
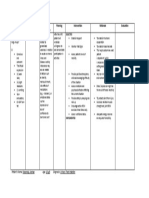
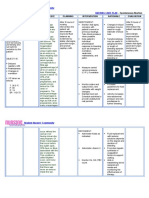
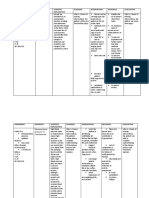
11NCP Ineffective Tissue Perfusion 2018 Revised 3.12.18
11NCP Ineffective Tissue Perfusion 2018 Revised 3.12.18
You might also like
- Contamination Control Strategy DevelopmentDocument75 pagesContamination Control Strategy DevelopmentArnaldo García100% (9)
- NCP For Subarachnoid HemorrhageDocument4 pagesNCP For Subarachnoid HemorrhageJoan Rose Rendon-Hung78% (18)
- NURSING-CARE-PLAN Breech PresentationDocument3 pagesNURSING-CARE-PLAN Breech PresentationGab83% (18)
- Nursing Care Plan (Bell's Palsy)Document3 pagesNursing Care Plan (Bell's Palsy)Yessamin Paith Roderos100% (3)
- Nursing Care Plan For CHFDocument7 pagesNursing Care Plan For CHFRosemarie Carpio100% (5)
- NCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Document1 pageNCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Carl Elexer Cuyugan Ano100% (6)
- Nursing Care Plan StrokeDocument2 pagesNursing Care Plan StrokeA HNo ratings yet
- NCP Act. IntoleranceDocument1 pageNCP Act. IntoleranceJanine Karla OrcaNo ratings yet
- The Minimally Conscious State: Definition and Diagnostic CriteriaDocument7 pagesThe Minimally Conscious State: Definition and Diagnostic CriteriadonnyawNo ratings yet
- Assessment Diagnosi S Inference Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosi S Inference Planning Intervention Rationale EvaluationSHARMAINE ANNE POLICIOS100% (1)
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDocument4 pagesKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNo ratings yet
- BPPV NCPDocument2 pagesBPPV NCPNiña Mae Marasigan67% (3)
- Risk For Acute Pain Related To Surgical IncisionDocument4 pagesRisk For Acute Pain Related To Surgical IncisionMia Grace Garcia100% (1)
- NCP PsychDocument7 pagesNCP PsychScarletNo ratings yet
- NCP - Tissue Perfusion (Cerebral)Document2 pagesNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- Altered Sensorium Batch 2016Document9 pagesAltered Sensorium Batch 2016Adriel PagariganNo ratings yet
- Nursing Care Plan Impaired CommunicationDocument3 pagesNursing Care Plan Impaired CommunicationRamiel ChristopherNo ratings yet
- Nueva Ecija University of Science and TechnologyDocument7 pagesNueva Ecija University of Science and TechnologyKym RonquilloNo ratings yet
- Nic IctpDocument2 pagesNic IctpRobby BanjarNo ratings yet
- Nursing Care Plan: Artery Blockage May BeDocument5 pagesNursing Care Plan: Artery Blockage May BeDienizs Labini TadenaNo ratings yet
- Cues Objective S Interventions Rationale Evaluatio NDocument2 pagesCues Objective S Interventions Rationale Evaluatio NJoehoney BarreraNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanMel Izhra N. MargateNo ratings yet
- Cues Nursing Diagnosis Goal & Objectives Nursing Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Goal & Objectives Nursing Intervention Rationale EvaluationJoanna DulongNo ratings yet
- NCP (Stroke)Document9 pagesNCP (Stroke)Claire M. AuditorNo ratings yet
- NCP CushingDocument4 pagesNCP CushingKatherine BautistaNo ratings yet
- Case Analysis: Neuro CaseDocument7 pagesCase Analysis: Neuro CaseKyle AndrewNo ratings yet
- Fluid Volume Excess Related To Decrease Glomerular Filtration Rate and Sodium RetentionDocument6 pagesFluid Volume Excess Related To Decrease Glomerular Filtration Rate and Sodium RetentionKristel Abe100% (1)
- Agn NCPDocument6 pagesAgn NCPJewel AnneNo ratings yet
