Download as pdf or txt
You might also like
- 2018 Geriatric Psychiatry PDFDocument738 pages2018 Geriatric Psychiatry PDFNungki100% (10)
- Home For The Elderly CitizensDocument4 pagesHome For The Elderly CitizensJaymar PadolinaNo ratings yet
- Ambulating ClientDocument4 pagesAmbulating ClientRegineCuasSulibNo ratings yet
- Guidelines APA PDFDocument25 pagesGuidelines APA PDFPau NndNo ratings yet
- Older AdultsDocument63 pagesOlder AdultsLuis RamosNo ratings yet
- Cognitive-Behavioral Interventions With Older AdulDocument38 pagesCognitive-Behavioral Interventions With Older AdulMARIELA LIZETH VALENTE CORTEZNo ratings yet
- Military Culture Strometal Et. Al. 2012Document10 pagesMilitary Culture Strometal Et. Al. 2012Lauren RyanNo ratings yet
- A 0029328Document12 pagesA 0029328Cristina MPNo ratings yet
- Ethical-Practice-in-Geropsychology-Intro-SampleDocument8 pagesEthical-Practice-in-Geropsychology-Intro-SampleYago CarvalhoNo ratings yet
- RecommendedDocument9 pagesRecommendedMaya Putri Haryanti100% (1)
- 9p - Intellectual Disability and Mental Health - Is Psychology PreparedDocument9 pages9p - Intellectual Disability and Mental Health - Is Psychology Preparedtiagompeixoto.psiNo ratings yet
- 2014 - APA Guidelines Older AdultsDocument32 pages2014 - APA Guidelines Older AdultsQueralt BNo ratings yet
- Art. Psicología Infantil Clínica - Una Especialidad para Niños, Adolescentes y Sus Familias 1Document8 pagesArt. Psicología Infantil Clínica - Una Especialidad para Niños, Adolescentes y Sus Familias 1Henry RiveraNo ratings yet
- Child and Adolescent Psychological Assessment CurrDocument9 pagesChild and Adolescent Psychological Assessment CurrArif Erdem KöroğluNo ratings yet
- Guidelines Assessment Intervention DisabilitiesDocument61 pagesGuidelines Assessment Intervention DisabilitiesBladimir Iles ChavesNo ratings yet
- A Model For Home-Based Psychology From The Veterans Health AdministrationDocument7 pagesA Model For Home-Based Psychology From The Veterans Health AdministrationStephanie SouzaNo ratings yet
- Assessment and Treatment of Gender Dysphoria and Gender Variant Patients: A Primer For PsychiatristsDocument1 pageAssessment and Treatment of Gender Dysphoria and Gender Variant Patients: A Primer For Psychiatristssergi pascualNo ratings yet
- Test Bank For Introduction To Clinical Psychology 8 e 8th Edition Geoffrey P Kramer Douglas A Bernstein Vicky PharesDocument11 pagesTest Bank For Introduction To Clinical Psychology 8 e 8th Edition Geoffrey P Kramer Douglas A Bernstein Vicky PharesMarlyn Islam100% (40)
- Park KubzanskyDocument11 pagesPark KubzanskyJONNABEL ROQUEZNo ratings yet
- (11 V) From The Laboratory To The Therapy RoomDocument16 pages(11 V) From The Laboratory To The Therapy RoomricardorickiNo ratings yet
- Only Human: Mental Health Difficulties Among Clinical, Counseling, and School Psychology Faculty and TraineesDocument49 pagesOnly Human: Mental Health Difficulties Among Clinical, Counseling, and School Psychology Faculty and TraineescrisolarisNo ratings yet
- Geropsychology Content in Clinical TrainDocument10 pagesGeropsychology Content in Clinical TrainTheo Buana ParandaNo ratings yet
- UC San Diego Previously Published WorksDocument12 pagesUC San Diego Previously Published WorkszahoNo ratings yet
