
Grozdev 2014
Grozdev 2014
You might also like
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocument4 pagesPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Acute and Chronic Inflammation MCQDocument2 pagesAcute and Chronic Inflammation MCQBeda Malecdan73% (30)
- Psoriasis and Comorbid DeseaseDocument67 pagesPsoriasis and Comorbid DeseaseAl NaifNo ratings yet
- SolDocument10 pagesSolTsigereda AberaNo ratings yet
- Psoriasis and Risk of Cardiovascular Disease: Case Report and DiscussionDocument4 pagesPsoriasis and Risk of Cardiovascular Disease: Case Report and DiscussionAbhishek KushwahNo ratings yet
- Update ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentDocument35 pagesUpdate ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentSudeesh KumarNo ratings yet
- Ahri Proposal 2Document28 pagesAhri Proposal 2Tsigereda AberaNo ratings yet
- Jcad 12 6 46 PDFDocument9 pagesJcad 12 6 46 PDFRatu TriaNo ratings yet
- Psoriasis and Dermatitis AtopicDocument11 pagesPsoriasis and Dermatitis AtopicsayasajaNo ratings yet
- Psoriasis NATURE AYFinlayDocument48 pagesPsoriasis NATURE AYFinlayMelly SyafridaNo ratings yet
- Psoriasis Carries An Increased Risk of Venous Thromboembolism: A Danish Nationwide Cohort StudyDocument6 pagesPsoriasis Carries An Increased Risk of Venous Thromboembolism: A Danish Nationwide Cohort StudyAnonymous 1bEPjKNo ratings yet
- Psoriasis and Vascular Disease: An Unsolved Mystery: ReviewDocument6 pagesPsoriasis and Vascular Disease: An Unsolved Mystery: ReviewkendinceNo ratings yet
- The Effect of Inflammation and Infection On Lipids and LipoproteinsDocument46 pagesThe Effect of Inflammation and Infection On Lipids and Lipoproteinshani akbarNo ratings yet
- Wijsenbeek2015 Treatment of SarcoidosisDocument17 pagesWijsenbeek2015 Treatment of SarcoidosisJohan ArocaNo ratings yet
- TB and PADDocument7 pagesTB and PADdicky wahyudiNo ratings yet
- Tuberculosis and Diabetes Mellitus - An Underappreciated AssociationDocument9 pagesTuberculosis and Diabetes Mellitus - An Underappreciated AssociationNajla rayNo ratings yet
- LEATRACHRER REVIEW TsiDocument22 pagesLEATRACHRER REVIEW TsiTsigereda AberaNo ratings yet
- Clinical Manifestations and Diagnosis of Raynaud Phenomenon - UpToDateDocument29 pagesClinical Manifestations and Diagnosis of Raynaud Phenomenon - UpToDateMarcos Torchia EstebanNo ratings yet
- Chronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With SepsisDocument8 pagesChronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With Sepsisida ayu agung WijayantiNo ratings yet
- Psoriasis and ComorbiditiesDocument8 pagesPsoriasis and ComorbiditiesIvanWinardyNo ratings yet
- EMTC Ortegahernandez2012 PDFDocument12 pagesEMTC Ortegahernandez2012 PDFGabriel CuadrosNo ratings yet
- Gelfand 2012Document5 pagesGelfand 2012gyyygNo ratings yet
- Bur FieldDocument6 pagesBur FieldNexi anessaNo ratings yet
- Yang LengkapDocument9 pagesYang LengkapauliyasaumaNo ratings yet
- Coronavirus Disease 2019 and Cardiovascular SystemDocument19 pagesCoronavirus Disease 2019 and Cardiovascular SystemAlif riadiNo ratings yet
- Stroke As A Potential Complication of COVID-19-Associated Coagulopathy: A Narrative and Systematic Review of The LiteratureDocument11 pagesStroke As A Potential Complication of COVID-19-Associated Coagulopathy: A Narrative and Systematic Review of The LiteraturedenisNo ratings yet
