Download as pdf or txt
You might also like
- Nakshatra Nadi Astrology - AstrogurukulDocument8 pagesNakshatra Nadi Astrology - AstrogurukulRakesh Soni60% (5)
- AJODO-2013 Claudino 143 6 799Document11 pagesAJODO-2013 Claudino 143 6 799player osamaNo ratings yet
- El 2011Document11 pagesEl 2011popsilviaizabellaNo ratings yet
- Fu 2016Document10 pagesFu 2016Soe San KyawNo ratings yet
- Alveolar Bone Grafting.Document58 pagesAlveolar Bone Grafting.Frederick Mars UntalanNo ratings yet
- Nelson 2008Document4 pagesNelson 2008Noi ZarkandyNo ratings yet
- Kim 2010Document11 pagesKim 2010popsilviaizabellaNo ratings yet
- First Premolar Extraction Effects On Upper Airway Dimension in Bimaxillary Proclination PatientsDocument7 pagesFirst Premolar Extraction Effects On Upper Airway Dimension in Bimaxillary Proclination PatientsJean-Philippe MercierNo ratings yet
- Airway Compartments Volume and Oxygen Saturation Changes After RapidDocument7 pagesAirway Compartments Volume and Oxygen Saturation Changes After Rapidkarengj952No ratings yet
- Three-Dimensional Analysis of The Airway With Cone-Beam Computed TomographyDocument9 pagesThree-Dimensional Analysis of The Airway With Cone-Beam Computed TomographySoe San KyawNo ratings yet
- Peng 2012Document7 pagesPeng 2012abhishekjha0082No ratings yet
- 11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The LiteratureDocument11 pages11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The Literaturekochikaghochi100% (1)
- FrankelDocument8 pagesFrankeldavid torresNo ratings yet
- 2017 AksuDocument7 pages2017 AksuR. Yair Delgado JaimesNo ratings yet
- DO in OSA PTDocument17 pagesDO in OSA PThammodihotmailcomNo ratings yet
- Respirador BucalDocument8 pagesRespirador Bucalyessenia armijosNo ratings yet
- Orientation of The Premaxilla in The Origin of Septal DeviationDocument5 pagesOrientation of The Premaxilla in The Origin of Septal Deviationnisrina hanifNo ratings yet
- Ucar 2011Document9 pagesUcar 2011dinaka samarathungaNo ratings yet
- Cleftlipandpalate Surgery:Anupdate Ofclinicaloutcomes ForprimaryrepairDocument16 pagesCleftlipandpalate Surgery:Anupdate Ofclinicaloutcomes ForprimaryrepairOrtodoncia UNAL 2020No ratings yet
- Milo Ro 2010Document12 pagesMilo Ro 2010abdullah özelNo ratings yet
- Coordes 2017Document21 pagesCoordes 2017nunisulastri1998No ratings yet
- Xu 2014Document8 pagesXu 2014Nadya Novia SariNo ratings yet
- Rme Efek AnakDocument10 pagesRme Efek AnakSiwi HadjarNo ratings yet
- Bimaxillary Dentoalveolar Protrusion Traits andDocument7 pagesBimaxillary Dentoalveolar Protrusion Traits andSAM PRASANTHNo ratings yet
- Gomez Et Al 2012Document12 pagesGomez Et Al 2012LAURA MARCELA BARRENECHE CALLENo ratings yet
- Lower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor FracturesDocument5 pagesLower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor Fracturesstoia_sebiNo ratings yet
- Effects of Maxillary Protraction and Fixed Appliance Therapy On The Pharyngeal AirwayDocument8 pagesEffects of Maxillary Protraction and Fixed Appliance Therapy On The Pharyngeal AirwayAkash AmbhoreNo ratings yet
- Volumetric Upper AirwayDocument6 pagesVolumetric Upper AirwayCARMEN ROSA AREVALO ROLDANNo ratings yet
- Surgery For Velopharyngeal Dysfunction A Systematic Review of Interventions and OutcomesDocument18 pagesSurgery For Velopharyngeal Dysfunction A Systematic Review of Interventions and Outcomesmohamed zohiriNo ratings yet
- 2019 Effect of Maxillary Expansion and Protraction On The Oropharyngeal Airway in Individuals With Non Syndromic Cleft Palatae Wit or Without Cleft LipDocument23 pages2019 Effect of Maxillary Expansion and Protraction On The Oropharyngeal Airway in Individuals With Non Syndromic Cleft Palatae Wit or Without Cleft LipaprilandralekaNo ratings yet