- Behaviour Research and Therapy: Alan E. KazdinDocument12 pagesBehaviour Research and Therapy: Alan E. KazdinDroguNo ratings yet
- The Abstracts of The 36th Annual Conference of The Australian Psychological SocietyDocument50 pagesThe Abstracts of The 36th Annual Conference of The Australian Psychological Societymoch.al.irsyad19No ratings yet
- Content ServerDocument9 pagesContent ServerNariman Abed Alganey AkariNo ratings yet
- Guidelines Dementia Age Related Cognitive ChangeDocument32 pagesGuidelines Dementia Age Related Cognitive ChangeFernanda Keren de PaulaNo ratings yet
- Feeny 2006 CBT For Bipolar Pilot 19719Document8 pagesFeeny 2006 CBT For Bipolar Pilot 19719shobaNo ratings yet
- Measures of Psychological Stress and Physical Health in Family Caregivers of Stroke Survivors A Literature ReviewDocument11 pagesMeasures of Psychological Stress and Physical Health in Family Caregivers of Stroke Survivors A Literature ReviewaNo ratings yet
- IndianJPsychiatry60524-4490945 122829Document25 pagesIndianJPsychiatry60524-4490945 122829EnaraNo ratings yet
- 2012 Positive Psy OverviewDocument17 pages2012 Positive Psy OverviewDivia RainaNo ratings yet
- Pottik 2007Document8 pagesPottik 2007Stijn VanheuleNo ratings yet
- CD QuestDocument20 pagesCD QuestDindini FanaiNo ratings yet
- Texto Sobre Foco No Terapeuta (4980)Document17 pagesTexto Sobre Foco No Terapeuta (4980)Fabiana H. ShimabukuroNo ratings yet
- Horan 2001Document49 pagesHoran 2001moch.al.irsyad19No ratings yet
- Bringing Psychotherapy To Primary Care: Innovations and ChallengesDocument24 pagesBringing Psychotherapy To Primary Care: Innovations and ChallengespqpnbnrmNo ratings yet
- Health Promotion With Older Adults Experiencing Mental Health Challenges: A Literature Review of Strength-Based ApproachesDocument28 pagesHealth Promotion With Older Adults Experiencing Mental Health Challenges: A Literature Review of Strength-Based ApproachesDewi AgustianiNo ratings yet
- Artigo SM 3Document10 pagesArtigo SM 3selfemanNo ratings yet
- Mental Health Diagnostic Considerations in Racial Ethnic Minority YouthDocument15 pagesMental Health Diagnostic Considerations in Racial Ethnic Minority YouthJohn BitsasNo ratings yet
- Mental Health and Palliative Care Literature ReviewDocument4 pagesMental Health and Palliative Care Literature ReviewafdtbwkhbNo ratings yet
- Hirvikoski, Et Al.j. (2015) - Cognitive Behavior Therapy-Based Psychoeducational Groups For Adults With ADHD and Their Significant OthersDocument11 pagesHirvikoski, Et Al.j. (2015) - Cognitive Behavior Therapy-Based Psychoeducational Groups For Adults With ADHD and Their Significant OthersjuanNo ratings yet
- Inpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsFrom EverandInpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsHoward H. FennNo ratings yet
- 2011 Adhd Npsy-AssessmentDocument15 pages2011 Adhd Npsy-AssessmentRoberta Finamore de AraujoNo ratings yet
- Hardaker Halcomb GriffithsBolzan Arblaster 2007Document11 pagesHardaker Halcomb GriffithsBolzan Arblaster 2007AdriánNo ratings yet
- Cashel, M.L. (2002) - Child and Adolescent Psychological Assessment. Current Clinical Practices and The Impact of Managed CareDocument8 pagesCashel, M.L. (2002) - Child and Adolescent Psychological Assessment. Current Clinical Practices and The Impact of Managed CareRicardo NarváezNo ratings yet
