Download as pdf or txt
You might also like
- Inner Critic WorkbookDocument16 pagesInner Critic WorkbookAlice Paul100% (17)
- Neurotics Anonymous Test of Mental and Emotional HealthDocument2 pagesNeurotics Anonymous Test of Mental and Emotional Healthcraigt90% (10)
- Sleep 50 QuestionnaireDocument5 pagesSleep 50 QuestionnaireSónia Alves100% (1)
- California Motion To Quash Search Warrant, StalenessDocument10 pagesCalifornia Motion To Quash Search Warrant, Stalenessmatthew_whitten100% (2)
- 4 Steps Cognitive RestructuringDocument4 pages4 Steps Cognitive RestructuringshirleyxxxxNo ratings yet
- Anxiety Help: A 2 Page Worksheet For Finding Anxiety TriggersDocument3 pagesAnxiety Help: A 2 Page Worksheet For Finding Anxiety Triggersdrjanebolton100% (3)
- New Patient FormsDocument6 pagesNew Patient FormsPerformax Physical TherapyNo ratings yet
- Respondent Covid 19 MootDocument15 pagesRespondent Covid 19 MootBarsha PaulNo ratings yet
- 7 PolicereportDocument1 page7 Policereportapi-327470316No ratings yet
- Fear QuestionnaireDocument3 pagesFear QuestionnaireTrinidad Cortés LópezNo ratings yet
- Trauma Recover Workbook F110222 1Document64 pagesTrauma Recover Workbook F110222 1halaalansari5No ratings yet
- First TestDocument1 pageFirst Testkardasha :v MGNo ratings yet
- Research GRADE 11Document11 pagesResearch GRADE 11jonalyn lodorNo ratings yet
- Pacform PDFDocument7 pagesPacform PDFIngrid GabrielleNo ratings yet
- Tcu Psyform: Please Indicate How Much You AGREE or DISAGREE With Each StatementDocument2 pagesTcu Psyform: Please Indicate How Much You AGREE or DISAGREE With Each Statementmysteryvan1981No ratings yet
- Psychotherapy Assessment Checklist Follow Up FormDocument7 pagesPsychotherapy Assessment Checklist Follow Up FormGissel QuinteroNo ratings yet
- Stress AssessmentDocument3 pagesStress AssessmentYhed ZmadNo ratings yet
- Physical Assessment Form (Adult)Document7 pagesPhysical Assessment Form (Adult)Mart Juaresa YambaoNo ratings yet
- Releasing Emotional PainDocument6 pagesReleasing Emotional PainJano LunaNo ratings yet
- Health14 TR P 03 03Document1 pageHealth14 TR P 03 03Sarah BourgeoisNo ratings yet
- Name: Monica Chut B. Albofera Section: 12 - MATTHEW Personal Development Module 1: Activity 1Document5 pagesName: Monica Chut B. Albofera Section: 12 - MATTHEW Personal Development Module 1: Activity 1Monica chut AlboferaNo ratings yet
- 00 Instrument For PeaceDocument6 pages00 Instrument For PeaceAnca BaciuNo ratings yet
- DSM 5 PAC FormDocument7 pagesDSM 5 PAC FormGissel QuinteroNo ratings yet
- 2008SportsPhys FormDocument2 pages2008SportsPhys FormbbruntNo ratings yet
- 029 General SurgeryDocument4 pages029 General Surgeryعبدالله الرعويNo ratings yet
- Calm Box Tool Kit NewDocument16 pagesCalm Box Tool Kit NewSarah Shea GlassNo ratings yet
- Schizophrenia: I. IdentificationDocument3 pagesSchizophrenia: I. Identificationmyer pasandalanNo ratings yet
- Stress Signals Instructions: Take A Look at The Warning Signs of Stress Listed Below. WriteDocument2 pagesStress Signals Instructions: Take A Look at The Warning Signs of Stress Listed Below. WritePrincess VillanuevaNo ratings yet
- New Patient Paperwork (FINAL DRAFT)Document4 pagesNew Patient Paperwork (FINAL DRAFT)andrew_sokolNo ratings yet
