Download as pdf or txt
You might also like
- Continum Epilepsy.2019 PDFDocument307 pagesContinum Epilepsy.2019 PDFLaura Ochoa100% (1)
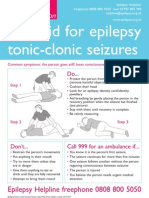
- Epilepsyaction FirstaidpostersDocument2 pagesEpilepsyaction FirstaidpostersKheliwiNo ratings yet
- Epilepsy Fact Sheet PresentationDocument39 pagesEpilepsy Fact Sheet Presentationflm999100% (2)
- Predictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsDocument12 pagesPredictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsPrabaningrum DwidjoasmoroNo ratings yet
- Fitzgerald Et Al. 2021 - Improving The Prediction of Epilepsy Surgery Outcomes Using Basic Scalp EEG FindingsDocument12 pagesFitzgerald Et Al. 2021 - Improving The Prediction of Epilepsy Surgery Outcomes Using Basic Scalp EEG FindingsLuís PachecoNo ratings yet
- Behdad Et Al-2009-EpilepsiaDocument12 pagesBehdad Et Al-2009-EpilepsiaNathaly LapoNo ratings yet
- Z Score SISCOMDocument9 pagesZ Score SISCOMAiswarya HariNo ratings yet
- PaparDocument7 pagesPaparishitaNo ratings yet
- Vestibular Neuritis Affects Both Superior and Inferior Vestibular NervesDocument10 pagesVestibular Neuritis Affects Both Superior and Inferior Vestibular NervesSabina BădilăNo ratings yet
- Electrocorticographic Monitoring As An Alternative Tool For The Pre-Surgical Evaluation of Patients With Bi-Temporal EpilepsyDocument7 pagesElectrocorticographic Monitoring As An Alternative Tool For The Pre-Surgical Evaluation of Patients With Bi-Temporal Epilepsydavidmy227464No ratings yet
- Rabin Stein 2010Document6 pagesRabin Stein 2010luis fermin paredesNo ratings yet
- Long Term Outcome of Temporal Lobe Epilepsy Surgery: Analyses of 140 Consecutive PatientsDocument10 pagesLong Term Outcome of Temporal Lobe Epilepsy Surgery: Analyses of 140 Consecutive PatientsIlham Kelian RamadhanNo ratings yet
- Frontal Lobe Epilepsy in A Pediatric Population: Characterization of Clinical Manifestations and SemiologyDocument9 pagesFrontal Lobe Epilepsy in A Pediatric Population: Characterization of Clinical Manifestations and SemiologyMaNolioxNo ratings yet
- CC Helps in LocalisationDocument9 pagesCC Helps in LocalisationRavi ChandraNo ratings yet
- G. Rees Cosgrove, M.D., F.R.C.S. (C) and Andrew J. Cole M.D., FRCP (C)Document11 pagesG. Rees Cosgrove, M.D., F.R.C.S. (C) and Andrew J. Cole M.D., FRCP (C)Jean Costan RNNo ratings yet
- SISCOM-Meta AnalysisDocument8 pagesSISCOM-Meta AnalysisAiswarya HariNo ratings yet
- Posterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsDocument7 pagesPosterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsJasper CubiasNo ratings yet
- Heterotopia PV GruposDocument12 pagesHeterotopia PV GruposJuan D. HoyosNo ratings yet
- The Long-Term Outcome of Adult Epilepsy Surgery, Patterns of Seizure Remission, and Relapse - A Cohort StudyDocument8 pagesThe Long-Term Outcome of Adult Epilepsy Surgery, Patterns of Seizure Remission, and Relapse - A Cohort StudyNeurologia homicNo ratings yet
- MRI SeizuresDocument7 pagesMRI SeizuresMarco MalagaNo ratings yet
- Long-Term Outcome Characteristics in Mesial Temporal Lobe Epilepsy With and Without Associated Cortical DysplasiaDocument10 pagesLong-Term Outcome Characteristics in Mesial Temporal Lobe Epilepsy With and Without Associated Cortical DysplasiaGesael Passos Ferreira JuniorNo ratings yet
- Utility of Routine EEG in Emergency Room and Inpatient ServiceDocument16 pagesUtility of Routine EEG in Emergency Room and Inpatient Servicefedcaf18No ratings yet
- Mink in 2021Document8 pagesMink in 2021Anonymous OT2xHY1UNo ratings yet
- Pleds 2009 JamaDocument7 pagesPleds 2009 JamaRosiane Da Silva FontanaNo ratings yet
- Surgical Management and Long-Term Outcome of Pediatric Patients With Different Subtypes of Epilepsy Associated With Cerebral Cavernous MalformationsDocument7 pagesSurgical Management and Long-Term Outcome of Pediatric Patients With Different Subtypes of Epilepsy Associated With Cerebral Cavernous MalformationsGonzalo Leonidas Rojas DelgadoNo ratings yet
