Download as pdf or txt
You might also like
- ADHD Test DIVA 5-0Document12 pagesADHD Test DIVA 5-0Augustin Gireada100% (4)
- Hooper Visual Organization Test PsychometricDocument10 pagesHooper Visual Organization Test PsychometricJosiane AlmeidaNo ratings yet
- Slides For S4 Advanced Available To Promise aATPDocument38 pagesSlides For S4 Advanced Available To Promise aATPMurali KrishnanNo ratings yet
- CURE Counseling & Assessment Training Centre: Instructions For Completing The PDQ-4 AssessmentDocument6 pagesCURE Counseling & Assessment Training Centre: Instructions For Completing The PDQ-4 AssessmentG. S.No ratings yet
- Accelerated ART Intro & Research Base Kip PPT 7-19-2017Document44 pagesAccelerated ART Intro & Research Base Kip PPT 7-19-2017scmesser0% (1)
- Effectiveness of PTSD TreatmentsDocument63 pagesEffectiveness of PTSD TreatmentsTariq J Faridi100% (1)
- Bessel Van Der KolkDocument49 pagesBessel Van Der Kolkjane100% (1)
- 1993 - AndrewsDocument11 pages1993 - AndrewsG. S.100% (1)
- CBT For Bipolar Disorder Slide Set For TeachingDocument50 pagesCBT For Bipolar Disorder Slide Set For TeachingZ 'No ratings yet
- Price Investigation of An Abbreviated 4 and 8 Item Version of The PTSD Checklist 5Document13 pagesPrice Investigation of An Abbreviated 4 and 8 Item Version of The PTSD Checklist 5aranza.guphNo ratings yet
- Prolonged Exposure Sessions With 20-MinuteDocument11 pagesProlonged Exposure Sessions With 20-MinutejlbermudezcNo ratings yet
- SSRN Id3550054Document23 pagesSSRN Id3550054Oscar CastañedaNo ratings yet
- CBT For Bipolar Disorder-Set Available For TeachingDocument50 pagesCBT For Bipolar Disorder-Set Available For Teachingjacqueline.n.britoNo ratings yet
- Foa 2013Document8 pagesFoa 2013Rituparna SamantarayNo ratings yet
- The Prevalence of Post Traumatic Stress Disorder Among Couples at PCEA Churches, Nairobi, KenyaDocument7 pagesThe Prevalence of Post Traumatic Stress Disorder Among Couples at PCEA Churches, Nairobi, KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Estres Agudo Bryant Et Al (2008)Document9 pagesEstres Agudo Bryant Et Al (2008)Eleoner RamirezNo ratings yet
- Articles Efficacy of EMDR Therapy For Children With PTSD: A Review of The LiteratureDocument19 pagesArticles Efficacy of EMDR Therapy For Children With PTSD: A Review of The LiteratureNerea F GNo ratings yet
- Guia Clinica DcaDocument11 pagesGuia Clinica DcaCaty PrietoNo ratings yet
- Treatment of Acute Stress DisorderDocument9 pagesTreatment of Acute Stress DisorderAlessandra LacerdaNo ratings yet
- Correlates and Predictors of Selfharm in A Prospective Sample of Sexually Assaulted AdolescentsDocument13 pagesCorrelates and Predictors of Selfharm in A Prospective Sample of Sexually Assaulted AdolescentsManya DhuparNo ratings yet
- 05 - Trauma Reactivation Under The Influence of Propranolol An Examination of Clinical PredictorsDocument10 pages05 - Trauma Reactivation Under The Influence of Propranolol An Examination of Clinical PredictorsLauraNo ratings yet
- Journal of Traumatic Stress - 2020 - Unterhitzenberger - Posttraumatic Stress Disorder and Childhood Traumatic Loss ADocument10 pagesJournal of Traumatic Stress - 2020 - Unterhitzenberger - Posttraumatic Stress Disorder and Childhood Traumatic Loss AAso Forenses S.A.SNo ratings yet
- Cognitive Function Following Breast Cancer TreatmentDocument4 pagesCognitive Function Following Breast Cancer TreatmentFrancisco MartinezNo ratings yet