- Express Your AngerDocument1 pageExpress Your AngerLyra May Manangan RefuerzoNo ratings yet
- Compassion FatigueDocument33 pagesCompassion FatigueDiane Celine SantianoNo ratings yet
- New ClassDocument1 pageNew Classapi-306485777No ratings yet
- Suicide Risk Asst ToolDocument3 pagesSuicide Risk Asst Toolrimpa29No ratings yet
- Polyclinic Medical Records HistoryDocument2 pagesPolyclinic Medical Records Historydevi ana ariesta bellaNo ratings yet
- My Personal Safety Plan WhiteDocument2 pagesMy Personal Safety Plan WhiteLesly N. MontielNo ratings yet
- Crucial Conversations PrimerDocument2 pagesCrucial Conversations PrimerGary PasseroNo ratings yet
- CH 4-5 TestDocument2 pagesCH 4-5 TestEyan OroscoNo ratings yet
- Assessment Form: Cebu Normal UniversityDocument8 pagesAssessment Form: Cebu Normal UniversityLauren JalandoniNo ratings yet
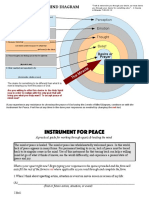
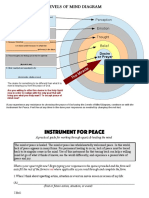
- Levels of Mind Diagram: Perception Emotion Thought BeliefDocument6 pagesLevels of Mind Diagram: Perception Emotion Thought BeliefVanessaBorgesNo ratings yet
- Mental Status ExamDocument3 pagesMental Status ExamvinodksahuNo ratings yet
- Dmpa 2 - Area InglesDocument5 pagesDmpa 2 - Area InglesUdad ManchegoNo ratings yet
- Headaches Residual Functional Capacity QuestionnaireDocument3 pagesHeadaches Residual Functional Capacity QuestionnaireDellComputer99No ratings yet
- Chapter 2. Test - Food & HealthDocument2 pagesChapter 2. Test - Food & HealthShavel KumarNo ratings yet
- Kathryn Seifert - Dancing With The Aardvark - A Guided Journal For Managing Stress-Electronic & Database Publishing, Inc. (2006)Document34 pagesKathryn Seifert - Dancing With The Aardvark - A Guided Journal For Managing Stress-Electronic & Database Publishing, Inc. (2006)edgtanz4No ratings yet
- Neuropsychology QuestionnaireDocument5 pagesNeuropsychology Questionnaireeva.mmNo ratings yet
- Causes and Effects of Depression To Teenagers and How They Overcome ItDocument3 pagesCauses and Effects of Depression To Teenagers and How They Overcome Itjonalyn lodorNo ratings yet
- CAE-UOE Part1Document4 pagesCAE-UOE Part1nikitsaNo ratings yet
- TraumainterviewDocument9 pagesTraumainterviewKathy RojasNo ratings yet
- 3.expressing FeelingsDocument6 pages3.expressing FeelingsSrínívas SrínuNo ratings yet
- Section 1: Epworth Sleepiness ScaleDocument3 pagesSection 1: Epworth Sleepiness ScaledwNo ratings yet
- PSS For StudentsDocument17 pagesPSS For StudentsJenefer AisoNo ratings yet
- Oe3bu6 p57 Writing SupportDocument8 pagesOe3bu6 p57 Writing SupportGabriel FungNo ratings yet
- Football Player Evaluation FormDocument1 pageFootball Player Evaluation FormAndohar PurbaNo ratings yet
- Introduce YourselfDocument2 pagesIntroduce YourselfPauli FerrariNo ratings yet
- Test Paper 4gradeDocument2 pagesTest Paper 4gradeNastiusha CaraimanNo ratings yet
- Science 1Document4 pagesScience 1karla mae kalaloNo ratings yet
- 101 Form 2 End Term 1 Exams ENGLISH QuestionsDocument9 pages101 Form 2 End Term 1 Exams ENGLISH Questionsedwinchirchir6130No ratings yet
- Final Exam 2Document2 pagesFinal Exam 2Nathalie MolinaNo ratings yet
- Suicide Risk Asst ToolDocument3 pagesSuicide Risk Asst ToolkasmiantoabadiNo ratings yet
- For Sts Unit 3 No 1 Grade 9 Teen Stress and PressureDocument2 pagesFor Sts Unit 3 No 1 Grade 9 Teen Stress and PressureAn NguyễnNo ratings yet