- Epidemiology of Peripheral Artery Disease: Narrative ReviewDocument15 pagesEpidemiology of Peripheral Artery Disease: Narrative ReviewRumah Sakit J. H. Awaloei ManadoNo ratings yet
- COVID 19: Is There A Link Between The Course of Infection and Pharmacological Agents in Diabetes?Document8 pagesCOVID 19: Is There A Link Between The Course of Infection and Pharmacological Agents in Diabetes?Marcela MahechaNo ratings yet
- Brauchli Et Al-2008-British Journal of Dermatology Psoriasis and The Risk of Incident Diabetes MellitusDocument7 pagesBrauchli Et Al-2008-British Journal of Dermatology Psoriasis and The Risk of Incident Diabetes Mellitussaputri rizkaNo ratings yet
- 38 Reaserch South AfricaDocument6 pages38 Reaserch South AfricaTsigereda AberaNo ratings yet
- All-Cause and Cause-Specific Mortality in Psoriasis: A Systematic Review and Meta-AnalysisDocument12 pagesAll-Cause and Cause-Specific Mortality in Psoriasis: A Systematic Review and Meta-AnalysisRielz ThereaperzNo ratings yet
- Manuscript Category: Review: Version of Record Doi: 10.1111/JDI.13326Document30 pagesManuscript Category: Review: Version of Record Doi: 10.1111/JDI.13326Marcela MahechaNo ratings yet
- The Bidirectional Relationship Between TuberculosiDocument7 pagesThe Bidirectional Relationship Between TuberculosiJunita Nelly Esther JosephNo ratings yet
- Zozulinska, 2006Document5 pagesZozulinska, 2006wanda oktariaNo ratings yet
- NIH Public Access: Metabolic Syndrome in Patients With Psoriatic DiseaseDocument8 pagesNIH Public Access: Metabolic Syndrome in Patients With Psoriatic DiseaseFEISAL HILMAN -No ratings yet
- JCM 10 01798Document20 pagesJCM 10 01798Asad NawazNo ratings yet
- Methotrexate Reduces The Occurrence of Cerebrovascular Events Among Taiwanese Psoriatic Patients: A Nationwide Population-Based StudyDocument4 pagesMethotrexate Reduces The Occurrence of Cerebrovascular Events Among Taiwanese Psoriatic Patients: A Nationwide Population-Based StudyHermayudiNo ratings yet
- Chronic Obstructive Pulmonary Disease and Diabetes MellitusDocument19 pagesChronic Obstructive Pulmonary Disease and Diabetes MellitusMirza RisqaNo ratings yet
- Type Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Document2 pagesType Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Akreditasi InternaNo ratings yet
- A Review of COVID 19 Vaccines and Major Considerations For Diabetic Patients. Biotechnology and Applied BiochemistryDocument22 pagesA Review of COVID 19 Vaccines and Major Considerations For Diabetic Patients. Biotechnology and Applied Biochemistryimamsantos1191No ratings yet
- Diabetes and Sepsis Outcomes - It Is Not All Bad News: CommentaryDocument2 pagesDiabetes and Sepsis Outcomes - It Is Not All Bad News: CommentaryYoery SadewoNo ratings yet
- Cardiovascular Disease and Its Relationship With Chronic Kidney DiseaseDocument9 pagesCardiovascular Disease and Its Relationship With Chronic Kidney Diseasetrinda ireneNo ratings yet
- Psoriasis With Vascular DiseaseDocument4 pagesPsoriasis With Vascular Diseasemegh dutNo ratings yet