- Family Response To Critical Illness: Postintensive Care Syndrome-FamilyDocument7 pagesFamily Response To Critical Illness: Postintensive Care Syndrome-FamilyPriscila FreitasNo ratings yet
- The Hidden Price and Possible Benefit of Repeated Traumatic ExposureDocument8 pagesThe Hidden Price and Possible Benefit of Repeated Traumatic ExposureafifahayestinapelinggaNo ratings yet
- Trauma Reactivation Under The InfluenceDocument9 pagesTrauma Reactivation Under The InfluenceHypnotica FranceNo ratings yet
- Annotated Bibliography 1. Depression and Anxiety - 2021 - Gramlich - Psychophysiology During Exposure To Trauma Memories Comparative Effects ofDocument13 pagesAnnotated Bibliography 1. Depression and Anxiety - 2021 - Gramlich - Psychophysiology During Exposure To Trauma Memories Comparative Effects offatimanagehNo ratings yet
- PTSD 1Document12 pagesPTSD 1sofiaNo ratings yet
- MDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDDocument8 pagesMDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDKayla GreenstienNo ratings yet
- Working Memory in Parkinson's Disease: The Effects of Depression and Side of Onset of Motor SymptomsDocument11 pagesWorking Memory in Parkinson's Disease: The Effects of Depression and Side of Onset of Motor SymptomsCatarina C.No ratings yet
- Virtual Reality Exposure Therapy For Social Anxiety Disorder: A Systematic Review and Meta-AnalysisDocument11 pagesVirtual Reality Exposure Therapy For Social Anxiety Disorder: A Systematic Review and Meta-AnalysisJazSa BerkahNo ratings yet
- The Effectiveness of Narrative Exposure Therapy With TraumatisedDocument8 pagesThe Effectiveness of Narrative Exposure Therapy With TraumatisedhNo ratings yet
- Results and DiscussionsDocument12 pagesResults and DiscussionsElla Tricia AquinoNo ratings yet
- Psychometrics of The Child PTSD Symptom Scale For DSM-5 For Trauma-Exposed Children and AdolescentsDocument10 pagesPsychometrics of The Child PTSD Symptom Scale For DSM-5 For Trauma-Exposed Children and AdolescentsRodolfo Preciado FabiánNo ratings yet
- Treating PTSD in Rape SurvivorsDocument11 pagesTreating PTSD in Rape Survivorsapi-253791196No ratings yet
- Fpsyg 11 00896Document12 pagesFpsyg 11 00896Hector OrgenaneroNo ratings yet
- Trauma Releasing Exercises TRE For PTSD41Document9 pagesTrauma Releasing Exercises TRE For PTSD41Vazta Mirta0% (1)
- Depression in Comorbid OCD and PTSDDocument6 pagesDepression in Comorbid OCD and PTSDnbookman1990No ratings yet
- Sywbds SDocument19 pagesSywbds SGustavoNo ratings yet
- General Papers: Borderline Personality Disorder and Substance Abuse: Consequences of ComorbidityDocument6 pagesGeneral Papers: Borderline Personality Disorder and Substance Abuse: Consequences of ComorbidityLina RodríguezNo ratings yet
- YBOCS AdultiDocument7 pagesYBOCS AdultiFabi kNo ratings yet
- 19 Buttner2013 Article ExaminationOfPremenstrualSymptDocument7 pages19 Buttner2013 Article ExaminationOfPremenstrualSymptraja yasminNo ratings yet
- Artículo EstrésDocument8 pagesArtículo EstrésMavah7No ratings yet
- Original Research Article First-Episode Psychosis and The Role of The Psychiatric ConsultantDocument4 pagesOriginal Research Article First-Episode Psychosis and The Role of The Psychiatric ConsultantJagdishVankarNo ratings yet
- Nhs 12283Document8 pagesNhs 12283maithakeloayNo ratings yet
- Childhood PTSDDocument10 pagesChildhood PTSDCaramel GazelleNo ratings yet
