Download as pdf or txt
You might also like
- Multi Step CarcinogenesisDocument27 pagesMulti Step CarcinogenesisANSH RAIZADA 20BOE10026No ratings yet
- REPORTING CERVICAL CYTOLOGY, The Bethesda SystemDocument3 pagesREPORTING CERVICAL CYTOLOGY, The Bethesda SystemNgotelo FunwiNo ratings yet
- Diagnosis of TrypanosomiasisDocument82 pagesDiagnosis of TrypanosomiasisDrVijayata Choudhary100% (1)
- 3.3 BioMagnetismDocument24 pages3.3 BioMagnetismaa5949045100% (1)
- 18 - Flow Cytometry and Introduction To Molecular PathologyDocument11 pages18 - Flow Cytometry and Introduction To Molecular Pathologyhamadadodo7No ratings yet
- RGU and MCU PPT Final For 18.9.23, BsmmuDocument46 pagesRGU and MCU PPT Final For 18.9.23, BsmmuMd.AlauddinNo ratings yet
- Basic Physical Examination In: UrologyDocument55 pagesBasic Physical Examination In: Urologyradiaputri25No ratings yet
- Antinuclear Antibody TestDocument3 pagesAntinuclear Antibody TestElise Señadoza Aulmo-BarcenasNo ratings yet
- ROLE OF FNAC TESTIS IN MALE INFERTILITY by SpandanaDocument61 pagesROLE OF FNAC TESTIS IN MALE INFERTILITY by SpandanaDineshprakash GovindhrajNo ratings yet
- Thalamus Hypothalamus GajDocument55 pagesThalamus Hypothalamus GajMédecin Adrian TGNo ratings yet
- CSF LectureDocument58 pagesCSF Lectureshweta yadavNo ratings yet
- Graft RejectionDocument33 pagesGraft Rejectionasmaa100% (1)
- BIOL 243 Guided Practice 3 - Transport Flow Chart AssignmentDocument1 pageBIOL 243 Guided Practice 3 - Transport Flow Chart AssignmentReeseNo ratings yet
- An Introduction To Molecular Biology: Savannah Mwesigwa Adapted From Aala A. AbulfarajDocument25 pagesAn Introduction To Molecular Biology: Savannah Mwesigwa Adapted From Aala A. AbulfarajMwanja MosesNo ratings yet
- 4 Safe Transfusion Right Blood Right Patient Right Time and Right PlaceDocument11 pages4 Safe Transfusion Right Blood Right Patient Right Time and Right PlaceEtrya Wianda100% (1)
- Entamoeba HistoyticaDocument25 pagesEntamoeba HistoyticaUmar FarooqNo ratings yet
- Gel Electrophoresis: By: Group 4Document29 pagesGel Electrophoresis: By: Group 4Aika SantillanNo ratings yet
- NGS Catalog14Document18 pagesNGS Catalog14Muhd Faiz NasirNo ratings yet
- Introduction To Clinical RadiologyDocument38 pagesIntroduction To Clinical RadiologyMUBIRU SAMUEL EDWARDNo ratings yet
- Case Control Studies - byDocument21 pagesCase Control Studies - byapi-3761895No ratings yet
- CSF & Body FluidDocument42 pagesCSF & Body FluidlopaNo ratings yet
- PrinsDocument44 pagesPrinsPalagiri MadhuNo ratings yet
- Beer Lambert LawDocument27 pagesBeer Lambert LawJainendra JainNo ratings yet
- Fungal Infections in IcuDocument195 pagesFungal Infections in IcubhumikaNo ratings yet
- Cytogenetics: Chromosome Banding & Barr Body DR Charu Khosla, 24/4/20, 10.45-11.45 AmDocument90 pagesCytogenetics: Chromosome Banding & Barr Body DR Charu Khosla, 24/4/20, 10.45-11.45 Amsonal aranha100% (2)
- Spirochetes: Aashutosh Nama M.SC Microbiology Sem - 1 Dr. B Lal Institute of BiotechnologyDocument34 pagesSpirochetes: Aashutosh Nama M.SC Microbiology Sem - 1 Dr. B Lal Institute of Biotechnologyaashutosh namaNo ratings yet
- Unit XII: Recombinant DNA TechnologyDocument38 pagesUnit XII: Recombinant DNA TechnologyKlynt BasadreNo ratings yet