- NCP Activity Intolerance (HTN Crisis)Document3 pagesNCP Activity Intolerance (HTN Crisis)Jenny AjocNo ratings yet
- NCP 2Document3 pagesNCP 2romelyn100% (1)
- AssessmentDocument3 pagesAssessmentaqualise101No ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- Nursing Care Plan AmebiasisDocument7 pagesNursing Care Plan AmebiasisCarl Simon CalingacionNo ratings yet
- Case Study 1 NCPDocument3 pagesCase Study 1 NCPJayson SamonteNo ratings yet
- Name: Garanchon, Ceyan Peaches BSN2DDocument3 pagesName: Garanchon, Ceyan Peaches BSN2DXeyanNo ratings yet
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- 3 Ncp'sDocument3 pages3 Ncp'sJohn Michael EstevesNo ratings yet
- Revised NCP 1-3Document6 pagesRevised NCP 1-3MarcieNo ratings yet
- Assessment Diagnosis Goal Intervention EvaluationDocument1 pageAssessment Diagnosis Goal Intervention EvaluationBree BalanaNo ratings yet
- ND2Document1 pageND2Janah PagayNo ratings yet
- Med Ward NCP Week 3Document4 pagesMed Ward NCP Week 3Ghianx Carlox PioquintoxNo ratings yet
- Heiz NCPDocument2 pagesHeiz NCPheizNo ratings yet
- Sleep DeprivationDocument2 pagesSleep DeprivationJulie Ann Gamboa EwicanNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- NCP Acute PainDocument3 pagesNCP Acute PainBasema HashhashNo ratings yet
- Nursing Care Plan: Obstetrics and Gynecology Nursing RotationDocument8 pagesNursing Care Plan: Obstetrics and Gynecology Nursing RotationMary Justine Nuyad-AfricaNo ratings yet
- Nursing Care Plan No.1: NewbornDocument5 pagesNursing Care Plan No.1: NewbornIrene Grace BalcuevaNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- General Malvar ST., Davao CityDocument5 pagesGeneral Malvar ST., Davao CityKhim BalcitaNo ratings yet
- Prenatal Nursing Care PlansDocument25 pagesPrenatal Nursing Care PlansRijane Tabonoc OmlangNo ratings yet
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- SElf Directed RT Manic Excitement NCP BM DISORDERDocument2 pagesSElf Directed RT Manic Excitement NCP BM DISORDEREden Marie FranciscoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermMicaela CrisostomoNo ratings yet
- Disturbed Visual Sensory Perception Related: Nursing Care PlanDocument3 pagesDisturbed Visual Sensory Perception Related: Nursing Care PlanMae Therese B. MAGNONo ratings yet
- Copy of NCP Format)Document4 pagesCopy of NCP Format)shai raNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention EvaluationPrince Mark BadilloNo ratings yet
- Norbe COMFORT MEASURESDocument10 pagesNorbe COMFORT MEASURESMarlo Dañez NorbeNo ratings yet
- Relapse Prevention Counseling Workbook: A Step-by-Step Guide to Sustainable Recovery: Holistic approaches to recovery and relapse preventionFrom EverandRelapse Prevention Counseling Workbook: A Step-by-Step Guide to Sustainable Recovery: Holistic approaches to recovery and relapse preventionNo ratings yet
- Polyvagal Blueprint: The 7-Step Program for Harnessing Your Vagal Power to Transform Anxiety, Trauma, and RelationshipsFrom EverandPolyvagal Blueprint: The 7-Step Program for Harnessing Your Vagal Power to Transform Anxiety, Trauma, and RelationshipsNo ratings yet
- Benign Paroxysmal Positional Vertigo Demystified: Doctor’s Secret GuideFrom EverandBenign Paroxysmal Positional Vertigo Demystified: Doctor’s Secret GuideNo ratings yet
- Mark Vincent San Gabriel, RN: Educational BackgroundDocument3 pagesMark Vincent San Gabriel, RN: Educational BackgroundAubrey SungaNo ratings yet
- Ways To Achieve Mental Well BeingDocument3 pagesWays To Achieve Mental Well BeingAubrey SungaNo ratings yet
