
Intersurgical Trachseal
Intersurgical Trachseal
You might also like
- 9E-A User Manuals and ServiceDocument10 pages9E-A User Manuals and Servicerponce161276No ratings yet
- Oropharyngeal, Tracheal, and Endotracheal SuctioningDocument6 pagesOropharyngeal, Tracheal, and Endotracheal SuctioningFaisal QureshiNo ratings yet
- Basic Airway ManagementDocument98 pagesBasic Airway ManagementRani Salsabilah100% (1)
- OBDocument7 pagesOBJune DianNo ratings yet
- First Two Steps Are Discussed in This SectionDocument26 pagesFirst Two Steps Are Discussed in This SectionArchanaShenoyNo ratings yet
- Critical Care SuctioningDocument5 pagesCritical Care SuctioningChinta Nabila 조롱 수없는No ratings yet
- Ateneo de Zamboanga University: Nursing Skills Output (Nso)Document9 pagesAteneo de Zamboanga University: Nursing Skills Output (Nso)Mitzi BelamideNo ratings yet
- 7 Steps Closed SuctionDocument4 pages7 Steps Closed SuctionerlintanNo ratings yet
- Na So Faring EalDocument5 pagesNa So Faring EalDian Putri ListyantiNo ratings yet
- Respironics WhisperFlow CPAP - User ManualDocument24 pagesRespironics WhisperFlow CPAP - User ManualJoão Francisco MontanhaniNo ratings yet
- Airway Mngt. Module 5Document21 pagesAirway Mngt. Module 5jubelynNo ratings yet
- 508 Cuff Leak Test Procedure 508/ Page 1 of 4: DescriptionDocument4 pages508 Cuff Leak Test Procedure 508/ Page 1 of 4: DescriptionM. Aulia RakhmanNo ratings yet
- Instrução de UsoDocument57 pagesInstrução de Usobiomedical_com_brNo ratings yet
- Suction Endotracheal V P StgeorgeDocument3 pagesSuction Endotracheal V P StgeorgeElaine Iris AbastaNo ratings yet
- SuctioningDocument18 pagesSuctioningFadz HadjiriNo ratings yet
- Oro Nasopharyngeal Suctioning 1Document13 pagesOro Nasopharyngeal Suctioning 1Lovely Mae DulvaNo ratings yet
- Sop Perawatan WSD Dan Tracheostomy, NebulizerDocument12 pagesSop Perawatan WSD Dan Tracheostomy, NebulizerSyamsiah AnwarNo ratings yet
- P 10 Ion StandardDocument5 pagesP 10 Ion StandardBeatrix RunkelNo ratings yet
- Specimen Collection Sputum Skill COVID 19 Toolkit - 010320 PDFDocument7 pagesSpecimen Collection Sputum Skill COVID 19 Toolkit - 010320 PDFMary AlabiNo ratings yet
- Instructions For Use: Nfusion YstemDocument80 pagesInstructions For Use: Nfusion Ystembiomedical_com_brNo ratings yet
- Adult NasalDocument14 pagesAdult NasalillirpohnimNo ratings yet
- Suctioning PDFDocument6 pagesSuctioning PDFIonel AfteneNo ratings yet
- Tracheostomy Suctioning SkillDocument6 pagesTracheostomy Suctioning Skill3thanKimNo ratings yet
- Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)Document7 pagesEndotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)DCaeiroNo ratings yet
- SUCTIONING PPT HandoutsDocument30 pagesSUCTIONING PPT HandoutsTanya FaustinoNo ratings yet
- Tracheostomy SuctioningDocument59 pagesTracheostomy SuctioningMaan LapitanNo ratings yet
- Tugas Kelompok 2 BHS Inggris SopDocument17 pagesTugas Kelompok 2 BHS Inggris Sopmoms naraNo ratings yet
- Open or Closed System SuctioningDocument6 pagesOpen or Closed System SuctioningGerard Rivera GenerosoNo ratings yet
- Hypo & HyperthyroidismDocument33 pagesHypo & HyperthyroidismSuchit Kumar50% (2)
- PRECAUTIONS FOR-WPS OfficeDocument5 pagesPRECAUTIONS FOR-WPS Officemkoboni23No ratings yet
- Suctioning: Endotracheal/ Tracheal Suctioning ProcedureDocument3 pagesSuctioning: Endotracheal/ Tracheal Suctioning ProcedureChristine_P_Es_229No ratings yet