- Best Practice & Research Clinical RheumatologyDocument14 pagesBest Practice & Research Clinical Rheumatologycukup unduhNo ratings yet
- CV Risc in SLE 5pdfDocument18 pagesCV Risc in SLE 5pdfŞtefaniuc IulianNo ratings yet
- Artículo 5 - COMORD. 2020Document10 pagesArtículo 5 - COMORD. 2020Nicolas CharrisNo ratings yet
- Obesity A Risk Factor For Increased COVID 19 Prevalence, Severity and Lethality (Review)Document11 pagesObesity A Risk Factor For Increased COVID 19 Prevalence, Severity and Lethality (Review)Imin BuntaraNo ratings yet
- 2 PBDocument9 pages2 PBDIAN HANDAYANINo ratings yet
- SLE DR - Nita Uul PunyaDocument18 pagesSLE DR - Nita Uul PunyaduratulkhNo ratings yet
- The Open Dermatology JournalDocument7 pagesThe Open Dermatology JournalTri SulistiyawatiNo ratings yet
- Smoking and PsoriasisDocument23 pagesSmoking and PsoriasishadiNo ratings yet
- Evaluation A ND Managementof Psoria Sis: An I Nternist 'S GuideDocument13 pagesEvaluation A ND Managementof Psoria Sis: An I Nternist 'S GuideCarlos PérezNo ratings yet
- Keac403 (1) 2Document14 pagesKeac403 (1) 2GysviuuNo ratings yet
- Periodontal Status of Survivors of Acute MyocardialDocument11 pagesPeriodontal Status of Survivors of Acute MyocardialJAVIERA IGNACIA PEÑAILILLO MONÁRDEZNo ratings yet
- Review Article: Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Cardiovascular LinksDocument19 pagesReview Article: Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Cardiovascular LinksMuhammad Jahari SupiantoNo ratings yet
- 48 Cardiovascular Involvement inDocument5 pages48 Cardiovascular Involvement inchandanNo ratings yet
- During The Coronavirus Disease 2019 (COVID-19) Pandemic, A New Phenomenon Manifesting As ADocument5 pagesDuring The Coronavirus Disease 2019 (COVID-19) Pandemic, A New Phenomenon Manifesting As APratiwiNo ratings yet
- Cardiovascular Disease in Type 2 Diabetes Mellitus: Progress Toward Personalized ManagementDocument15 pagesCardiovascular Disease in Type 2 Diabetes Mellitus: Progress Toward Personalized Managementngọc ngôNo ratings yet
- The Effect of Age On The Development and Outcome of Adult SepsisDocument7 pagesThe Effect of Age On The Development and Outcome of Adult Sepsisjsph3No ratings yet
- Choudhury 2014Document30 pagesChoudhury 2014Andry Wahyudi AgusNo ratings yet
- Fast Facts: Myelodysplastic Syndromes: Determining risk, tailoring therapy, supporting patientsFrom EverandFast Facts: Myelodysplastic Syndromes: Determining risk, tailoring therapy, supporting patientsNo ratings yet
- Heart Valve Disease: State of the ArtFrom EverandHeart Valve Disease: State of the ArtJose ZamoranoNo ratings yet
- Game Changer in Dealing With Hard Scale Using A Slickline Torque Action Debris BreakerDocument1 pageGame Changer in Dealing With Hard Scale Using A Slickline Torque Action Debris Breakermahmoud korieshNo ratings yet
- Gas Lift in Heavy Oil ManuscriptDocument9 pagesGas Lift in Heavy Oil Manuscriptmahmoud korieshNo ratings yet
- Prime 1 - 4Document7 pagesPrime 1 - 4mahmoud korieshNo ratings yet
- The Clinical Spectrum of Psoriasis: Luigi Naldi, MD, Daniele Gambini, MDDocument9 pagesThe Clinical Spectrum of Psoriasis: Luigi Naldi, MD, Daniele Gambini, MDmahmoud korieshNo ratings yet