- Addressing The Stigma On Mental IllnessDocument2 pagesAddressing The Stigma On Mental IllnessAubrey SungaNo ratings yet
- Exercise 3 - Neuro, Cranial NervesDocument3 pagesExercise 3 - Neuro, Cranial NervesAubrey SungaNo ratings yet
- Exercise 1-Management of Client With Ear Problem Review: Anatomy & PhysiologyDocument2 pagesExercise 1-Management of Client With Ear Problem Review: Anatomy & PhysiologyAubrey SungaNo ratings yet
- NC 116 Exercise 2-EYES Assessment 1. Label The Following PartsDocument3 pagesNC 116 Exercise 2-EYES Assessment 1. Label The Following PartsAubrey SungaNo ratings yet
- Health Care EthicsDocument12 pagesHealth Care EthicsAubrey SungaNo ratings yet
- Coping Area Justification: Rating/ Point On The ScaleDocument1 pageCoping Area Justification: Rating/ Point On The ScaleAubrey SungaNo ratings yet
- Clien With CMLDocument4 pagesClien With CMLAubrey SungaNo ratings yet
- Hygiene Is The Science of Health and Its: Types of Hygienic CareDocument12 pagesHygiene Is The Science of Health and Its: Types of Hygienic CareAubrey SungaNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey Sunga100% (1)
- Nursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationDocument5 pagesNursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationAubrey SungaNo ratings yet
- Is The Set of Life-Sustaining Chemical Reactions in OrganismDocument3 pagesIs The Set of Life-Sustaining Chemical Reactions in OrganismAubrey SungaNo ratings yet
- Computation of The ProblemsDocument1 pageComputation of The ProblemsAubrey SungaNo ratings yet
- The Lymphatic & Immune Systems: Thymus Spleen Lymph Nodes Lymphatic VesselDocument30 pagesThe Lymphatic & Immune Systems: Thymus Spleen Lymph Nodes Lymphatic VesselAubrey SungaNo ratings yet
- Journal Notes CN107 SlabDocument1 pageJournal Notes CN107 SlabAubrey SungaNo ratings yet
- I. Biographical Data: F. PatternDocument2 pagesI. Biographical Data: F. PatternAubrey SungaNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey SungaNo ratings yet
- Date Cues Subjective/Objective Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeDocument2 pagesDate Cues Subjective/Objective Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeAubrey SungaNo ratings yet
- Health History AND Physical Assessment: Sunga Jean Aubrey S.ADocument4 pagesHealth History AND Physical Assessment: Sunga Jean Aubrey S.AAubrey SungaNo ratings yet
- Implementing The Proper Selection, Collection, Transport, and Processing of Appropriate Clinical SpecimensDocument3 pagesImplementing The Proper Selection, Collection, Transport, and Processing of Appropriate Clinical SpecimensAubrey SungaNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey SungaNo ratings yet
- Date Cues Subjective/Objectiv e Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeDocument1 pageDate Cues Subjective/Objectiv e Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeAubrey SungaNo ratings yet
- Conceptual Framework - Scope and Delimitation of The StudyDocument3 pagesConceptual Framework - Scope and Delimitation of The StudyAubrey SungaNo ratings yet
- Low Calorie DietDocument2 pagesLow Calorie DietAubrey SungaNo ratings yet
- Initial Database Record: A. Family Structure, Characteristics and DynamicsDocument9 pagesInitial Database Record: A. Family Structure, Characteristics and DynamicsAubrey SungaNo ratings yet
- Diphtheria ReportDocument13 pagesDiphtheria ReportAubrey SungaNo ratings yet