- Vulvar Conditions & Vaginal ConditionsDocument15 pagesVulvar Conditions & Vaginal ConditionsRohitNo ratings yet
- Cytology and Cytological TechniquesDocument29 pagesCytology and Cytological TechniquesNgotelo FunwiNo ratings yet
- Dermatitis Numularis and NeurodermatitisDocument22 pagesDermatitis Numularis and NeurodermatitisNura ReefaNo ratings yet
- Chemical Examination of UrineDocument13 pagesChemical Examination of UrinePam Fajardo100% (1)
- Lecture 1 - Introduction To HistopathologyDocument6 pagesLecture 1 - Introduction To Histopathologynessa nimoNo ratings yet
- The SickDocument5 pagesThe Sicknarendraverma6484No ratings yet
- Bioelectricity Quiz - BME 111Document3 pagesBioelectricity Quiz - BME 111nav4evrNo ratings yet
- Spectrophotometry. Principle and ApplicationsDocument11 pagesSpectrophotometry. Principle and Applicationsmdusman2010No ratings yet
- Oedema 2Document18 pagesOedema 2Duppala Sateesh KumarNo ratings yet
- Dosimetry: Film Badge DosimetersDocument3 pagesDosimetry: Film Badge DosimetersmahaNo ratings yet
- Radio Immuno As SayDocument35 pagesRadio Immuno As SayDawlat SalamaNo ratings yet
- Histopath Lec Lu51Document8 pagesHistopath Lec Lu51Wennethbelle M. CorpuzNo ratings yet
- Laboratory Diagnosis of Infectious Diseases GuidelineDocument100 pagesLaboratory Diagnosis of Infectious Diseases GuidelineGalo PinosNo ratings yet
- Steps in Tissue Processing For Paraffin Sections: Presented By: Analee Nicole RilleraDocument15 pagesSteps in Tissue Processing For Paraffin Sections: Presented By: Analee Nicole RilleraNico LokoNo ratings yet
- Dna and Rna Powerpoint 2Document46 pagesDna and Rna Powerpoint 2api-267309851No ratings yet
- Lumbar Puncture: Bagasin, Nester James S. Rodriguez, Lourdes Erika ADocument32 pagesLumbar Puncture: Bagasin, Nester James S. Rodriguez, Lourdes Erika ANdor BariboloNo ratings yet
- Molecular Chaperones ReportDocument47 pagesMolecular Chaperones ReportKristian Cada100% (1)
- Infection and Modes of TransmissionDocument14 pagesInfection and Modes of TransmissionLucky Radita Alma100% (1)
- PHM304: Microbiology and Parasitology: Week 2: Parasitic InfectionDocument36 pagesPHM304: Microbiology and Parasitology: Week 2: Parasitic InfectionIsabel PeraltaNo ratings yet
- Secondary ImmunodeficiencyDocument13 pagesSecondary ImmunodeficiencytanyagargNo ratings yet
- Medical para Health-1Document504 pagesMedical para Health-1Yordanos AsmareNo ratings yet
- Introduction To Tissue ProcessingDocument21 pagesIntroduction To Tissue ProcessingELIEZER MAYAPITNo ratings yet
- Signs in ObgyDocument2 pagesSigns in ObgyAnnapurna DangetiNo ratings yet
- Fine Needle Aspiration Cytology (FNAC) of GISTDocument7 pagesFine Needle Aspiration Cytology (FNAC) of GISTurfriendanshul100% (1)
- Urology Physical Examination For BUPSDocument22 pagesUrology Physical Examination For BUPSLuki ErtandriNo ratings yet
- SpirocheteDocument32 pagesSpirocheteSAYMABANUNo ratings yet
- Assignment On Forensic ScienceDocument11 pagesAssignment On Forensic ScienceRakib Hossain100% (1)
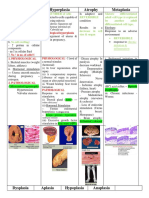
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- AUBF 02 - (Urine) Chemical PropertiesDocument11 pagesAUBF 02 - (Urine) Chemical PropertiesJustine Alexandrea RamirezNo ratings yet