- SPE-177990-MS Electric Submersible Pump Installation and Commissioning - Challenges and Lesson Learned From Field DevelopmentDocument17 pagesSPE-177990-MS Electric Submersible Pump Installation and Commissioning - Challenges and Lesson Learned From Field Developmentmahmoud korieshNo ratings yet
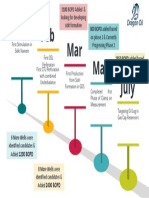
- Jan July May Mar Feb: Looking For Developing Sidri Formation On Phase 1 & Currently Progressing Phase 2Document1 pageJan July May Mar Feb: Looking For Developing Sidri Formation On Phase 1 & Currently Progressing Phase 2mahmoud korieshNo ratings yet
- Aoran: - A - Book - An - Ant - An - ElephantDocument1 pageAoran: - A - Book - An - Ant - An - Elephantmahmoud korieshNo ratings yet
- Choose The Correct AnswerDocument1 pageChoose The Correct Answermahmoud korieshNo ratings yet
- Should or Shouldnt Direct Method Activities - 115041Document5 pagesShould or Shouldnt Direct Method Activities - 115041mahmoud korieshNo ratings yet
- Name - No - ClassDocument1 pageName - No - Classmahmoud korieshNo ratings yet
- 2sea Animals Game Games - 8420Document14 pages2sea Animals Game Games - 8420mahmoud korieshNo ratings yet
- 3wild Animals Game Games - 8419Document15 pages3wild Animals Game Games - 8419mahmoud korieshNo ratings yet
- On ..My Birthday at .8 Am. in . The Morning. at .Night. in Winter. On MondayDocument3 pagesOn ..My Birthday at .8 Am. in . The Morning. at .Night. in Winter. On Mondaymahmoud korieshNo ratings yet
- Julian2014 PDFDocument9 pagesJulian2014 PDFmahmoud korieshNo ratings yet
- 117 Torque Action Debris Breaker Pws DsheetDocument1 page117 Torque Action Debris Breaker Pws Dsheetmahmoud korieshNo ratings yet
- Schmid 1973Document14 pagesSchmid 1973mahmoud korieshNo ratings yet
- OilfieldTechnology November 2015 PDFDocument76 pagesOilfieldTechnology November 2015 PDFmahmoud korieshNo ratings yet
- Fournier 2000Document15 pagesFournier 2000mahmoud korieshNo ratings yet
- Fournier 2000Document15 pagesFournier 2000mahmoud korieshNo ratings yet
- Breaking StrengthDocument1 pageBreaking Strengthmahmoud korieshNo ratings yet
- Top Squeeze or Top Fill: Improved Secondary Cementing For Geothermal WellsDocument4 pagesTop Squeeze or Top Fill: Improved Secondary Cementing For Geothermal Wellsmahmoud korieshNo ratings yet
- Update On Arthritis in Kids and Adults: Jia, Ra and OaDocument68 pagesUpdate On Arthritis in Kids and Adults: Jia, Ra and OaDian Hayuningtyas PNo ratings yet
- Bases Moleculares Enfermedades NeurodegenerativasDocument53 pagesBases Moleculares Enfermedades NeurodegenerativasLaura Paola Corredor NietoNo ratings yet
- Effect of Night Class On Academic PerforDocument19 pagesEffect of Night Class On Academic PerforWilliam DizonNo ratings yet
- Ozone Therapy A New Exemplar in DentistryDocument5 pagesOzone Therapy A New Exemplar in DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Type 3 Cytokines IL-17A and IL-22 Drive TGF - Dependent Liver FibrosisDocument16 pagesType 3 Cytokines IL-17A and IL-22 Drive TGF - Dependent Liver FibrosisAndrio PalayukanNo ratings yet
- DITIADocument5 pagesDITIADian PertiwiNo ratings yet
- Arch Facial Plast SurgDocument5 pagesArch Facial Plast SurgEliann GabaldónNo ratings yet
- Nutrition and Exercise ImmunologyDocument204 pagesNutrition and Exercise ImmunologytodayisnovemberNo ratings yet