- Children of Alcoholics - wp1 Final DraftDocument6 pagesChildren of Alcoholics - wp1 Final Draftapi-425081999No ratings yet
- Terrier Football Strength and Conditioning Summer ManualDocument28 pagesTerrier Football Strength and Conditioning Summer Manualcoachowens68100% (1)
- Project On Anatomy of Foot & SkinDocument29 pagesProject On Anatomy of Foot & SkinShahbaj KhanNo ratings yet
- Monitoring and Evaluation ME PlanDocument12 pagesMonitoring and Evaluation ME PlanMirAfghan GhulamiPoorNo ratings yet
- SEAFDEC/AQD Institutional Repository (SAIR) : This Document Is Downloaded At: 2013-07-02 07:11:51 CSTDocument53 pagesSEAFDEC/AQD Institutional Repository (SAIR) : This Document Is Downloaded At: 2013-07-02 07:11:51 CSTKarl KiwisNo ratings yet
- Demographic Profile of The Respondents by Age and GenderDocument6 pagesDemographic Profile of The Respondents by Age and GenderBabelinoBedroGetesJr.No ratings yet
- Pharma Chapter 1- 7 融合 PDFDocument396 pagesPharma Chapter 1- 7 融合 PDF爾雅雷No ratings yet
- Communication MidwiferyDocument11 pagesCommunication Midwiferygraham20No ratings yet
- GolfDocument28 pagesGolfCharles MercadoNo ratings yet
- Fluid Volume Deficient Cues SDocument6 pagesFluid Volume Deficient Cues SjedrickNo ratings yet
- Kat, Smarties, Nesquik, Stouffer's, Vittel, and MaggiDocument23 pagesKat, Smarties, Nesquik, Stouffer's, Vittel, and MaggiSaadNo ratings yet
- A Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFDocument5 pagesA Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFhahahapsuNo ratings yet
- Modified Radical Mastectomy - 3B ABLOGDocument45 pagesModified Radical Mastectomy - 3B ABLOGDafny CzarinaNo ratings yet
- Occupational Health Assessment Questionnaire Version 2 February 2010Document3 pagesOccupational Health Assessment Questionnaire Version 2 February 2010Cherry Mañibo100% (1)
- Guiding For HospitalDocument14 pagesGuiding For HospitalAnkit Bhatia100% (1)
- How Much Time Can You Keep A Butt Plug in - BuscaDocument1 pageHow Much Time Can You Keep A Butt Plug in - BuscamaniizuNo ratings yet
- BLOOD PRESSURE Vs HEART RATE From American Heart AssociationDocument2 pagesBLOOD PRESSURE Vs HEART RATE From American Heart AssociationSyima MnnNo ratings yet
- PNLE Nursing Practice V (RN Pedia)Document10 pagesPNLE Nursing Practice V (RN Pedia)Ma. Dominique L. FacultadNo ratings yet
- 2014 Bookmatter ContemporarySocio-CulturalAndPDocument21 pages2014 Bookmatter ContemporarySocio-CulturalAndPYvette TolentinoNo ratings yet
- Tata AIG Medi Care 82932b277aDocument30 pagesTata AIG Medi Care 82932b277aChandra SekaranNo ratings yet
- Writing Paper 2 Part 1 H 9Document3 pagesWriting Paper 2 Part 1 H 9Punky BrewsterNo ratings yet
- Obesity AssessmentDocument34 pagesObesity AssessmentMahmoud ShabbanNo ratings yet
- Mini Clinical EvaluationDocument2 pagesMini Clinical Evaluationdileepa RathnayakaNo ratings yet
- Nabl 126Document31 pagesNabl 126Gazal GuptaNo ratings yet
- IndianJPsychiatry 2019 61 4 423 262795Document2 pagesIndianJPsychiatry 2019 61 4 423 262795gion.nandNo ratings yet
- 10 Overtraining SyndromeDocument15 pages10 Overtraining SyndromeTasniiem KhmbataNo ratings yet
- Shauna - Shames - Barriers - and - Solutions 5Document13 pagesShauna - Shames - Barriers - and - Solutions 5ANKUR CHOUDHARYNo ratings yet
- Culpeper Herbal TherapeuticsDocument9 pagesCulpeper Herbal Therapeuticsjoel_tetardNo ratings yet