- Adlantos en La EpilepsiaDocument6 pagesAdlantos en La EpilepsiaCaro CortésNo ratings yet
- Interictal Pattern On Scalp Electroencephalogram Predicts Excellent Surgical Outcome of Epilepsy Caused by Focal Cortical DysplasiaDocument11 pagesInterictal Pattern On Scalp Electroencephalogram Predicts Excellent Surgical Outcome of Epilepsy Caused by Focal Cortical DysplasiaLuís PachecoNo ratings yet
- Clarke 2020Document6 pagesClarke 2020Lobo CalupohNo ratings yet
- Frontal Lobe SeizuresDocument14 pagesFrontal Lobe SeizuresfeawefNo ratings yet
- Multiples Resecciones EpilepsiaDocument17 pagesMultiples Resecciones EpilepsiaAlejandra SaenzNo ratings yet
- Presuregry EvaluationDocument8 pagesPresuregry Evaluationbhadresh neuro mangukiyaNo ratings yet
- Epilepsia - 2018 - GibbsDocument5 pagesEpilepsia - 2018 - GibbsYenny MaharaniNo ratings yet
- Abstracts of The 2018 AANS/CNS Joint Section On Disorders of The Spine and Peripheral Nerves Annual MeetingDocument109 pagesAbstracts of The 2018 AANS/CNS Joint Section On Disorders of The Spine and Peripheral Nerves Annual MeetingEka Wahyu HerdiyantiNo ratings yet
- 1 s2.0 S1059131107000842 MainDocument12 pages1 s2.0 S1059131107000842 MainNathaly LapoNo ratings yet
- Preoperative Prognostic Value of MRI Findings in 108 Patients With Idiopathic Normal Pressure HydrocephalusDocument9 pagesPreoperative Prognostic Value of MRI Findings in 108 Patients With Idiopathic Normal Pressure HydrocephalusSantiago FuentesNo ratings yet
- Hodnett Et Al 2015 Clinical Anatomy 2Document7 pagesHodnett Et Al 2015 Clinical Anatomy 2ChrissNo ratings yet
- MainDocument12 pagesMainbozasnachoNo ratings yet
- J Clinph 2013 03 031Document7 pagesJ Clinph 2013 03 031Andres Rojas JerezNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Riri KumalaNo ratings yet
- Importance of Long-Term EEG in Seizure-Free PatienDocument5 pagesImportance of Long-Term EEG in Seizure-Free PatienChu Thị NghiệpNo ratings yet
- PicadoDocument3 pagesPicadoGrigori ChulakiNo ratings yet
- Jurnal Bedah SarafDocument10 pagesJurnal Bedah SarafSarah AmaniNo ratings yet
- Journal 7 N.vii 7Document5 pagesJournal 7 N.vii 7Azmi FananyNo ratings yet
- Visual Evoked Potentials in Guillain-Barré Syndrome: MethodsDocument6 pagesVisual Evoked Potentials in Guillain-Barré Syndrome: MethodsYulianti PurnamasariNo ratings yet
- Epilepsy SurgeryDocument13 pagesEpilepsy SurgeryMatthew DavisNo ratings yet
- FocusDocument7 pagesFocusRafaelNo ratings yet
- Surgical Management of Epilepsy 9.12.18Document32 pagesSurgical Management of Epilepsy 9.12.18Dr.Humayun Rashid SagorNo ratings yet
- Epidermoid Cysts TNEDocument10 pagesEpidermoid Cysts TNEbello_england_209552No ratings yet
- Meniere's DiseaseDocument5 pagesMeniere's DiseasePhrycilia LimenNo ratings yet
- Early Postoperative Seizures EPS in Patients UnderDocument11 pagesEarly Postoperative Seizures EPS in Patients UnderSri Eka HandayaniNo ratings yet
- Proceedings of The 2014 Spring Meeting of The Society of British 2014Document40 pagesProceedings of The 2014 Spring Meeting of The Society of British 2014rabiatul adawiyahNo ratings yet
- Surgical Results of Persistent Fetal Vasculature: Li-Sheng Cheng, MD Hsi-Kung Kuo, MD Sue-Ann Lin, MD Ming-Lun Kuo, MDDocument7 pagesSurgical Results of Persistent Fetal Vasculature: Li-Sheng Cheng, MD Hsi-Kung Kuo, MD Sue-Ann Lin, MD Ming-Lun Kuo, MDCalvin NugrahaNo ratings yet
- cVEMP y oVEMP en ESCLEROSIS MULTIPLEDocument8 pagescVEMP y oVEMP en ESCLEROSIS MULTIPLEJaneth GuzmanNo ratings yet
- Awake CraniotomyDocument28 pagesAwake CraniotomyBeba EchevarriaNo ratings yet
- Selective AmygdalohippocampectomyDocument17 pagesSelective AmygdalohippocampectomyNeurologia homicNo ratings yet
- Structural Magnetic Resonance Imaging in Epilepsy: NeuroDocument11 pagesStructural Magnetic Resonance Imaging in Epilepsy: NeuroAnggit Adhi PrasetyaNo ratings yet