- Drug StudyDocument4 pagesDrug Studyjazmine_caritos100% (2)
- Jurnal Stress OksidatifDocument8 pagesJurnal Stress OksidatifDesi RatnaningtyasNo ratings yet
- Immunomodulatory Effects of Polysaccharides From Edible Fungus - A ReviewDocument8 pagesImmunomodulatory Effects of Polysaccharides From Edible Fungus - A ReviewAlonso Ornelas GonzalezNo ratings yet
- Pathogenic Fungal Infection in The Lung: Zhi Li, Gen Lu and Guangxun MengDocument20 pagesPathogenic Fungal Infection in The Lung: Zhi Li, Gen Lu and Guangxun Mengbanteng wibisonoNo ratings yet
- Thoracoscopy MinimalDocument32 pagesThoracoscopy MinimalThomas KurianNo ratings yet
- PhytophotodermatitisDocument3 pagesPhytophotodermatitisjaggu5005No ratings yet
- Hypoalbuminemia: Pathogenesis and Clinical SignificanceDocument13 pagesHypoalbuminemia: Pathogenesis and Clinical SignificanceLuna Ivanka Al FatihNo ratings yet
- 2019 2 6 - enDocument4 pages2019 2 6 - enmisulica2010No ratings yet
- Endothelial ACKR3 Drives Atherosclerosis by PromotDocument18 pagesEndothelial ACKR3 Drives Atherosclerosis by PromotspraptamaNo ratings yet
- Immunology Made Simple AF FinalDocument77 pagesImmunology Made Simple AF FinalStudy EverydayNo ratings yet
- Enzyme Promiscuity in Earthworm Serine Protease: Substrate Versatility and Therapeutic PotentialDocument8 pagesEnzyme Promiscuity in Earthworm Serine Protease: Substrate Versatility and Therapeutic PotentialKhánh HuyềnNo ratings yet
- Histology of PulpDocument61 pagesHistology of PulpLom SimloteNo ratings yet
- BC Lioton SKDocument71 pagesBC Lioton SKAlejandra Cale Radowitz0% (1)
- Phenylbutazone Review-Dr. Lawrence R. SomaDocument12 pagesPhenylbutazone Review-Dr. Lawrence R. SomaAndi Ade NurqalbiNo ratings yet
- Events - in - Acute - Inflammation FlowchartDocument1 pageEvents - in - Acute - Inflammation FlowchartHarini KarthikeyanNo ratings yet
- 2021 Feb Black Seed Oil Infographic (Final Approved)Document1 page2021 Feb Black Seed Oil Infographic (Final Approved)Prastica Diah PratiwiNo ratings yet
- Binding Immunoglobulin During DiseaseDocument12 pagesBinding Immunoglobulin During DiseaseAGLNo ratings yet
- Oxygen Ontents - Reading - ExcerptDocument23 pagesOxygen Ontents - Reading - ExcerptBabli Lovely Nicky100% (1)
- Diet and Liver Disease PDFDocument42 pagesDiet and Liver Disease PDFRaghad.SNo ratings yet
- Yi Jin JingDocument17 pagesYi Jin Jingflorinhangan67% (3)











































































































Download as pdf or txt
You might also like
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocument4 pagesPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Acute and Chronic Inflammation MCQDocument2 pagesAcute and Chronic Inflammation MCQBeda Malecdan73% (30)
- Psoriasis and Comorbid DeseaseDocument67 pagesPsoriasis and Comorbid DeseaseAl NaifNo ratings yet
- SolDocument10 pagesSolTsigereda AberaNo ratings yet
- Psoriasis and Risk of Cardiovascular Disease: Case Report and DiscussionDocument4 pagesPsoriasis and Risk of Cardiovascular Disease: Case Report and DiscussionAbhishek KushwahNo ratings yet
- Update ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentDocument35 pagesUpdate ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentSudeesh KumarNo ratings yet