- 4.1 Pathogenic FlagellatesDocument63 pages4.1 Pathogenic Flagellateskaartikey dubeNo ratings yet
- Para2021-3 2Document29 pagesPara2021-3 2Koko HashamNo ratings yet
- Atrial Flagellates: Romeo D. Dolar, JR MD Fpogs, Fpasmap, PapshpiDocument32 pagesAtrial Flagellates: Romeo D. Dolar, JR MD Fpogs, Fpasmap, PapshpiAlpana LaisomNo ratings yet
- Group1 ProtozoanMicrosDocument3 pagesGroup1 ProtozoanMicrosLuke Jovanni TAOCNo ratings yet
- Para Lec Trans PrelimDocument15 pagesPara Lec Trans PrelimSarah EugenioNo ratings yet
- Lecture 5 6 - Microscopy AND LUMINAL PROTOZOANDocument54 pagesLecture 5 6 - Microscopy AND LUMINAL PROTOZOANNida RidzuanNo ratings yet
- What Symbiote Are You?Document42 pagesWhat Symbiote Are You?Neil LopezNo ratings yet
- FLAGELLATESDocument34 pagesFLAGELLATESRediat GossayeNo ratings yet
- Para MCQDocument12 pagesPara MCQJames Blake100% (2)
- Dracunculus Medinensis and Filarial WormsDocument19 pagesDracunculus Medinensis and Filarial WormsAnastasiaNo ratings yet
- Flotation LabDocument17 pagesFlotation LabChinyere ObiNo ratings yet
- Giardiasis Case Karam Mizied 120180138Document13 pagesGiardiasis Case Karam Mizied 120180138Karam AtefNo ratings yet
- Phylum ProtozoaDocument65 pagesPhylum ProtozoaDan FabrosNo ratings yet
- Para MCQDocument2 pagesPara MCQMohamed HaridyNo ratings yet
- Giardia SisDocument3 pagesGiardia SisChrisMerellNo ratings yet
- ClinPara FlagellatesDocument10 pagesClinPara FlagellatesStephen YorNo ratings yet
- PARASITOLOGY (Quizlet)Document9 pagesPARASITOLOGY (Quizlet)Allyssa AniNo ratings yet
- Compilation of ParasitesDocument140 pagesCompilation of ParasitesChrissa Mae Tumaliuan CatindoyNo ratings yet
- Daftar Pustaka ParasitDocument11 pagesDaftar Pustaka Parasitresnha419No ratings yet
- Protozoan Infections Part 2Document19 pagesProtozoan Infections Part 2Medicine SWUNo ratings yet
- MCQ ParasitologyDocument11 pagesMCQ ParasitologyNida Ridzuan100% (1)
- Adam 2001. Biology of Giardia LambliaDocument29 pagesAdam 2001. Biology of Giardia Lambliaresnha419No ratings yet
- Eckhard Worch - Drinking Water Treatment - An Introduction-De Gruyter (2019)Document324 pagesEckhard Worch - Drinking Water Treatment - An Introduction-De Gruyter (2019)Ali MohieldinNo ratings yet
- Midterms - Clinical ParasitologyDocument19 pagesMidterms - Clinical ParasitologyJyne CatipayNo ratings yet
- Giardia LambliaDocument40 pagesGiardia LambliaKotilakshmanareddy TetaliNo ratings yet
- Study Guide of Medical Parasitology, Part 1. ProtozoologyDocument50 pagesStudy Guide of Medical Parasitology, Part 1. Protozoologymicrobehunter007No ratings yet
- PARA 11 Intro To ParasitologyDocument9 pagesPARA 11 Intro To ParasitologyArlene DaroNo ratings yet
- Giardia LambliaDocument4 pagesGiardia LambliaUzziel Galinea TolosaNo ratings yet
- Medical ParacitologyDocument83 pagesMedical ParacitologyariffdrNo ratings yet
- CHAPTER 5 ParasitologyyDocument35 pagesCHAPTER 5 ParasitologyyMerlpa May AlcardeNo ratings yet
- Giardiasis in Small AnimalsDocument6 pagesGiardiasis in Small AnimalsPad-ay Jasmin IrisNo ratings yet
- Parasitology: Prepared By: Charriz A. AmoyanDocument99 pagesParasitology: Prepared By: Charriz A. AmoyanRaphylyn EscalonaNo ratings yet
- Mdparas NotesDocument46 pagesMdparas Notesnamkimseo100% (1)