- Prevalence of Malocclusion in Children With Sleep Disordered BreathingDocument4 pagesPrevalence of Malocclusion in Children With Sleep Disordered BreathingMu'taz ArmanNo ratings yet
- Three Dimensional Facial Morphology Following Surgical Repair of Unilateral Cleft Lip and Palate in Patients After Nasoalveolar MoldingDocument7 pagesThree Dimensional Facial Morphology Following Surgical Repair of Unilateral Cleft Lip and Palate in Patients After Nasoalveolar MoldingnoraveNo ratings yet
- Altered Speech Following Adenoidectomy A 20 Year ExperienceDocument5 pagesAltered Speech Following Adenoidectomy A 20 Year Experienceenfanat23No ratings yet
- 2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDocument7 pages2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDimitris RodriguezNo ratings yet
- Nasal Obstruction and Facial Growth: The Strength of Evidence For Clinical AssumptionsDocument9 pagesNasal Obstruction and Facial Growth: The Strength of Evidence For Clinical AssumptionsSurpreet AroraNo ratings yet
- Medicina Basada en Evidencia. Paladar HendidoDocument5 pagesMedicina Basada en Evidencia. Paladar HendidoDanisse RoaNo ratings yet
- FDSFCFDSFDocument10 pagesFDSFCFDSFBhumika ChawlaNo ratings yet
- 2011 Coronectomy of The Lower Third Molar Is Safe Within The First 3 YearsDocument8 pages2011 Coronectomy of The Lower Third Molar Is Safe Within The First 3 YearskaarlaamendezNo ratings yet
- Medoralv21 I1 p111Document7 pagesMedoralv21 I1 p111Marco ColacinoNo ratings yet
- Craniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingDocument10 pagesCraniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingMonojit DuttaNo ratings yet
- A Cephalometric Study To Evaluate The Variations IDocument6 pagesA Cephalometric Study To Evaluate The Variations IjayashreeNo ratings yet
- AJODO-2013 Pavlin 144 5 637Document2 pagesAJODO-2013 Pavlin 144 5 637osama-alaliNo ratings yet
- Determination of The Occlusal Vertical Dimention in Eduntulos Patients Using Lateral CephalograamsDocument7 pagesDetermination of The Occlusal Vertical Dimention in Eduntulos Patients Using Lateral CephalograamsLeenMash'anNo ratings yet
- Surgical Treatment of Chronic Rhinosinusitis After Sinus LiftDocument5 pagesSurgical Treatment of Chronic Rhinosinusitis After Sinus LiftAnthony LiNo ratings yet
- 2017 Incidence of Secondary Surgery After Modified Furlow Palatoplasty A 20-Year Single-SurgeonDocument6 pages2017 Incidence of Secondary Surgery After Modified Furlow Palatoplasty A 20-Year Single-SurgeonDimitris RodriguezNo ratings yet
- RDENJ Volume 5 Issue 2 Pages 161-167Document7 pagesRDENJ Volume 5 Issue 2 Pages 161-167وليد خالدNo ratings yet
- Susarla 2020Document8 pagesSusarla 2020MarcelaGutiérrezCarranzaNo ratings yet
- Role of MRI in Detection of Repaired Cleft Palate Muscles and Correlation To SpeechDocument6 pagesRole of MRI in Detection of Repaired Cleft Palate Muscles and Correlation To SpeechESTEFANIA LOPEZ OBANDONo ratings yet
- Effect of Mono and BimaxillaryDocument6 pagesEffect of Mono and BimaxillarytamisatnamNo ratings yet
- Demetriades 2010Document6 pagesDemetriades 2010Sai Rakesh ChavaNo ratings yet
- Art 1Document6 pagesArt 1Alvaro Jose Uribe TamaraNo ratings yet
- Comparision of Orofacial Airway Dimensions in Subject With Different Breathing PatternDocument8 pagesComparision of Orofacial Airway Dimensions in Subject With Different Breathing PatternLudy Jiménez ValdiviaNo ratings yet
- Dinh 2021Document6 pagesDinh 2021Mai ThúyNo ratings yet
- Ledderose2021 Article EndoscopicEndonasalRepairOfComDocument7 pagesLedderose2021 Article EndoscopicEndonasalRepairOfComAlejandra Oliveros VargasNo ratings yet
- DownloadDocument16 pagesDownloadhasan nazzalNo ratings yet