- VO Guidlines For LLB 3 Year CET - 2022 - FinalDocument16 pagesVO Guidlines For LLB 3 Year CET - 2022 - FinalRAJESHWAR SINGHNo ratings yet
















































































































Download as docx, pdf, or txt
You might also like
- Contamination Control Strategy DevelopmentDocument75 pagesContamination Control Strategy DevelopmentArnaldo García100% (9)
- NCP For Subarachnoid HemorrhageDocument4 pagesNCP For Subarachnoid HemorrhageJoan Rose Rendon-Hung78% (18)
- NURSING-CARE-PLAN Breech PresentationDocument3 pagesNURSING-CARE-PLAN Breech PresentationGab83% (18)
- Nursing Care Plan (Bell's Palsy)Document3 pagesNursing Care Plan (Bell's Palsy)Yessamin Paith Roderos100% (3)
- Nursing Care Plan For CHFDocument7 pagesNursing Care Plan For CHFRosemarie Carpio100% (5)
- NCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Document1 pageNCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Carl Elexer Cuyugan Ano100% (6)
- Nursing Care Plan StrokeDocument2 pagesNursing Care Plan StrokeA HNo ratings yet
- NCP Act. IntoleranceDocument1 pageNCP Act. IntoleranceJanine Karla OrcaNo ratings yet
- The Minimally Conscious State: Definition and Diagnostic CriteriaDocument7 pagesThe Minimally Conscious State: Definition and Diagnostic CriteriadonnyawNo ratings yet
- Assessment Diagnosi S Inference Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosi S Inference Planning Intervention Rationale EvaluationSHARMAINE ANNE POLICIOS100% (1)
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDocument4 pagesKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNo ratings yet
- BPPV NCPDocument2 pagesBPPV NCPNiña Mae Marasigan67% (3)
- Risk For Acute Pain Related To Surgical IncisionDocument4 pagesRisk For Acute Pain Related To Surgical IncisionMia Grace Garcia100% (1)
- NCP PsychDocument7 pagesNCP PsychScarletNo ratings yet
- NCP - Tissue Perfusion (Cerebral)Document2 pagesNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- Altered Sensorium Batch 2016Document9 pagesAltered Sensorium Batch 2016Adriel PagariganNo ratings yet
- Nursing Care Plan Impaired CommunicationDocument3 pagesNursing Care Plan Impaired CommunicationRamiel ChristopherNo ratings yet
- Nueva Ecija University of Science and TechnologyDocument7 pagesNueva Ecija University of Science and TechnologyKym RonquilloNo ratings yet
- Nic IctpDocument2 pagesNic IctpRobby BanjarNo ratings yet
- Nursing Care Plan: Artery Blockage May BeDocument5 pagesNursing Care Plan: Artery Blockage May BeDienizs Labini TadenaNo ratings yet
- Cues Objective S Interventions Rationale Evaluatio NDocument2 pagesCues Objective S Interventions Rationale Evaluatio NJoehoney BarreraNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanMel Izhra N. MargateNo ratings yet
- Cues Nursing Diagnosis Goal & Objectives Nursing Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Goal & Objectives Nursing Intervention Rationale EvaluationJoanna DulongNo ratings yet
- NCP (Stroke)Document9 pagesNCP (Stroke)Claire M. AuditorNo ratings yet
- NCP CushingDocument4 pagesNCP CushingKatherine BautistaNo ratings yet
- Case Analysis: Neuro CaseDocument7 pagesCase Analysis: Neuro CaseKyle AndrewNo ratings yet
- Fluid Volume Excess Related To Decrease Glomerular Filtration Rate and Sodium RetentionDocument6 pagesFluid Volume Excess Related To Decrease Glomerular Filtration Rate and Sodium RetentionKristel Abe100% (1)
- Agn NCPDocument6 pagesAgn NCPJewel AnneNo ratings yet
- NCP Activity Intolerance (HTN Crisis)Document3 pagesNCP Activity Intolerance (HTN Crisis)Jenny AjocNo ratings yet