- Balón Dilatación Acalasia RigiflexDocument28 pagesBalón Dilatación Acalasia RigiflexMuriel AlejandraNo ratings yet
- Model 88E39 Blast Helmet: Instruction ManualDocument12 pagesModel 88E39 Blast Helmet: Instruction ManualkarijosephNo ratings yet
- Decanulasi TrakeostomiDocument6 pagesDecanulasi TrakeostomiDhiel Muhammad FarreyraNo ratings yet
- SuctioningDocument24 pagesSuctioningLanz LlnsNo ratings yet
- ECMO Protocol AustraliaDocument17 pagesECMO Protocol AustraliaBiswarup Purkayastha100% (1)
- Airway SuctioningDocument30 pagesAirway SuctioningPearl DiBerardinoNo ratings yet
- TRACHEOSTOMYDocument109 pagesTRACHEOSTOMYJayson RN92% (12)
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- Catálogo Anderson Greenwood 400sDocument32 pagesCatálogo Anderson Greenwood 400sDaniela BeltranNo ratings yet
- CH 2 SuctioningDocument90 pagesCH 2 SuctioningMaherNo ratings yet
- Suctioning TracheaDocument24 pagesSuctioning Trachealuis_chubee100% (1)
- Care of Patients With Mechanical VentilatorDocument4 pagesCare of Patients With Mechanical VentilatorIman Bee Sanayon0% (1)
- ET SuctioningDocument8 pagesET SuctioningSylvia LoongNo ratings yet
- SuctionNing ProacessDocument24 pagesSuctionNing Proacesspop lopNo ratings yet
- Anaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandDocument40 pagesAnaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandCrystieNo ratings yet
- MedSurg NotesDocument57 pagesMedSurg NotesCHRISTOFER CORONADONo ratings yet
- SuctioningDocument24 pagesSuctioningzhaimeangirlNo ratings yet
- Nasopharyngeal Airway SuctioningDocument3 pagesNasopharyngeal Airway SuctioningHaitham ZraigatNo ratings yet
- Spirometry: Performance and Interpretation A Guide For General PractitionersDocument15 pagesSpirometry: Performance and Interpretation A Guide For General PractitionersAgi AngloSaxonNo ratings yet
- NGT Insertion Directly From CanvasDocument6 pagesNGT Insertion Directly From CanvasRico Delgado of WorldbexNo ratings yet
- Spirometry: Arrazi ClinicsDocument8 pagesSpirometry: Arrazi ClinicsJ Russel DichosoNo ratings yet
- Laboratory Unit 3 1Document6 pagesLaboratory Unit 3 1Mushy_ayaNo ratings yet
- CRT HintDocument47 pagesCRT HintEloisa Marie ReyesNo ratings yet
- SCBA ProgramDocument7 pagesSCBA Programrajakhurshed7185No ratings yet
- SuctioningDocument13 pagesSuctioningAmanda ScarletNo ratings yet
- Percutaneous Emergency Oxygenation Strategies in the “Can’t Intubate, Can’t Oxygenate” Scenario: PEOS in the CICO Scenario, #2From EverandPercutaneous Emergency Oxygenation Strategies in the “Can’t Intubate, Can’t Oxygenate” Scenario: PEOS in the CICO Scenario, #2No ratings yet
- Contemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsFrom EverandContemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsNo ratings yet
- Community EngagementDocument16 pagesCommunity EngagementJune DianNo ratings yet
- Computers and NursingDocument6 pagesComputers and NursingJune DianNo ratings yet
- Mrs CampanaDocument2 pagesMrs CampanaJune DianNo ratings yet
- Inducing Labor at 39 Weeks Decreases Need For Cesarean SectionDocument2 pagesInducing Labor at 39 Weeks Decreases Need For Cesarean SectionJune DianNo ratings yet
- Human Infectious Diseases and Risk of Preeclampsia: An Updated Review of The LiteratureDocument12 pagesHuman Infectious Diseases and Risk of Preeclampsia: An Updated Review of The LiteratureasfwegereNo ratings yet
- Clinical MedecineDocument314 pagesClinical MedecineAdriana IoanaNo ratings yet
