Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Monster Treasure Assortment Set 2 Levels 4 6Document12 pagesMonster Treasure Assortment Set 2 Levels 4 6Nic Trotti100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Colligative Properties and AnswerDocument3 pagesColligative Properties and AnswerTai PanNo ratings yet
- EP2500 User Manual PDFDocument72 pagesEP2500 User Manual PDFThomas LunaNo ratings yet
- SAP Cash Management PresentationDocument16 pagesSAP Cash Management Presentationmuneendra030650% (2)
- Oracle Project Procurement Process GuideDocument100 pagesOracle Project Procurement Process GuideSrinivasa Rao AsuruNo ratings yet
- RandomDocument1,919 pagesRandomNajmul Puda Pappadam50% (2)
- Neighborhood and Connectivity of PixelsDocument25 pagesNeighborhood and Connectivity of Pixelswit12345No ratings yet
- History of AnatomyDocument21 pagesHistory of AnatomyCatarina SimõesNo ratings yet
- Stan 2012Document4 pagesStan 2012Gerson OrtegaNo ratings yet
- Grade 6 EnglishDocument249 pagesGrade 6 Englishgetacheweyob74No ratings yet
- Portal Frames ConstructionDocument47 pagesPortal Frames ConstructionYashi GuptaNo ratings yet
- Euroncap 2017 Kia Picanto DatasheetDocument11 pagesEuroncap 2017 Kia Picanto DatasheetYassine SaberNo ratings yet
- 06 Part Location Guide ATA 24Document8 pages06 Part Location Guide ATA 24Ernesto Antonio Grande SantosNo ratings yet
- PDFDocument374 pagesPDFSushmìta NirmalNo ratings yet
- Guest FolioDocument2 pagesGuest FolioJulyca SimbajonNo ratings yet
- Laguna Northwestern College: San Lorenzo Ruiz Montessori CenterDocument2 pagesLaguna Northwestern College: San Lorenzo Ruiz Montessori CenterMichael RojoNo ratings yet
- Marketing Moguls Gartons IIM Kashipur FinalsDocument22 pagesMarketing Moguls Gartons IIM Kashipur FinalsTarun SinghNo ratings yet
- Extreme Loading For Structures - WikipediaDocument5 pagesExtreme Loading For Structures - WikipediaEn Iyisi İnşaat MühendisiNo ratings yet
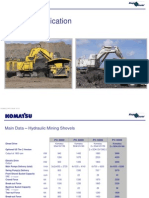
- 11 - PC8000 - 6 ApplDocument37 pages11 - PC8000 - 6 Appljhon jairo trujillo100% (1)
- Final Unit 4Document21 pagesFinal Unit 4Ayessa AnchetaNo ratings yet
- OB Case Study-1Document4 pagesOB Case Study-1melat bizu0% (1)
- 3rd Prep - M.SDocument52 pages3rd Prep - M.ShaithamNo ratings yet
- A New Mutuel Kerberos Authentication Protocol For Distributed SystemsDocument10 pagesA New Mutuel Kerberos Authentication Protocol For Distributed SystemsRahul prabhaNo ratings yet
- ENG201 Mid Term Past Paper 2Document6 pagesENG201 Mid Term Past Paper 2malik100% (1)
- Try It For Yourself: Platform OverviewDocument32 pagesTry It For Yourself: Platform OverviewМаниш НахтвандерерNo ratings yet
- AP Bio Cram Chart 2021Document1 pageAP Bio Cram Chart 2021Evangeline YaoNo ratings yet
- Internal Control PSA315Document8 pagesInternal Control PSA315John Lexter Macalber100% (1)
- PedodonticsDocument2 pagesPedodonticsjunquelalaNo ratings yet
- Itachi - Bright Light Chapter 4Document21 pagesItachi - Bright Light Chapter 4Koji ChoqueticllaNo ratings yet
- SP Initial 1-5K - ManualDocument37 pagesSP Initial 1-5K - ManualkobochanstoreNo ratings yet