- NCDH - Influence of Psychological Response On Survival in Breast Cancer - A Population-Based Cohort Study - BBYHDPN3-Kim XuanDocument6 pagesNCDH - Influence of Psychological Response On Survival in Breast Cancer - A Population-Based Cohort Study - BBYHDPN3-Kim XuanNguyễn Tấn PhúNo ratings yet
- Journal of Affective DisordersDocument8 pagesJournal of Affective DisordersNerea F GNo ratings yet
- TEC y PsiquiatríaDocument15 pagesTEC y PsiquiatríaCarolina MuñozNo ratings yet
- Does Motivation Impact OCD Symptom Severity? An Exploration of Longitudinal EffectsDocument14 pagesDoes Motivation Impact OCD Symptom Severity? An Exploration of Longitudinal EffectsLaura HdaNo ratings yet
- Evidence-Based Treatment For Adult Women With Child Abuse-Related Complex PTSD: A Quantitative ReviewDocument19 pagesEvidence-Based Treatment For Adult Women With Child Abuse-Related Complex PTSD: A Quantitative ReviewRichard millsNo ratings yet
- Stress Among Charge NursesDocument10 pagesStress Among Charge NursesRey AllanNo ratings yet
- Validation Study of A Portuguese Version of The Hospital Anxiety and Depression ScaleDocument15 pagesValidation Study of A Portuguese Version of The Hospital Anxiety and Depression ScaleNeiler OverpowerNo ratings yet
- Cancers 12 03000Document13 pagesCancers 12 03000Gary LheureuxNo ratings yet
- Depression and Anxiety - 2022 - Gutner - A Pilot Randomized Effectiveness Trial of The Unified Protocol in Trauma ExposedDocument11 pagesDepression and Anxiety - 2022 - Gutner - A Pilot Randomized Effectiveness Trial of The Unified Protocol in Trauma ExposedCristina Alarcón RuedaNo ratings yet
- Infantile Marfan Syndrome in A Korean Tertiary Referral CenterDocument6 pagesInfantile Marfan Syndrome in A Korean Tertiary Referral CenterLoretta SaphiraNo ratings yet
- Meta-Analysis of Trauma-Focused Cognitive Behavioral Therapy For Treating PTSD and Co-Occurring Depression Among Children and AdolescentsDocument15 pagesMeta-Analysis of Trauma-Focused Cognitive Behavioral Therapy For Treating PTSD and Co-Occurring Depression Among Children and AdolescentsRoman ClaudiaNo ratings yet
- Special Issue Complex Trauma Oct 2006 JTS1Document12 pagesSpecial Issue Complex Trauma Oct 2006 JTS1gabanton666No ratings yet
- Conceptualization of PTSD From The Vietnam War To Current Conflicts and Beyond 1522 4821 1000278Document3 pagesConceptualization of PTSD From The Vietnam War To Current Conflicts and Beyond 1522 4821 1000278Teofztogo Palsimon100% (1)
- School Bullying ArticlesDocument8 pagesSchool Bullying ArticlesBhima DewanNo ratings yet
- The Effectiveness of Mindfulness Based Cognitive Behavioural Therapy (MBCBT) in The Treatment of PTSD Among Couples at PCEA Churches, Nairobi, KenyaDocument9 pagesThe Effectiveness of Mindfulness Based Cognitive Behavioural Therapy (MBCBT) in The Treatment of PTSD Among Couples at PCEA Churches, Nairobi, KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- APJCP - Volume 20 - Issue 10 - Pages 2903-2908Document6 pagesAPJCP - Volume 20 - Issue 10 - Pages 2903-2908Guillermo MoranteNo ratings yet
- Beyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDDocument9 pagesBeyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDmakolla007No ratings yet
- Key Performance Indicators For Australian Mental Health Court Liaison ServicesDocument5 pagesKey Performance Indicators For Australian Mental Health Court Liaison ServicesG. S.No ratings yet