- Harker Washington 0250E 19146Document109 pagesHarker Washington 0250E 19146CHEE KOK SENGNo ratings yet
- JamaDocument11 pagesJamaDipin MutrejaNo ratings yet
- HHS Public Access: Mental Health Diagnostic Considerations in Racial/Ethnic Minority YouthDocument25 pagesHHS Public Access: Mental Health Diagnostic Considerations in Racial/Ethnic Minority YouthTry Wahyudi Jeremi LoLyNo ratings yet
- E144 Vol. 52 No. 6 December 2016 Selected AbstractsDocument2 pagesE144 Vol. 52 No. 6 December 2016 Selected AbstractsJos CanalesNo ratings yet
- Benefits of An Experimental Program of Equestrian Therapy For Children With ADHD PDFDocument10 pagesBenefits of An Experimental Program of Equestrian Therapy For Children With ADHD PDFJuli DeviaNo ratings yet
- 01 Taylor-Rodgers Evaluation of An Online 2014Document7 pages01 Taylor-Rodgers Evaluation of An Online 2014sushmita bhartiaNo ratings yet
- A2 Uedp2 223Document6 pagesA2 Uedp2 223arundhatisah01No ratings yet
- Intellectual DevelopmentalDocument29 pagesIntellectual DevelopmentalAnne de AndradeNo ratings yet
- Fields of PsychologyDocument14 pagesFields of Psychologyhumna naeemNo ratings yet
- Pauta Discapacidad N&ADocument29 pagesPauta Discapacidad N&APedro Y. LuyoNo ratings yet
- Chapter 4Document44 pagesChapter 4AnonimoNo ratings yet
- Prevalence and Correlates of DepressionDocument9 pagesPrevalence and Correlates of Depressioncristel.talladaNo ratings yet
- Pacha Nager o Psych Training 2010Document11 pagesPacha Nager o Psych Training 2010Theo Buana ParandaNo ratings yet
- Aging, Mental Health and Demographic Challenges For PsychotherapistsDocument8 pagesAging, Mental Health and Demographic Challenges For PsychotherapistsChristian RiveraNo ratings yet
- Videoconferencing Psychotherapy: A Systematic Review: Psychological Services May 2012Document22 pagesVideoconferencing Psychotherapy: A Systematic Review: Psychological Services May 2012juan acuñaNo ratings yet
- Sareeceguerrero-324-Litreviewfinal-Bosa 1Document7 pagesSareeceguerrero-324-Litreviewfinal-Bosa 1api-520930030No ratings yet
- Statistical Bulletin: Health Expectancies at Birth and at Age 65 in The United Kingdom, 2007-2009Document17 pagesStatistical Bulletin: Health Expectancies at Birth and at Age 65 in The United Kingdom, 2007-2009Papato KongNo ratings yet
- p95 09 1 PDFDocument196 pagesp95 09 1 PDFPapato KongNo ratings yet
- Measuring National Well-Being at What Age Is Personal Well-Being The HighestDocument6 pagesMeasuring National Well-Being at What Age Is Personal Well-Being The HighestPapato KongNo ratings yet
- M01 S09 Gender Stereotypes PDFDocument9 pagesM01 S09 Gender Stereotypes PDFPapato KongNo ratings yet
- Social Communication Assessment After Traumatic Brain Injury A Narrative Review of Innovations in Pragmatic and Discourse Assessment MethodsDocument15 pagesSocial Communication Assessment After Traumatic Brain Injury A Narrative Review of Innovations in Pragmatic and Discourse Assessment MethodsPapato KongNo ratings yet
- T ADLQMunoz NeiraSlachevskyetal2012 - PDFDocument12 pagesT ADLQMunoz NeiraSlachevskyetal2012 - PDFPapato KongNo ratings yet
- Computational Neuroscience: Rajesh P. N. Rao Adrienne Fairhall University of Washington, Seattle, USADocument7 pagesComputational Neuroscience: Rajesh P. N. Rao Adrienne Fairhall University of Washington, Seattle, USAPapato KongNo ratings yet