- Concurrent ChemoRadiotherapyDocument51 pagesConcurrent ChemoRadiotherapyJalal EltabibNo ratings yet
- Trace ElementsDocument5 pagesTrace ElementsFaithNo ratings yet
- What Acupuncture Is Made For and Just How It Can HelpDocument2 pagesWhat Acupuncture Is Made For and Just How It Can HelpTerryCollins2No ratings yet
- Stricture Urethra in Children: An Indian Perspective: Original ArticleDocument6 pagesStricture Urethra in Children: An Indian Perspective: Original ArticleLilis Endah SulistiyawatiNo ratings yet
- Practical and Theoretical Seminar Of: Bioprogressive ScienceDocument5 pagesPractical and Theoretical Seminar Of: Bioprogressive SciencesaberNo ratings yet
- Gestational Trophoblastic DiseaseDocument40 pagesGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- Kti Vida HusniaDocument49 pagesKti Vida HusniaElsa AghniaNo ratings yet
- Hyperkalemia: Ateneo de Naga University College of Nursing Nursing Care PlanDocument1 pageHyperkalemia: Ateneo de Naga University College of Nursing Nursing Care PlanRenie Serrano100% (1)
- Oils, Blends & Products Recommended:: Reflexology PointsDocument2 pagesOils, Blends & Products Recommended:: Reflexology Pointshmaddy3117No ratings yet
- Emerging Ifectious DiseasesDocument179 pagesEmerging Ifectious DiseasesEleni ThalassinouNo ratings yet
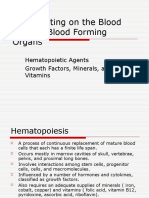
- Drugs Acting On The Blood and The BloodDocument26 pagesDrugs Acting On The Blood and The BloodHealthy7No ratings yet
- Afina Fitra Firdaus Ppds Ipd 50Document30 pagesAfina Fitra Firdaus Ppds Ipd 5050Afina Fitra FirdausNo ratings yet
- Application FormDocument5 pagesApplication Formapi-603319031No ratings yet
- Mommy JDocument2 pagesMommy JGeean59% (22)
- Cold Chain System and Adverse Reaction Following Immunization (Aefi)Document46 pagesCold Chain System and Adverse Reaction Following Immunization (Aefi)Shikya AbnasNo ratings yet
- A.1 AbortionDocument47 pagesA.1 AbortionRiza Mae Follero DanteNo ratings yet
- Coxa Plana-Legg DiseaseDocument10 pagesCoxa Plana-Legg DiseasejosephineNo ratings yet
- Medical Semiology Respiratory SystemDocument111 pagesMedical Semiology Respiratory SystemNadir al bu lahNo ratings yet
- Mucosta Drug Interactions - MIMS MalaysiaDocument4 pagesMucosta Drug Interactions - MIMS MalaysiaEsy LNo ratings yet
- Intercom March 2013Document5 pagesIntercom March 2013Lexington Medical CenterNo ratings yet
- PM201428 (8) Brinkman StoppelenburgDocument27 pagesPM201428 (8) Brinkman StoppelenburgAnanda Soraya B.No ratings yet
- SGH Paediatrics Guide 2020 08Document44 pagesSGH Paediatrics Guide 2020 08Yoseph SeleshiNo ratings yet
- Sagum, Diana Rose - (Pelvic)Document1 pageSagum, Diana Rose - (Pelvic)AUSTRIAN DIAGNOSTIC CENTERNo ratings yet
- Hematocrite Values With High Measurement of Eritrosit After Centrifugation On Serum MakingDocument10 pagesHematocrite Values With High Measurement of Eritrosit After Centrifugation On Serum MakingPutri Aswariyah RamliNo ratings yet
- Telescopium) EXTRACTS: West Visayas State University College of MedicineDocument5 pagesTelescopium) EXTRACTS: West Visayas State University College of MedicineMark FuerteNo ratings yet
- PHYSICAL FITNESS TEST PFT SCORE SHEET FO-revisedDocument1 pagePHYSICAL FITNESS TEST PFT SCORE SHEET FO-revisedMary Grace DeramasNo ratings yet
- Osteoporosis in Postmenopausal WomenDocument37 pagesOsteoporosis in Postmenopausal WomenKhalid AhmedNo ratings yet
- Cancerchemo TocDocument6 pagesCancerchemo TocMoatez HlmNo ratings yet





























































