- NCP 2Document3 pagesNCP 2romelyn100% (1)
- AssessmentDocument3 pagesAssessmentaqualise101No ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- Nursing Care Plan AmebiasisDocument7 pagesNursing Care Plan AmebiasisCarl Simon CalingacionNo ratings yet
- Case Study 1 NCPDocument3 pagesCase Study 1 NCPJayson SamonteNo ratings yet
- Name: Garanchon, Ceyan Peaches BSN2DDocument3 pagesName: Garanchon, Ceyan Peaches BSN2DXeyanNo ratings yet
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- 3 Ncp'sDocument3 pages3 Ncp'sJohn Michael EstevesNo ratings yet
- Revised NCP 1-3Document6 pagesRevised NCP 1-3MarcieNo ratings yet
- Assessment Diagnosis Goal Intervention EvaluationDocument1 pageAssessment Diagnosis Goal Intervention EvaluationBree BalanaNo ratings yet
- ND2Document1 pageND2Janah PagayNo ratings yet
- Med Ward NCP Week 3Document4 pagesMed Ward NCP Week 3Ghianx Carlox PioquintoxNo ratings yet
- Heiz NCPDocument2 pagesHeiz NCPheizNo ratings yet
- Sleep DeprivationDocument2 pagesSleep DeprivationJulie Ann Gamboa EwicanNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- NCP Acute PainDocument3 pagesNCP Acute PainBasema HashhashNo ratings yet
- Nursing Care Plan: Obstetrics and Gynecology Nursing RotationDocument8 pagesNursing Care Plan: Obstetrics and Gynecology Nursing RotationMary Justine Nuyad-AfricaNo ratings yet
- Nursing Care Plan No.1: NewbornDocument5 pagesNursing Care Plan No.1: NewbornIrene Grace BalcuevaNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- General Malvar ST., Davao CityDocument5 pagesGeneral Malvar ST., Davao CityKhim BalcitaNo ratings yet
- Prenatal Nursing Care PlansDocument25 pagesPrenatal Nursing Care PlansRijane Tabonoc OmlangNo ratings yet
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- SElf Directed RT Manic Excitement NCP BM DISORDERDocument2 pagesSElf Directed RT Manic Excitement NCP BM DISORDEREden Marie FranciscoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermMicaela CrisostomoNo ratings yet
- Disturbed Visual Sensory Perception Related: Nursing Care PlanDocument3 pagesDisturbed Visual Sensory Perception Related: Nursing Care PlanMae Therese B. MAGNONo ratings yet
- Copy of NCP Format)Document4 pagesCopy of NCP Format)shai raNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention EvaluationPrince Mark BadilloNo ratings yet
- Norbe COMFORT MEASURESDocument10 pagesNorbe COMFORT MEASURESMarlo Dañez NorbeNo ratings yet
- Relapse Prevention Counseling Workbook: A Step-by-Step Guide to Sustainable Recovery: Holistic approaches to recovery and relapse preventionFrom EverandRelapse Prevention Counseling Workbook: A Step-by-Step Guide to Sustainable Recovery: Holistic approaches to recovery and relapse preventionNo ratings yet
- Polyvagal Blueprint: The 7-Step Program for Harnessing Your Vagal Power to Transform Anxiety, Trauma, and RelationshipsFrom EverandPolyvagal Blueprint: The 7-Step Program for Harnessing Your Vagal Power to Transform Anxiety, Trauma, and RelationshipsNo ratings yet
- Benign Paroxysmal Positional Vertigo Demystified: Doctor’s Secret GuideFrom EverandBenign Paroxysmal Positional Vertigo Demystified: Doctor’s Secret GuideNo ratings yet
- Mark Vincent San Gabriel, RN: Educational BackgroundDocument3 pagesMark Vincent San Gabriel, RN: Educational BackgroundAubrey SungaNo ratings yet
- Ways To Achieve Mental Well BeingDocument3 pagesWays To Achieve Mental Well BeingAubrey SungaNo ratings yet