- Changing Mental Health Gatekeeping: Effects On Performance IndicatorsDocument17 pagesChanging Mental Health Gatekeeping: Effects On Performance IndicatorsG. S.No ratings yet
- 1988 - CramerDocument23 pages1988 - CramerG. S.No ratings yet
- HSCL ArabicDocument3 pagesHSCL ArabicG. S.No ratings yet
- 2010 - Porcerelli Et Al.Document7 pages2010 - Porcerelli Et Al.G. S.No ratings yet
- Composing A Core Set of Performance Indicators For Public Mental Health Care: A Modified Delphi ProcedureDocument11 pagesComposing A Core Set of Performance Indicators For Public Mental Health Care: A Modified Delphi ProcedureG. S.No ratings yet
- Bsi 18Document1 pageBsi 18G. S.No ratings yet
- APA DSM5TR Level2AngerAdultDocument3 pagesAPA DSM5TR Level2AngerAdultG. S.No ratings yet
- Taylor 2016Document15 pagesTaylor 2016G. S.No ratings yet
- Baker 1999Document3 pagesBaker 1999G. S.No ratings yet
- Self-Report Instrument For: Development of A Brief, MultidimensionalDocument18 pagesSelf-Report Instrument For: Development of A Brief, MultidimensionalG. S.No ratings yet
- APA DSM5TR Level2RepetitiveThoughtsAndBehaviorsAdultDocument3 pagesAPA DSM5TR Level2RepetitiveThoughtsAndBehaviorsAdultG. S.No ratings yet
- Clinician-Administered Rating Scale For Mania (CARS-M)Document6 pagesClinician-Administered Rating Scale For Mania (CARS-M)G. S.No ratings yet
- MHA - Healthcare Administration - Executive TrackDocument1 pageMHA - Healthcare Administration - Executive TrackG. S.No ratings yet
- Qids CDocument2 pagesQids CG. S.No ratings yet
- Gpsych 2019 December 32 6 Inline Supplementary Material 1Document1 pageGpsych 2019 December 32 6 Inline Supplementary Material 1G. S.No ratings yet
- Manic State Rating Scale (MSRS) : VersionsDocument1 pageManic State Rating Scale (MSRS) : VersionsG. S.No ratings yet
- Ybocs Ii SRDocument6 pagesYbocs Ii SRG. S.No ratings yet
- Development and Psychometric Evaluation of The Yale-Brown Obsessive-Compulsive Scale-Second EditionDocument10 pagesDevelopment and Psychometric Evaluation of The Yale-Brown Obsessive-Compulsive Scale-Second EditionG. S.No ratings yet
- EMHA Brochure Digital - VFDocument8 pagesEMHA Brochure Digital - VFG. S.No ratings yet
- UWM MHA-guide-to-application-processDocument1 pageUWM MHA-guide-to-application-processG. S.No ratings yet
- The Six Key Themes of Perfectionism: 1. Not Good EnoughDocument1 pageThe Six Key Themes of Perfectionism: 1. Not Good EnoughG. S.No ratings yet
- What Is Unhealthy Perfectionism?: © Russ Harris, 2023Document1 pageWhat Is Unhealthy Perfectionism?: © Russ Harris, 2023G. S.No ratings yet
- 2002 - Ali Et Al.Document9 pages2002 - Ali Et Al.G. S.No ratings yet
- Personality Questi Ire: Appendix LDocument11 pagesPersonality Questi Ire: Appendix LG. S.No ratings yet
- 2005 - Chabrol Et Al.Document3 pages2005 - Chabrol Et Al.G. S.No ratings yet
- An Action Research ProposalDocument21 pagesAn Action Research ProposalRICHEL MANGMANGNo ratings yet
- تفسير الاحلام محمد بن سيرين tafsir al ahlamDocument4 pagesتفسير الاحلام محمد بن سيرين tafsir al ahlamJawwad Hussain100% (2)
- 95 - A53 Z1 9 0020 B en - Technical DocumentationDocument184 pages95 - A53 Z1 9 0020 B en - Technical DocumentationSyed Mohammad NaveedNo ratings yet
- Ryan-James Papworth: Address: 69 Thetford Road Brandon IP27 0BZ Mobile: 07825705487 Personal StatmentDocument10 pagesRyan-James Papworth: Address: 69 Thetford Road Brandon IP27 0BZ Mobile: 07825705487 Personal Statmentryan482No ratings yet
