Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- Lore of Running 4th Ed PDFDocument946 pagesLore of Running 4th Ed PDFwooyann67% (12)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cardiac Electrophysiology Board Review and Self-AssessmentDocument335 pagesCardiac Electrophysiology Board Review and Self-AssessmentAndonis Angelov100% (1)
- @anesthesia Books 2019 Hensley's PDFDocument1,175 pages@anesthesia Books 2019 Hensley's PDFAurora Herrera100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Physiology. Hrd.Document549 pagesPhysiology. Hrd.Sʌɩĸʌt PʌʋɭNo ratings yet
- Chapter 9 Cardiac MuscleDocument5 pagesChapter 9 Cardiac MuscleYheng GaosaiiNo ratings yet
- CNS Tract SummaryDocument2 pagesCNS Tract SummaryAlexaNo ratings yet
- Heart MurmursDocument242 pagesHeart MurmursAlexaNo ratings yet
- Ascending Tracts MENMONIC AND SummaryDocument2 pagesAscending Tracts MENMONIC AND SummaryAlexaNo ratings yet
- Corticospinal Tract Practice QuestionsDocument2 pagesCorticospinal Tract Practice QuestionsAlexaNo ratings yet
- Golgi Complex,: Secretion and Protein TransportDocument46 pagesGolgi Complex,: Secretion and Protein TransportAlexaNo ratings yet
- Pocket ConstitutionDocument52 pagesPocket ConstitutionAlexaNo ratings yet
- Budgeting Basics: Managing Your Money During The Lean YearsDocument2 pagesBudgeting Basics: Managing Your Money During The Lean YearsAlexaNo ratings yet
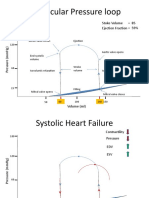
- Ventricular Pressure LoopDocument8 pagesVentricular Pressure LoopAlexaNo ratings yet
- Cell DivisionDocument41 pagesCell DivisionAlexaNo ratings yet
- Quirce Et Al-1998-Clinical & Experimental AllergyDocument8 pagesQuirce Et Al-1998-Clinical & Experimental AllergyAlexaNo ratings yet
- 322 Fall 2014 Exam 2 KeyDocument7 pages322 Fall 2014 Exam 2 KeyAlexaNo ratings yet
- Accuracy Percision LabDocument2 pagesAccuracy Percision LabAlexaNo ratings yet
- CH 13 PPT Lecture Bio1350Document17 pagesCH 13 PPT Lecture Bio1350AlexaNo ratings yet
- Jce 2007 P 0124 WDocument25 pagesJce 2007 P 0124 WAlexaNo ratings yet
- Creatinin and CaffeineDocument33 pagesCreatinin and CaffeineNina RianaNo ratings yet
- MUSCLE 4 NursingDocument67 pagesMUSCLE 4 NursingCHALIE MEQUNo ratings yet
- Inotropic AgentsDocument5 pagesInotropic AgentsanaeshklNo ratings yet
- Muscle PhysiologyDocument50 pagesMuscle PhysiologyJoyce Adjei-boateng100% (1)
- Cardiolab NotesDocument14 pagesCardiolab NotesEmmanuel MensahNo ratings yet
- Berg 8e Testbank Chapter13 PDFDocument13 pagesBerg 8e Testbank Chapter13 PDFbenin2No ratings yet
- Muscle Tissue OutlineDocument4 pagesMuscle Tissue OutlinePeachy PieNo ratings yet
- Physio Pretest WordDocument143 pagesPhysio Pretest WordJanie-Vi Gorospe67% (3)
- Cambridge International AS & A Level: BIOLOGY 9700/43Document28 pagesCambridge International AS & A Level: BIOLOGY 9700/43Weirdo PsychoNo ratings yet
- Explain Why The Increased Release of K+ From Muscles During High Intensity Exercise May Cause FatigueDocument3 pagesExplain Why The Increased Release of K+ From Muscles During High Intensity Exercise May Cause Fatiguenganleo5801No ratings yet
- 2Document17 pages2이어진No ratings yet
- Neuromuscular JunctionDocument6 pagesNeuromuscular JunctionManish GujjarNo ratings yet
- Cardiac Action PotentialDocument9 pagesCardiac Action PotentialswennecaNo ratings yet
- P2 2019 SMK Methodist PDFDocument11 pagesP2 2019 SMK Methodist PDFBryanLeeChienYungNo ratings yet
- Dongsheng Duan, Jerry R. Mendell - Muscle Gene Therapy-Springer International Publishing (2019)Document804 pagesDongsheng Duan, Jerry R. Mendell - Muscle Gene Therapy-Springer International Publishing (2019)Sorin DinuNo ratings yet
- 4.1.1 Draw and Label A Diagram of A Motor Unit.: Movement AnalysisDocument30 pages4.1.1 Draw and Label A Diagram of A Motor Unit.: Movement AnalysisMaggie-Louise BellamyNo ratings yet
- Insecticide Mode of ActionDocument76 pagesInsecticide Mode of ActionPheromonalNo ratings yet
- Physiology of The Muscular System: Language of Science Chapter OutlineDocument34 pagesPhysiology of The Muscular System: Language of Science Chapter OutlinedevaaNo ratings yet
- Sarcopenia - Mechanisms and TreatmentsDocument7 pagesSarcopenia - Mechanisms and TreatmentsshodhgangaNo ratings yet
- Cardiac Function in Heart Failure-The Role of Calcium Cycling PDFDocument8 pagesCardiac Function in Heart Failure-The Role of Calcium Cycling PDFJosie Enad Purlares CelyonNo ratings yet
- 3D. Muscle TissueDocument47 pages3D. Muscle Tissuejaf123xyNo ratings yet
- 397 - Musculoskeletal Physiology) Smooth MuscleDocument5 pages397 - Musculoskeletal Physiology) Smooth Musclevkpremiyahoo.comNo ratings yet
- Pathophysiology On ArrhythmiaDocument34 pagesPathophysiology On ArrhythmiaYhr Yh100% (1)
- Falla Cardiaca 2013Document20 pagesFalla Cardiaca 2013Diego Andrés Mejía VascoNo ratings yet
- Official Bank-MusclesDocument27 pagesOfficial Bank-MusclesEbtihal AlharthiNo ratings yet