- RHS 2022Document3 pagesRHS 2022winnerfromparisNo ratings yet
- Surgical Approaches To EpilepsyDocument13 pagesSurgical Approaches To EpilepsyJames E. WalkerNo ratings yet
- Helmstaedter2004 EpilBhvr NPAspectsOfEpiSurgDocument11 pagesHelmstaedter2004 EpilBhvr NPAspectsOfEpiSurgrmindreanu979No ratings yet
- JURNALDocument6 pagesJURNALPutu erwanNo ratings yet
- Goll Witz Er 2018Document7 pagesGoll Witz Er 2018jela1309No ratings yet
- Parinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronDocument6 pagesParinaud Syndrome: Any Clinicoradiological Correlation?: L. Pollak - T. Zehavi-Dorin - A. Eyal - R. Milo - R. Huna-BaronJessica HerreraNo ratings yet
- Monic 2Document106 pagesMonic 2Life PediaNo ratings yet
- Proposal For ElectroencephalogramDocument3 pagesProposal For ElectroencephalogramHamza El-ȜfifiNo ratings yet
- Seziures: Status Epilepticus Status EpilepticusDocument2 pagesSeziures: Status Epilepticus Status EpilepticusEna PaparićNo ratings yet
- (Progress in Epileptic Disorders, Vol. 13) Solomon L. Moshé, J. Helen Cross, Linda de Vries, Douglas Nordli, Federico Vigevano-Seizures and Syndromes of PDFDocument283 pages(Progress in Epileptic Disorders, Vol. 13) Solomon L. Moshé, J. Helen Cross, Linda de Vries, Douglas Nordli, Federico Vigevano-Seizures and Syndromes of PDFWalter Huacani HuamaniNo ratings yet
- Mari 2006Document4 pagesMari 2006Nico NicoNo ratings yet
- SandasjkbdjabkdabkajsbdDocument3 pagesSandasjkbdjabkdabkajsbdM Rafif Rasyid FNo ratings yet
- Daftar Pustaka Mini ProjectDocument3 pagesDaftar Pustaka Mini ProjectMahadian Ismail NasutionNo ratings yet
- Quiz 8Document3 pagesQuiz 8DoctorSajid BuzdarNo ratings yet
- Electroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDate PDFDocument37 pagesElectroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDate PDFRobert MîndreanuNo ratings yet
- EtiologyEpilepsy2011ExpertRevNeur (Recovered)Document17 pagesEtiologyEpilepsy2011ExpertRevNeur (Recovered)ArwatiKilwowD'ctzGreenNo ratings yet
- Slides For SeizureDocument15 pagesSlides For SeizureBryan Mae H. Degorio100% (3)
- Ketogenic Diet PresentationDocument64 pagesKetogenic Diet Presentationstefanie_561186832100% (2)
- Lateralisasi Semiologi Bangkitan Epileptik Pada Epilepsi Lobus Temporal Mesial Dengan Sklerosis HipokampusDocument12 pagesLateralisasi Semiologi Bangkitan Epileptik Pada Epilepsi Lobus Temporal Mesial Dengan Sklerosis HipokampusemyNo ratings yet
- Types of SeizuresDocument3 pagesTypes of SeizuresOliver FullenteNo ratings yet
- No Nama Obat Jumlah Penggunaan Obat Harga Satuan Ket Sisa StokDocument11 pagesNo Nama Obat Jumlah Penggunaan Obat Harga Satuan Ket Sisa StokAgatha NightrayNo ratings yet
- Dve2 EcDocument18 pagesDve2 Eclegal ptkhalifiNo ratings yet
- McqepilipsyDocument3 pagesMcqepilipsyNguyen Anh TuanNo ratings yet
- Unverricht-Lundborg Disease A Case Report and LiteDocument4 pagesUnverricht-Lundborg Disease A Case Report and LiteAndreea CimpoiNo ratings yet
- Maine Epilepsy Moms Press ReleaseDocument1 pageMaine Epilepsy Moms Press ReleaseBrian BretonNo ratings yet
- Paediatrics Epileptiform DisordersDocument11 pagesPaediatrics Epileptiform DisordersayunisallehNo ratings yet
- Seizure Iscemiic StrokeDocument14 pagesSeizure Iscemiic StrokeJeli Jati AnggeriaNo ratings yet
- Daftar Judul Poster AOCN PembimbingDocument3 pagesDaftar Judul Poster AOCN PembimbingWaskitho NugrohoNo ratings yet
- Sindrome de WestDocument8 pagesSindrome de Westmaria laura ramirezNo ratings yet
- Epilepsy in Infants and ChildrenDocument6 pagesEpilepsy in Infants and ChildrenDaniela NaranjoNo ratings yet
- Neurology EMQDocument5 pagesNeurology EMQLakshya J BasumataryNo ratings yet
- Case Report Kejang NeonatusDocument12 pagesCase Report Kejang NeonatusSonya HyekyoNo ratings yet
- Soal + Pembahasan - Epilepsy and Seizure - 2Document2 pagesSoal + Pembahasan - Epilepsy and Seizure - 2jumasriNo ratings yet