- STAT 330 Extra Problems - Chapters 1 To 5Document6 pagesSTAT 330 Extra Problems - Chapters 1 To 5Matt WangNo ratings yet
- TCAEMM EmptyvaluesdocumentDocument689 pagesTCAEMM EmptyvaluesdocumentJithinNo ratings yet
- Lecture 1: MEMS Motivation: Prasanna S. Gandhi Assistant ProfessorDocument36 pagesLecture 1: MEMS Motivation: Prasanna S. Gandhi Assistant ProfessorAditya Narayan SahooNo ratings yet
- History of Cities and City PlanningDocument8 pagesHistory of Cities and City PlanningmahnoorNo ratings yet
- Psychrometric Process (With Chart) - Air Conditioning - Thermal EngineeringDocument9 pagesPsychrometric Process (With Chart) - Air Conditioning - Thermal Engineeringrobelyn.sudariaNo ratings yet
- College Students' Need For Cognition, Academic Motivation, Performance, and Well-Being 2012Document19 pagesCollege Students' Need For Cognition, Academic Motivation, Performance, and Well-Being 2012Vania RamirezNo ratings yet
- ISSMGE Bulletin Volume 4 Issue1Document52 pagesISSMGE Bulletin Volume 4 Issue1bm-naceurNo ratings yet
- Benefits of Shabad Guru - 3HO FoundationDocument5 pagesBenefits of Shabad Guru - 3HO FoundationBorisNo ratings yet
- AP&AR VAT Return ReportDocument7 pagesAP&AR VAT Return ReportMohd Imran AhmedNo ratings yet
- "Great Nationalism, Little Nationalism and Problem of Integration: A Tentative View" by Amalendu GuhaDocument4 pages"Great Nationalism, Little Nationalism and Problem of Integration: A Tentative View" by Amalendu GuhaEl BiswajitNo ratings yet
- Performance of The Double-Cross Tomato Hybrids FroDocument13 pagesPerformance of The Double-Cross Tomato Hybrids FroAgus TinusNo ratings yet
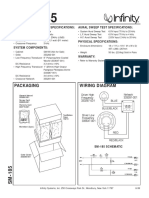
- Infinity sm-185Document2 pagesInfinity sm-185Bmwmotorsport GabriNo ratings yet
- 5E Lesson Plan: Engagement: Day 1 &2Document3 pages5E Lesson Plan: Engagement: Day 1 &2api-240269666No ratings yet
- Humes IntentionsDocument174 pagesHumes IntentionsmikeNo ratings yet
- Tinywow - PSME 100-3 S + WFI LOOP PHARMA STILL MULTIPLE EFFECT + DISTRIBUTION 2.2 - 5949770Document6 pagesTinywow - PSME 100-3 S + WFI LOOP PHARMA STILL MULTIPLE EFFECT + DISTRIBUTION 2.2 - 5949770Yacine MokhtariNo ratings yet
- C1812 Display Logger DatasheetDocument4 pagesC1812 Display Logger DatasheetselnemaisNo ratings yet
- 28 TerminalsDocument42 pages28 TerminalsAlin FazacasNo ratings yet
- Acknowledgement: Display System For Amount of Seats Available Free in LibraryDocument24 pagesAcknowledgement: Display System For Amount of Seats Available Free in LibraryHaymanot LegesseNo ratings yet
- Mathematics (51) : Class XDocument5 pagesMathematics (51) : Class XdhruvNo ratings yet
- Data Analytics Using R-Programming NotesDocument100 pagesData Analytics Using R-Programming NotesSHIKHAR MOHANNo ratings yet
- Comparison of Bond Strength Between A Conventional Resin Adhesive and A Resin-Modified Glass Ionomer Adhesive: An in Vitro and in Vivo Study.Document2 pagesComparison of Bond Strength Between A Conventional Resin Adhesive and A Resin-Modified Glass Ionomer Adhesive: An in Vitro and in Vivo Study.Reliance Orthodontic ProductsNo ratings yet
- R-LSK 211Document9 pagesR-LSK 211neomakabe14No ratings yet
- International Ego State Therapy Bibliography Sept 2014Document35 pagesInternational Ego State Therapy Bibliography Sept 2014RudolfSianto100% (1)
- Confidential: High Efficiency Synchronous Rectifier Boost ConverterDocument15 pagesConfidential: High Efficiency Synchronous Rectifier Boost ConverterkingNo ratings yet