- Ahri Proposal 2Document28 pagesAhri Proposal 2Tsigereda AberaNo ratings yet
- Jcad 12 6 46 PDFDocument9 pagesJcad 12 6 46 PDFRatu TriaNo ratings yet
- Psoriasis and Dermatitis AtopicDocument11 pagesPsoriasis and Dermatitis AtopicsayasajaNo ratings yet
- Psoriasis NATURE AYFinlayDocument48 pagesPsoriasis NATURE AYFinlayMelly SyafridaNo ratings yet
- Psoriasis Carries An Increased Risk of Venous Thromboembolism: A Danish Nationwide Cohort StudyDocument6 pagesPsoriasis Carries An Increased Risk of Venous Thromboembolism: A Danish Nationwide Cohort StudyAnonymous 1bEPjKNo ratings yet
- Psoriasis and Vascular Disease: An Unsolved Mystery: ReviewDocument6 pagesPsoriasis and Vascular Disease: An Unsolved Mystery: ReviewkendinceNo ratings yet
- The Effect of Inflammation and Infection On Lipids and LipoproteinsDocument46 pagesThe Effect of Inflammation and Infection On Lipids and Lipoproteinshani akbarNo ratings yet
- Wijsenbeek2015 Treatment of SarcoidosisDocument17 pagesWijsenbeek2015 Treatment of SarcoidosisJohan ArocaNo ratings yet
- TB and PADDocument7 pagesTB and PADdicky wahyudiNo ratings yet
- Tuberculosis and Diabetes Mellitus - An Underappreciated AssociationDocument9 pagesTuberculosis and Diabetes Mellitus - An Underappreciated AssociationNajla rayNo ratings yet
- LEATRACHRER REVIEW TsiDocument22 pagesLEATRACHRER REVIEW TsiTsigereda AberaNo ratings yet
- Clinical Manifestations and Diagnosis of Raynaud Phenomenon - UpToDateDocument29 pagesClinical Manifestations and Diagnosis of Raynaud Phenomenon - UpToDateMarcos Torchia EstebanNo ratings yet
- Chronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With SepsisDocument8 pagesChronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With Sepsisida ayu agung WijayantiNo ratings yet
- Psoriasis and ComorbiditiesDocument8 pagesPsoriasis and ComorbiditiesIvanWinardyNo ratings yet
- EMTC Ortegahernandez2012 PDFDocument12 pagesEMTC Ortegahernandez2012 PDFGabriel CuadrosNo ratings yet
- Gelfand 2012Document5 pagesGelfand 2012gyyygNo ratings yet
- Bur FieldDocument6 pagesBur FieldNexi anessaNo ratings yet
- Yang LengkapDocument9 pagesYang LengkapauliyasaumaNo ratings yet
- Coronavirus Disease 2019 and Cardiovascular SystemDocument19 pagesCoronavirus Disease 2019 and Cardiovascular SystemAlif riadiNo ratings yet
- Stroke As A Potential Complication of COVID-19-Associated Coagulopathy: A Narrative and Systematic Review of The LiteratureDocument11 pagesStroke As A Potential Complication of COVID-19-Associated Coagulopathy: A Narrative and Systematic Review of The LiteraturedenisNo ratings yet
- Epidemiology of Peripheral Artery Disease: Narrative ReviewDocument15 pagesEpidemiology of Peripheral Artery Disease: Narrative ReviewRumah Sakit J. H. Awaloei ManadoNo ratings yet
- COVID 19: Is There A Link Between The Course of Infection and Pharmacological Agents in Diabetes?Document8 pagesCOVID 19: Is There A Link Between The Course of Infection and Pharmacological Agents in Diabetes?Marcela MahechaNo ratings yet
- Brauchli Et Al-2008-British Journal of Dermatology Psoriasis and The Risk of Incident Diabetes MellitusDocument7 pagesBrauchli Et Al-2008-British Journal of Dermatology Psoriasis and The Risk of Incident Diabetes Mellitussaputri rizkaNo ratings yet
