To Epidemiology: Cohort Studiesv_ratNo ratings yet
- Day 1 - Equipment-Mohan-1Document22 pagesDay 1 - Equipment-Mohan-1v_ratNo ratings yet
- Assessment of Patient Engagement With A Mobile Application Among Service Members in TransitionDocument9 pagesAssessment of Patient Engagement With A Mobile Application Among Service Members in Transitionv_ratNo ratings yet
- Patient Engagement Planning Checklist: Planning Component Key Questions To ConsiderDocument2 pagesPatient Engagement Planning Checklist: Planning Component Key Questions To Considerv_ratNo ratings yet
- Stable Fixed Points of Card Trick FunctionsDocument10 pagesStable Fixed Points of Card Trick FunctionsDerekNo ratings yet
- Exercises in RussianDocument270 pagesExercises in RussiansuzzixxNo ratings yet
- Chroma Bidirectional DC Power Supply Model 62000D SeriesDocument12 pagesChroma Bidirectional DC Power Supply Model 62000D SeriesaboofazilNo ratings yet
- Parent Involvement in Education: Kathleen Cotton and Karen Reed WikelundDocument17 pagesParent Involvement in Education: Kathleen Cotton and Karen Reed WikelundMohsin khaliqNo ratings yet
- September 23, Infer The Purpose of The Poem Listened ToDocument4 pagesSeptember 23, Infer The Purpose of The Poem Listened ToLouelle GonzalesNo ratings yet
- XXX (Topic) 好处影响1 相反好处 2. 你⾃自⼰己的观点,后⾯面会展开的Document3 pagesXXX (Topic) 好处影响1 相反好处 2. 你⾃自⼰己的观点,后⾯面会展开的Miyou KwanNo ratings yet
- Panasonic TH-P42C10M, S, T, K, DDocument122 pagesPanasonic TH-P42C10M, S, T, K, DEliel PinheiroNo ratings yet
- Optimal Design of Low-Cost and Reliable Hybrid Renewable Energy System Considering Grid BlackoutsDocument7 pagesOptimal Design of Low-Cost and Reliable Hybrid Renewable Energy System Considering Grid BlackoutsNelson Andres Entralgo MaldonadoNo ratings yet
- 115 Ballard Tommelein 2021 LPS Benchmark 2020 2Document125 pages115 Ballard Tommelein 2021 LPS Benchmark 2020 2ATDNo ratings yet
- MAD Practical 6Document15 pagesMAD Practical 6DIVYESH PATELNo ratings yet
- Building 7Document1 pageBuilding 7Arshad AlamNo ratings yet
- Dungeon 190Document77 pagesDungeon 190Helmous100% (4)
- Jadwal Pertandingan Liga Inggris 2009-2010Document11 pagesJadwal Pertandingan Liga Inggris 2009-2010Adjie SatryoNo ratings yet
- Taylor Swift LyricsDocument2 pagesTaylor Swift LyricsElsie DomeNo ratings yet
- Quiz For Western Lit.Document25 pagesQuiz For Western Lit.donnie4workingNo ratings yet
- Simulation and ModulationDocument89 pagesSimulation and ModulationGuruKPO67% (6)
- Chapter 1 Peanut Growing and HarvestingDocument18 pagesChapter 1 Peanut Growing and HarvestingKapil BhattNo ratings yet
- Company Profile For ICB TechnimontDocument4 pagesCompany Profile For ICB TechnimontShankarMukherjeeNo ratings yet
- Name:: Nyoman Gede Abhyasa Class: X Mipa 2 Absent: 25 AnswersDocument2 pagesName:: Nyoman Gede Abhyasa Class: X Mipa 2 Absent: 25 AnswersRetrify - Random ContentNo ratings yet
- How To Download A Windows 10 ISO File - PCWorldDocument3 pagesHow To Download A Windows 10 ISO File - PCWorldRajeev BatraNo ratings yet
- Muac MunichaccDocument24 pagesMuac MunichaccDelavillièreNo ratings yet
- Fs Tco Battery Diesel Delivery Trucks Jun2022Document3 pagesFs Tco Battery Diesel Delivery Trucks Jun2022The International Council on Clean TransportationNo ratings yet
- Physical Pendulum - Angular SHM - Solved ProblemsDocument7 pagesPhysical Pendulum - Angular SHM - Solved ProblemsHomayoon GeramifarNo ratings yet
- Dezvoltare Sustenabila in Zonele RuraleDocument20 pagesDezvoltare Sustenabila in Zonele RuraleAdrian BuțaNo ratings yet
- HG-G9 Module 7 RTP PDFDocument10 pagesHG-G9 Module 7 RTP PDFDaniel Robert BuccatNo ratings yet
- ACCA P5 Question 2 June 2013 QaDocument4 pagesACCA P5 Question 2 June 2013 QaFarhan AlchiNo ratings yet
- MC&OB Unit 4Document17 pagesMC&OB Unit 4Tanya MalviyaNo ratings yet