- Addressing The Stigma On Mental IllnessDocument2 pagesAddressing The Stigma On Mental IllnessAubrey SungaNo ratings yet
- Exercise 3 - Neuro, Cranial NervesDocument3 pagesExercise 3 - Neuro, Cranial NervesAubrey SungaNo ratings yet
- Exercise 1-Management of Client With Ear Problem Review: Anatomy & PhysiologyDocument2 pagesExercise 1-Management of Client With Ear Problem Review: Anatomy & PhysiologyAubrey SungaNo ratings yet
- NC 116 Exercise 2-EYES Assessment 1. Label The Following PartsDocument3 pagesNC 116 Exercise 2-EYES Assessment 1. Label The Following PartsAubrey SungaNo ratings yet
- Health Care EthicsDocument12 pagesHealth Care EthicsAubrey SungaNo ratings yet
- Coping Area Justification: Rating/ Point On The ScaleDocument1 pageCoping Area Justification: Rating/ Point On The ScaleAubrey SungaNo ratings yet
- Clien With CMLDocument4 pagesClien With CMLAubrey SungaNo ratings yet
- Hygiene Is The Science of Health and Its: Types of Hygienic CareDocument12 pagesHygiene Is The Science of Health and Its: Types of Hygienic CareAubrey SungaNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey Sunga100% (1)
- Nursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationDocument5 pagesNursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationAubrey SungaNo ratings yet
- Is The Set of Life-Sustaining Chemical Reactions in OrganismDocument3 pagesIs The Set of Life-Sustaining Chemical Reactions in OrganismAubrey SungaNo ratings yet
- Computation of The ProblemsDocument1 pageComputation of The ProblemsAubrey SungaNo ratings yet
- The Lymphatic & Immune Systems: Thymus Spleen Lymph Nodes Lymphatic VesselDocument30 pagesThe Lymphatic & Immune Systems: Thymus Spleen Lymph Nodes Lymphatic VesselAubrey SungaNo ratings yet
- Journal Notes CN107 SlabDocument1 pageJournal Notes CN107 SlabAubrey SungaNo ratings yet
- I. Biographical Data: F. PatternDocument2 pagesI. Biographical Data: F. PatternAubrey SungaNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey SungaNo ratings yet
- Date Cues Subjective/Objective Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeDocument2 pagesDate Cues Subjective/Objective Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeAubrey SungaNo ratings yet
- Health History AND Physical Assessment: Sunga Jean Aubrey S.ADocument4 pagesHealth History AND Physical Assessment: Sunga Jean Aubrey S.AAubrey SungaNo ratings yet
- Implementing The Proper Selection, Collection, Transport, and Processing of Appropriate Clinical SpecimensDocument3 pagesImplementing The Proper Selection, Collection, Transport, and Processing of Appropriate Clinical SpecimensAubrey SungaNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey SungaNo ratings yet
- Date Cues Subjective/Objectiv e Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeDocument1 pageDate Cues Subjective/Objectiv e Nursing Diagnosis Nursing Objectives Nursing Intervention Rationale Expected OutcomeAubrey SungaNo ratings yet
- Conceptual Framework - Scope and Delimitation of The StudyDocument3 pagesConceptual Framework - Scope and Delimitation of The StudyAubrey SungaNo ratings yet
- Low Calorie DietDocument2 pagesLow Calorie DietAubrey SungaNo ratings yet
- Initial Database Record: A. Family Structure, Characteristics and DynamicsDocument9 pagesInitial Database Record: A. Family Structure, Characteristics and DynamicsAubrey SungaNo ratings yet
- Diphtheria ReportDocument13 pagesDiphtheria ReportAubrey SungaNo ratings yet