- What Is TrustDocument20 pagesWhat Is Trustcameron_ball_7No ratings yet
- Unit 7 ICA ChartsDocument5 pagesUnit 7 ICA Chartsnavyabearad2715No ratings yet
- An Intelligent and Strong Actor - Song Lyrics GeneratorDocument4 pagesAn Intelligent and Strong Actor - Song Lyrics GeneratorRui Jorge AbreuNo ratings yet
- Tirol - Mj.legal EthicsDocument10 pagesTirol - Mj.legal EthicsMark Jason S. TirolNo ratings yet
- Kidnapping and AbductionDocument22 pagesKidnapping and AbductionKhairul Iman100% (3)
- Spouses Zalamea vs. CADocument15 pagesSpouses Zalamea vs. CAAira Mae LayloNo ratings yet
- De La Paz v. L & J Development CoDocument2 pagesDe La Paz v. L & J Development CoNivra Lyn EmpialesNo ratings yet
- Motion To Cancel and Reset Hearing and Formal Entry of AppearanceDocument3 pagesMotion To Cancel and Reset Hearing and Formal Entry of AppearanceKalex KryptonNo ratings yet
- Free ConsentDocument54 pagesFree ConsentAnonymous cy5AUWGXwzNo ratings yet
- People Vs Aleman GR No. 181539 FactsDocument1 pagePeople Vs Aleman GR No. 181539 FactsJessette Amihope CASTORNo ratings yet
- BGC Boutique Menarco Tower SummaryDocument3 pagesBGC Boutique Menarco Tower SummaryJohnson SambranoNo ratings yet
- Module 5 - ContractsDocument65 pagesModule 5 - ContractsDeryl GalveNo ratings yet
- Government Contracts: Umakanth VarottilDocument16 pagesGovernment Contracts: Umakanth VarottilAadhitya NarayananNo ratings yet
- Zero No Tsukaima 7 - The Silver PentecostDocument186 pagesZero No Tsukaima 7 - The Silver PentecostCerberus Media DesignsNo ratings yet
- Mabeza v. NLRC, April 18, 1997Document12 pagesMabeza v. NLRC, April 18, 1997BREL GOSIMATNo ratings yet
- Civil Procedure - Udsm Manual 2002Document107 pagesCivil Procedure - Udsm Manual 2002habiye2013100% (1)
- Voice and Voice Therapy 9th Edition Boone Test BankDocument35 pagesVoice and Voice Therapy 9th Edition Boone Test Bankbrakemancullet.qzp7100% (30)
- Engagement LetterDocument2 pagesEngagement LetterCristopher ReyesNo ratings yet
- TC 28 RespondentDocument18 pagesTC 28 RespondentHimadri BadoniNo ratings yet
- No. ONGC/ER/CP/: MED/01 0 Office Order Dated 26th September, 2007Document5 pagesNo. ONGC/ER/CP/: MED/01 0 Office Order Dated 26th September, 2007MithunNo ratings yet
- The Game of Cricket Has A Known History Spanning From The 16th Century To The Present DayDocument12 pagesThe Game of Cricket Has A Known History Spanning From The 16th Century To The Present DayGaurav JaiswalNo ratings yet
- IPC Crime Against Women by Pragati DewanganDocument24 pagesIPC Crime Against Women by Pragati DewanganShubhamPatelNo ratings yet
- List of Presidents of The United States: President Term Began Term EndedDocument1 pageList of Presidents of The United States: President Term Began Term Endedmalaya tripathy100% (1)
- Appreciation On Autres Temps... (Edith Wharton) - by FELIDocument7 pagesAppreciation On Autres Temps... (Edith Wharton) - by FELIfelifire1No ratings yet
- His Plant TranslationDocument13 pagesHis Plant TranslationBig Zaman45No ratings yet
- U12 Asian Games SpeDocument29 pagesU12 Asian Games SpeheobilNo ratings yet
- East PakistanDocument3 pagesEast PakistanMohammad JamilNo ratings yet
- TM 9 1025 211 34Document697 pagesTM 9 1025 211 34Mark Ab100% (1)