Download as docx, pdf, or txt
You might also like
- 9E-A User Manuals and ServiceDocument10 pages9E-A User Manuals and Servicerponce161276No ratings yet
- Oropharyngeal, Tracheal, and Endotracheal SuctioningDocument6 pagesOropharyngeal, Tracheal, and Endotracheal SuctioningFaisal QureshiNo ratings yet
- Basic Airway ManagementDocument98 pagesBasic Airway ManagementRani Salsabilah100% (1)
- OBDocument7 pagesOBJune DianNo ratings yet
- First Two Steps Are Discussed in This SectionDocument26 pagesFirst Two Steps Are Discussed in This SectionArchanaShenoyNo ratings yet
- Critical Care SuctioningDocument5 pagesCritical Care SuctioningChinta Nabila 조롱 수없는No ratings yet
- Ateneo de Zamboanga University: Nursing Skills Output (Nso)Document9 pagesAteneo de Zamboanga University: Nursing Skills Output (Nso)Mitzi BelamideNo ratings yet
- 7 Steps Closed SuctionDocument4 pages7 Steps Closed SuctionerlintanNo ratings yet
- Na So Faring EalDocument5 pagesNa So Faring EalDian Putri ListyantiNo ratings yet
- Respironics WhisperFlow CPAP - User ManualDocument24 pagesRespironics WhisperFlow CPAP - User ManualJoão Francisco MontanhaniNo ratings yet
- Airway Mngt. Module 5Document21 pagesAirway Mngt. Module 5jubelynNo ratings yet
- 508 Cuff Leak Test Procedure 508/ Page 1 of 4: DescriptionDocument4 pages508 Cuff Leak Test Procedure 508/ Page 1 of 4: DescriptionM. Aulia RakhmanNo ratings yet
- Instrução de UsoDocument57 pagesInstrução de Usobiomedical_com_brNo ratings yet
- Suction Endotracheal V P StgeorgeDocument3 pagesSuction Endotracheal V P StgeorgeElaine Iris AbastaNo ratings yet
- SuctioningDocument18 pagesSuctioningFadz HadjiriNo ratings yet
- Oro Nasopharyngeal Suctioning 1Document13 pagesOro Nasopharyngeal Suctioning 1Lovely Mae DulvaNo ratings yet
- Sop Perawatan WSD Dan Tracheostomy, NebulizerDocument12 pagesSop Perawatan WSD Dan Tracheostomy, NebulizerSyamsiah AnwarNo ratings yet
- P 10 Ion StandardDocument5 pagesP 10 Ion StandardBeatrix RunkelNo ratings yet
- Specimen Collection Sputum Skill COVID 19 Toolkit - 010320 PDFDocument7 pagesSpecimen Collection Sputum Skill COVID 19 Toolkit - 010320 PDFMary AlabiNo ratings yet
- Instructions For Use: Nfusion YstemDocument80 pagesInstructions For Use: Nfusion Ystembiomedical_com_brNo ratings yet
- Adult NasalDocument14 pagesAdult NasalillirpohnimNo ratings yet
- Suctioning PDFDocument6 pagesSuctioning PDFIonel AfteneNo ratings yet
- Tracheostomy Suctioning SkillDocument6 pagesTracheostomy Suctioning Skill3thanKimNo ratings yet
- Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)Document7 pagesEndotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)DCaeiroNo ratings yet
- SUCTIONING PPT HandoutsDocument30 pagesSUCTIONING PPT HandoutsTanya FaustinoNo ratings yet
- Tracheostomy SuctioningDocument59 pagesTracheostomy SuctioningMaan LapitanNo ratings yet
- Tugas Kelompok 2 BHS Inggris SopDocument17 pagesTugas Kelompok 2 BHS Inggris Sopmoms naraNo ratings yet
- Open or Closed System SuctioningDocument6 pagesOpen or Closed System SuctioningGerard Rivera GenerosoNo ratings yet
- Hypo & HyperthyroidismDocument33 pagesHypo & HyperthyroidismSuchit Kumar50% (2)
- PRECAUTIONS FOR-WPS OfficeDocument5 pagesPRECAUTIONS FOR-WPS Officemkoboni23No ratings yet
- Suctioning: Endotracheal/ Tracheal Suctioning ProcedureDocument3 pagesSuctioning: Endotracheal/ Tracheal Suctioning ProcedureChristine_P_Es_229No ratings yet