- 38 Reaserch South AfricaDocument6 pages38 Reaserch South AfricaTsigereda AberaNo ratings yet
- All-Cause and Cause-Specific Mortality in Psoriasis: A Systematic Review and Meta-AnalysisDocument12 pagesAll-Cause and Cause-Specific Mortality in Psoriasis: A Systematic Review and Meta-AnalysisRielz ThereaperzNo ratings yet
- Manuscript Category: Review: Version of Record Doi: 10.1111/JDI.13326Document30 pagesManuscript Category: Review: Version of Record Doi: 10.1111/JDI.13326Marcela MahechaNo ratings yet
- The Bidirectional Relationship Between TuberculosiDocument7 pagesThe Bidirectional Relationship Between TuberculosiJunita Nelly Esther JosephNo ratings yet
- Zozulinska, 2006Document5 pagesZozulinska, 2006wanda oktariaNo ratings yet
- NIH Public Access: Metabolic Syndrome in Patients With Psoriatic DiseaseDocument8 pagesNIH Public Access: Metabolic Syndrome in Patients With Psoriatic DiseaseFEISAL HILMAN -No ratings yet
- JCM 10 01798Document20 pagesJCM 10 01798Asad NawazNo ratings yet
- Methotrexate Reduces The Occurrence of Cerebrovascular Events Among Taiwanese Psoriatic Patients: A Nationwide Population-Based StudyDocument4 pagesMethotrexate Reduces The Occurrence of Cerebrovascular Events Among Taiwanese Psoriatic Patients: A Nationwide Population-Based StudyHermayudiNo ratings yet
- Chronic Obstructive Pulmonary Disease and Diabetes MellitusDocument19 pagesChronic Obstructive Pulmonary Disease and Diabetes MellitusMirza RisqaNo ratings yet
- Type Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Document2 pagesType Diabetes and Multiple Myeloma The Latest Insights 2329 6917.1000e110Akreditasi InternaNo ratings yet
- A Review of COVID 19 Vaccines and Major Considerations For Diabetic Patients. Biotechnology and Applied BiochemistryDocument22 pagesA Review of COVID 19 Vaccines and Major Considerations For Diabetic Patients. Biotechnology and Applied Biochemistryimamsantos1191No ratings yet
- Diabetes and Sepsis Outcomes - It Is Not All Bad News: CommentaryDocument2 pagesDiabetes and Sepsis Outcomes - It Is Not All Bad News: CommentaryYoery SadewoNo ratings yet
- Cardiovascular Disease and Its Relationship With Chronic Kidney DiseaseDocument9 pagesCardiovascular Disease and Its Relationship With Chronic Kidney Diseasetrinda ireneNo ratings yet
- Psoriasis With Vascular DiseaseDocument4 pagesPsoriasis With Vascular Diseasemegh dutNo ratings yet
- Best Practice & Research Clinical RheumatologyDocument14 pagesBest Practice & Research Clinical Rheumatologycukup unduhNo ratings yet
- CV Risc in SLE 5pdfDocument18 pagesCV Risc in SLE 5pdfŞtefaniuc IulianNo ratings yet
- Artículo 5 - COMORD. 2020Document10 pagesArtículo 5 - COMORD. 2020Nicolas CharrisNo ratings yet
- Obesity A Risk Factor For Increased COVID 19 Prevalence, Severity and Lethality (Review)Document11 pagesObesity A Risk Factor For Increased COVID 19 Prevalence, Severity and Lethality (Review)Imin BuntaraNo ratings yet
- 2 PBDocument9 pages2 PBDIAN HANDAYANINo ratings yet
- SLE DR - Nita Uul PunyaDocument18 pagesSLE DR - Nita Uul PunyaduratulkhNo ratings yet
- The Open Dermatology JournalDocument7 pagesThe Open Dermatology JournalTri SulistiyawatiNo ratings yet