- Children of Alcoholics - wp1 Final DraftDocument6 pagesChildren of Alcoholics - wp1 Final Draftapi-425081999No ratings yet
- Terrier Football Strength and Conditioning Summer ManualDocument28 pagesTerrier Football Strength and Conditioning Summer Manualcoachowens68100% (1)
- Project On Anatomy of Foot & SkinDocument29 pagesProject On Anatomy of Foot & SkinShahbaj KhanNo ratings yet
- Monitoring and Evaluation ME PlanDocument12 pagesMonitoring and Evaluation ME PlanMirAfghan GhulamiPoorNo ratings yet
- SEAFDEC/AQD Institutional Repository (SAIR) : This Document Is Downloaded At: 2013-07-02 07:11:51 CSTDocument53 pagesSEAFDEC/AQD Institutional Repository (SAIR) : This Document Is Downloaded At: 2013-07-02 07:11:51 CSTKarl KiwisNo ratings yet
- Demographic Profile of The Respondents by Age and GenderDocument6 pagesDemographic Profile of The Respondents by Age and GenderBabelinoBedroGetesJr.No ratings yet
- Pharma Chapter 1- 7 融合 PDFDocument396 pagesPharma Chapter 1- 7 融合 PDF爾雅雷No ratings yet
- Communication MidwiferyDocument11 pagesCommunication Midwiferygraham20No ratings yet
- GolfDocument28 pagesGolfCharles MercadoNo ratings yet
- Fluid Volume Deficient Cues SDocument6 pagesFluid Volume Deficient Cues SjedrickNo ratings yet
- Kat, Smarties, Nesquik, Stouffer's, Vittel, and MaggiDocument23 pagesKat, Smarties, Nesquik, Stouffer's, Vittel, and MaggiSaadNo ratings yet
- A Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFDocument5 pagesA Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFhahahapsuNo ratings yet
- Modified Radical Mastectomy - 3B ABLOGDocument45 pagesModified Radical Mastectomy - 3B ABLOGDafny CzarinaNo ratings yet
- Occupational Health Assessment Questionnaire Version 2 February 2010Document3 pagesOccupational Health Assessment Questionnaire Version 2 February 2010Cherry Mañibo100% (1)
- Guiding For HospitalDocument14 pagesGuiding For HospitalAnkit Bhatia100% (1)
- How Much Time Can You Keep A Butt Plug in - BuscaDocument1 pageHow Much Time Can You Keep A Butt Plug in - BuscamaniizuNo ratings yet
- BLOOD PRESSURE Vs HEART RATE From American Heart AssociationDocument2 pagesBLOOD PRESSURE Vs HEART RATE From American Heart AssociationSyima MnnNo ratings yet
- PNLE Nursing Practice V (RN Pedia)Document10 pagesPNLE Nursing Practice V (RN Pedia)Ma. Dominique L. FacultadNo ratings yet
- 2014 Bookmatter ContemporarySocio-CulturalAndPDocument21 pages2014 Bookmatter ContemporarySocio-CulturalAndPYvette TolentinoNo ratings yet
- Tata AIG Medi Care 82932b277aDocument30 pagesTata AIG Medi Care 82932b277aChandra SekaranNo ratings yet
- Writing Paper 2 Part 1 H 9Document3 pagesWriting Paper 2 Part 1 H 9Punky BrewsterNo ratings yet
- Obesity AssessmentDocument34 pagesObesity AssessmentMahmoud ShabbanNo ratings yet
- Mini Clinical EvaluationDocument2 pagesMini Clinical Evaluationdileepa RathnayakaNo ratings yet
- Nabl 126Document31 pagesNabl 126Gazal GuptaNo ratings yet
- IndianJPsychiatry 2019 61 4 423 262795Document2 pagesIndianJPsychiatry 2019 61 4 423 262795gion.nandNo ratings yet
- 10 Overtraining SyndromeDocument15 pages10 Overtraining SyndromeTasniiem KhmbataNo ratings yet
- Shauna - Shames - Barriers - and - Solutions 5Document13 pagesShauna - Shames - Barriers - and - Solutions 5ANKUR CHOUDHARYNo ratings yet
- Culpeper Herbal TherapeuticsDocument9 pagesCulpeper Herbal Therapeuticsjoel_tetardNo ratings yet
- VO Guidlines For LLB 3 Year CET - 2022 - FinalDocument16 pagesVO Guidlines For LLB 3 Year CET - 2022 - FinalRAJESHWAR SINGHNo ratings yet