- House Democratic Caucus Task Force On Aging and Families LTR To Biden Harris Transition - Geriatrician To COVID Advisory BoardDocument2 pagesHouse Democratic Caucus Task Force On Aging and Families LTR To Biden Harris Transition - Geriatrician To COVID Advisory BoardPeter SullivanNo ratings yet
- Late Life and Neurocognitive DisordersDocument24 pagesLate Life and Neurocognitive DisordersJonnaNo ratings yet
- Health Sciences 2711B 2011 - Health Issues in AgingDocument8 pagesHealth Sciences 2711B 2011 - Health Issues in AgingJillKellyNo ratings yet
- Posterior Cortical AtrophyDocument9 pagesPosterior Cortical AtrophyAnonymous zxTFUoqzklNo ratings yet
- Ebp PresentationDocument12 pagesEbp Presentationapi-267985804No ratings yet
- Drug Study HaldolDocument2 pagesDrug Study HaldolGracia EvangelistaNo ratings yet
- UTI Treatment Guidelines PDFDocument5 pagesUTI Treatment Guidelines PDFMuhammad IhsanuddinNo ratings yet
- TMH ResumeDocument2 pagesTMH Resumeapi-257873078No ratings yet
- Nursing InterventionsDocument1 pageNursing InterventionsTancred UyNo ratings yet
- RLE NCMB 314-M2-CU 9 Respiratory ChangesDocument6 pagesRLE NCMB 314-M2-CU 9 Respiratory ChangesJordz PlaciNo ratings yet
- Biomechanics and Clinical Implications of Complete Edentulous StateDocument4 pagesBiomechanics and Clinical Implications of Complete Edentulous StateDorobantuMihaiGabiNo ratings yet
- Assessment Constipation PDFDocument6 pagesAssessment Constipation PDFDennis CobbNo ratings yet
- Mood Affect....Document3 pagesMood Affect....Michael ReidNo ratings yet
- NFDN 2003Document2 pagesNFDN 2003api-319220519No ratings yet
- Tpo Ward BMDocument3 pagesTpo Ward BMAhl A PurujiNo ratings yet
- Daftar Pustaka 13 Permasalahan Terkait Obat Antihipertensi Pada Pasien Usia Lanjut Di Poli Geriatri RSUD DR - Soetomo PDFDocument6 pagesDaftar Pustaka 13 Permasalahan Terkait Obat Antihipertensi Pada Pasien Usia Lanjut Di Poli Geriatri RSUD DR - Soetomo PDFDave AbrahamNo ratings yet
- What Is CaregivingDocument3 pagesWhat Is CaregivingjasmineNo ratings yet
- PermethrinDocument3 pagesPermethrinaficoNo ratings yet
- Escala Internacional de Demencia HIVDocument8 pagesEscala Internacional de Demencia HIVctobonaNo ratings yet
- Assessment of Older People 2: Assessing The Physical DomainDocument5 pagesAssessment of Older People 2: Assessing The Physical DomainJastine SabornidoNo ratings yet
- Vascular Dementia, With Lacunar StrokeDocument28 pagesVascular Dementia, With Lacunar StrokeTimotius Wira YudhaNo ratings yet
- NeuropsychiatricDocument18 pagesNeuropsychiatricSamuel JohnsonNo ratings yet
- J Neurol Neurosurg Psychiatry 1998 Royall 588 94Document8 pagesJ Neurol Neurosurg Psychiatry 1998 Royall 588 9454321000No ratings yet
- Gastritis Erosif PatofisiologiDocument3 pagesGastritis Erosif PatofisiologiLargactil CpzNo ratings yet
- Nursing Manangment of Older PersonDocument5 pagesNursing Manangment of Older PersonRaiden VizcondeNo ratings yet
- Save The Date: 94th Anniversary DinnerDocument4 pagesSave The Date: 94th Anniversary DinnerthehebrewhomeNo ratings yet
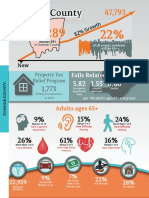
- Sumner County Senior StatisticsDocument1 pageSumner County Senior StatisticsJen ToddNo ratings yet
- VirtualSx Event (Invite-Only)Document2 pagesVirtualSx Event (Invite-Only)SexRecoveryNo ratings yet