- Balón Dilatación Acalasia RigiflexDocument28 pagesBalón Dilatación Acalasia RigiflexMuriel AlejandraNo ratings yet
- Model 88E39 Blast Helmet: Instruction ManualDocument12 pagesModel 88E39 Blast Helmet: Instruction ManualkarijosephNo ratings yet
- Decanulasi TrakeostomiDocument6 pagesDecanulasi TrakeostomiDhiel Muhammad FarreyraNo ratings yet
- SuctioningDocument24 pagesSuctioningLanz LlnsNo ratings yet
- ECMO Protocol AustraliaDocument17 pagesECMO Protocol AustraliaBiswarup Purkayastha100% (1)
- Airway SuctioningDocument30 pagesAirway SuctioningPearl DiBerardinoNo ratings yet
- TRACHEOSTOMYDocument109 pagesTRACHEOSTOMYJayson RN92% (12)
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- Catálogo Anderson Greenwood 400sDocument32 pagesCatálogo Anderson Greenwood 400sDaniela BeltranNo ratings yet
- CH 2 SuctioningDocument90 pagesCH 2 SuctioningMaherNo ratings yet
- Suctioning TracheaDocument24 pagesSuctioning Trachealuis_chubee100% (1)
- Care of Patients With Mechanical VentilatorDocument4 pagesCare of Patients With Mechanical VentilatorIman Bee Sanayon0% (1)
- ET SuctioningDocument8 pagesET SuctioningSylvia LoongNo ratings yet
- SuctionNing ProacessDocument24 pagesSuctionNing Proacesspop lopNo ratings yet
- Anaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandDocument40 pagesAnaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandCrystieNo ratings yet
- MedSurg NotesDocument57 pagesMedSurg NotesCHRISTOFER CORONADONo ratings yet
- SuctioningDocument24 pagesSuctioningzhaimeangirlNo ratings yet
- Nasopharyngeal Airway SuctioningDocument3 pagesNasopharyngeal Airway SuctioningHaitham ZraigatNo ratings yet
- Spirometry: Performance and Interpretation A Guide For General PractitionersDocument15 pagesSpirometry: Performance and Interpretation A Guide For General PractitionersAgi AngloSaxonNo ratings yet
- NGT Insertion Directly From CanvasDocument6 pagesNGT Insertion Directly From CanvasRico Delgado of WorldbexNo ratings yet
- Spirometry: Arrazi ClinicsDocument8 pagesSpirometry: Arrazi ClinicsJ Russel DichosoNo ratings yet
- Laboratory Unit 3 1Document6 pagesLaboratory Unit 3 1Mushy_ayaNo ratings yet
- CRT HintDocument47 pagesCRT HintEloisa Marie ReyesNo ratings yet
- SCBA ProgramDocument7 pagesSCBA Programrajakhurshed7185No ratings yet
- SuctioningDocument13 pagesSuctioningAmanda ScarletNo ratings yet
- Percutaneous Emergency Oxygenation Strategies in the “Can’t Intubate, Can’t Oxygenate” Scenario: PEOS in the CICO Scenario, #2From EverandPercutaneous Emergency Oxygenation Strategies in the “Can’t Intubate, Can’t Oxygenate” Scenario: PEOS in the CICO Scenario, #2No ratings yet
- Contemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsFrom EverandContemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsNo ratings yet
- Community EngagementDocument16 pagesCommunity EngagementJune DianNo ratings yet
- Computers and NursingDocument6 pagesComputers and NursingJune DianNo ratings yet
- Mrs CampanaDocument2 pagesMrs CampanaJune DianNo ratings yet
- Inducing Labor at 39 Weeks Decreases Need For Cesarean SectionDocument2 pagesInducing Labor at 39 Weeks Decreases Need For Cesarean SectionJune DianNo ratings yet
- Human Infectious Diseases and Risk of Preeclampsia: An Updated Review of The LiteratureDocument12 pagesHuman Infectious Diseases and Risk of Preeclampsia: An Updated Review of The LiteratureasfwegereNo ratings yet
- Clinical MedecineDocument314 pagesClinical MedecineAdriana IoanaNo ratings yet