- Effects of Rapid Maxillary Expansion On Upper Airway Volume: A Three-Dimensional Cone-Beam Computed Tomography StudyDocument7 pagesEffects of Rapid Maxillary Expansion On Upper Airway Volume: A Three-Dimensional Cone-Beam Computed Tomography StudyVishal SharmaNo ratings yet
- Cleft Lip and Palate: Current Surgical ManagementDocument3 pagesCleft Lip and Palate: Current Surgical ManagementFarisa BelaNo ratings yet
- Sonneveld 2018Document5 pagesSonneveld 2018James Alexander Toruño GordonNo ratings yet
- Jurnal EbmDocument10 pagesJurnal EbmdeasyNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Condensation Risk Assessment 2007 10Document15 pagesCondensation Risk Assessment 2007 10Clef GonadanNo ratings yet
- Al 9351 Tractor and Farm EquipmentsDocument2 pagesAl 9351 Tractor and Farm EquipmentsDhivya PNo ratings yet
- Hiqmat KanthapuraDocument19 pagesHiqmat KanthapuraSohel Bangi0% (1)
- James Clerk Maxwell BiographyDocument3 pagesJames Clerk Maxwell BiographypseudonimNo ratings yet
- Survey 2008Document17 pagesSurvey 2008Thành LongNo ratings yet
- Engineering Management KNR 4553 / KNL 4603: Topic 3 - PlanningDocument23 pagesEngineering Management KNR 4553 / KNL 4603: Topic 3 - PlanningrpjongNo ratings yet
- Letter Writing Business LettersDocument60 pagesLetter Writing Business LettersAvery Jan SilosNo ratings yet
- Full Download Fundamentals of Human Resource Management 5th Edition Noe Test BankDocument35 pagesFull Download Fundamentals of Human Resource Management 5th Edition Noe Test Bankflautistimpend.bkjv100% (43)
- UNIX For Beginners: 1. Introduction: What Is UNIX ?Document21 pagesUNIX For Beginners: 1. Introduction: What Is UNIX ?yemparalaNo ratings yet
- 90ZV-2 Function & StructureDocument499 pages90ZV-2 Function & StructureKawasaki100% (1)
- Demag ZKKE ManualDocument5 pagesDemag ZKKE ManualAlan MaciasNo ratings yet
- Exam 9Document3 pagesExam 9Schuller TechNo ratings yet
- 12 ApspDocument6 pages12 ApspseemasuranaNo ratings yet
- Lec 1Document63 pagesLec 1Hiba ErramiNo ratings yet
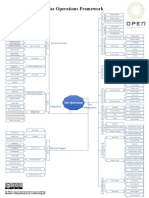
- OCP Framework - Mindmap.2019v1.4Document1 pageOCP Framework - Mindmap.2019v1.4LCNo ratings yet
- Mars Attacks 1996 PDFDocument109 pagesMars Attacks 1996 PDFJay ConnorNo ratings yet
- PDMS Forum TipsDocument3 pagesPDMS Forum TipsSudheepNo ratings yet
- Volland 2016Document20 pagesVolland 2016Amira FerianiNo ratings yet
- Com. English 1st Term Exam XIDocument3 pagesCom. English 1st Term Exam XIjohnadhikari999No ratings yet
- Principle/S Involved:: Chemical Formula of The Reagent Used Role/Use in The Experiment Naoh Na H Y - 2H O MGCL - 6H ODocument2 pagesPrinciple/S Involved:: Chemical Formula of The Reagent Used Role/Use in The Experiment Naoh Na H Y - 2H O MGCL - 6H OCathrina Andrea RamosNo ratings yet
- Book Review: Self-Declaration of "No Plagiarism"Document3 pagesBook Review: Self-Declaration of "No Plagiarism"Movies PictureNo ratings yet
- B05 - Environmental AccountingDocument10 pagesB05 - Environmental AccountingAcca BooksNo ratings yet
- ShaftingDocument7 pagesShaftingMico CampoNo ratings yet
- Burnette, Pollack, ForsythDocument12 pagesBurnette, Pollack, ForsythAmadeus ChinNo ratings yet
- Part 26, 2017 - 07Document82 pagesPart 26, 2017 - 07vallirajuNo ratings yet
- Amt in Household and ServicesDocument25 pagesAmt in Household and ServicesShabby Gay TroganiNo ratings yet
- Applied Business Unit 2 CourseworkDocument7 pagesApplied Business Unit 2 Courseworkykzdmfajd100% (2)
- Three: Evaluating A Company's External EnvironmentDocument30 pagesThree: Evaluating A Company's External EnvironmentPromiti SarkerNo ratings yet
- Products Used in Steel Manufacturing (ZAM)Document31 pagesProducts Used in Steel Manufacturing (ZAM)osama raufNo ratings yet