- Concurrent ChemoRadiotherapyDocument51 pagesConcurrent ChemoRadiotherapyJalal EltabibNo ratings yet
- Trace ElementsDocument5 pagesTrace ElementsFaithNo ratings yet
- What Acupuncture Is Made For and Just How It Can HelpDocument2 pagesWhat Acupuncture Is Made For and Just How It Can HelpTerryCollins2No ratings yet
- Stricture Urethra in Children: An Indian Perspective: Original ArticleDocument6 pagesStricture Urethra in Children: An Indian Perspective: Original ArticleLilis Endah SulistiyawatiNo ratings yet
- Practical and Theoretical Seminar Of: Bioprogressive ScienceDocument5 pagesPractical and Theoretical Seminar Of: Bioprogressive SciencesaberNo ratings yet
- Gestational Trophoblastic DiseaseDocument40 pagesGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- Kti Vida HusniaDocument49 pagesKti Vida HusniaElsa AghniaNo ratings yet
- Hyperkalemia: Ateneo de Naga University College of Nursing Nursing Care PlanDocument1 pageHyperkalemia: Ateneo de Naga University College of Nursing Nursing Care PlanRenie Serrano100% (1)
- Oils, Blends & Products Recommended:: Reflexology PointsDocument2 pagesOils, Blends & Products Recommended:: Reflexology Pointshmaddy3117No ratings yet
- Emerging Ifectious DiseasesDocument179 pagesEmerging Ifectious DiseasesEleni ThalassinouNo ratings yet
- Drugs Acting On The Blood and The BloodDocument26 pagesDrugs Acting On The Blood and The BloodHealthy7No ratings yet
- Afina Fitra Firdaus Ppds Ipd 50Document30 pagesAfina Fitra Firdaus Ppds Ipd 5050Afina Fitra FirdausNo ratings yet
- Application FormDocument5 pagesApplication Formapi-603319031No ratings yet
- Mommy JDocument2 pagesMommy JGeean59% (22)
- Cold Chain System and Adverse Reaction Following Immunization (Aefi)Document46 pagesCold Chain System and Adverse Reaction Following Immunization (Aefi)Shikya AbnasNo ratings yet
- A.1 AbortionDocument47 pagesA.1 AbortionRiza Mae Follero DanteNo ratings yet
- Coxa Plana-Legg DiseaseDocument10 pagesCoxa Plana-Legg DiseasejosephineNo ratings yet
- Medical Semiology Respiratory SystemDocument111 pagesMedical Semiology Respiratory SystemNadir al bu lahNo ratings yet
- Mucosta Drug Interactions - MIMS MalaysiaDocument4 pagesMucosta Drug Interactions - MIMS MalaysiaEsy LNo ratings yet
- Intercom March 2013Document5 pagesIntercom March 2013Lexington Medical CenterNo ratings yet
- PM201428 (8) Brinkman StoppelenburgDocument27 pagesPM201428 (8) Brinkman StoppelenburgAnanda Soraya B.No ratings yet
- SGH Paediatrics Guide 2020 08Document44 pagesSGH Paediatrics Guide 2020 08Yoseph SeleshiNo ratings yet
- Sagum, Diana Rose - (Pelvic)Document1 pageSagum, Diana Rose - (Pelvic)AUSTRIAN DIAGNOSTIC CENTERNo ratings yet
- Hematocrite Values With High Measurement of Eritrosit After Centrifugation On Serum MakingDocument10 pagesHematocrite Values With High Measurement of Eritrosit After Centrifugation On Serum MakingPutri Aswariyah RamliNo ratings yet
- Telescopium) EXTRACTS: West Visayas State University College of MedicineDocument5 pagesTelescopium) EXTRACTS: West Visayas State University College of MedicineMark FuerteNo ratings yet
- PHYSICAL FITNESS TEST PFT SCORE SHEET FO-revisedDocument1 pagePHYSICAL FITNESS TEST PFT SCORE SHEET FO-revisedMary Grace DeramasNo ratings yet
- Osteoporosis in Postmenopausal WomenDocument37 pagesOsteoporosis in Postmenopausal WomenKhalid AhmedNo ratings yet
- Cancerchemo TocDocument6 pagesCancerchemo TocMoatez HlmNo ratings yet