- Smoking and PsoriasisDocument23 pagesSmoking and PsoriasishadiNo ratings yet
- Evaluation A ND Managementof Psoria Sis: An I Nternist 'S GuideDocument13 pagesEvaluation A ND Managementof Psoria Sis: An I Nternist 'S GuideCarlos PérezNo ratings yet
- Keac403 (1) 2Document14 pagesKeac403 (1) 2GysviuuNo ratings yet
- Periodontal Status of Survivors of Acute MyocardialDocument11 pagesPeriodontal Status of Survivors of Acute MyocardialJAVIERA IGNACIA PEÑAILILLO MONÁRDEZNo ratings yet
- Review Article: Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Cardiovascular LinksDocument19 pagesReview Article: Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Cardiovascular LinksMuhammad Jahari SupiantoNo ratings yet
- 48 Cardiovascular Involvement inDocument5 pages48 Cardiovascular Involvement inchandanNo ratings yet
- During The Coronavirus Disease 2019 (COVID-19) Pandemic, A New Phenomenon Manifesting As ADocument5 pagesDuring The Coronavirus Disease 2019 (COVID-19) Pandemic, A New Phenomenon Manifesting As APratiwiNo ratings yet
- Cardiovascular Disease in Type 2 Diabetes Mellitus: Progress Toward Personalized ManagementDocument15 pagesCardiovascular Disease in Type 2 Diabetes Mellitus: Progress Toward Personalized Managementngọc ngôNo ratings yet
- The Effect of Age On The Development and Outcome of Adult SepsisDocument7 pagesThe Effect of Age On The Development and Outcome of Adult Sepsisjsph3No ratings yet
- Choudhury 2014Document30 pagesChoudhury 2014Andry Wahyudi AgusNo ratings yet
- Fast Facts: Myelodysplastic Syndromes: Determining risk, tailoring therapy, supporting patientsFrom EverandFast Facts: Myelodysplastic Syndromes: Determining risk, tailoring therapy, supporting patientsNo ratings yet
- Heart Valve Disease: State of the ArtFrom EverandHeart Valve Disease: State of the ArtJose ZamoranoNo ratings yet
- Game Changer in Dealing With Hard Scale Using A Slickline Torque Action Debris BreakerDocument1 pageGame Changer in Dealing With Hard Scale Using A Slickline Torque Action Debris Breakermahmoud korieshNo ratings yet
- Gas Lift in Heavy Oil ManuscriptDocument9 pagesGas Lift in Heavy Oil Manuscriptmahmoud korieshNo ratings yet
- Prime 1 - 4Document7 pagesPrime 1 - 4mahmoud korieshNo ratings yet
- The Clinical Spectrum of Psoriasis: Luigi Naldi, MD, Daniele Gambini, MDDocument9 pagesThe Clinical Spectrum of Psoriasis: Luigi Naldi, MD, Daniele Gambini, MDmahmoud korieshNo ratings yet
- SPE-177990-MS Electric Submersible Pump Installation and Commissioning - Challenges and Lesson Learned From Field DevelopmentDocument17 pagesSPE-177990-MS Electric Submersible Pump Installation and Commissioning - Challenges and Lesson Learned From Field Developmentmahmoud korieshNo ratings yet
- Jan July May Mar Feb: Looking For Developing Sidri Formation On Phase 1 & Currently Progressing Phase 2Document1 pageJan July May Mar Feb: Looking For Developing Sidri Formation On Phase 1 & Currently Progressing Phase 2mahmoud korieshNo ratings yet
- Aoran: - A - Book - An - Ant - An - ElephantDocument1 pageAoran: - A - Book - An - Ant - An - Elephantmahmoud korieshNo ratings yet
- Choose The Correct AnswerDocument1 pageChoose The Correct Answermahmoud korieshNo ratings yet
- Should or Shouldnt Direct Method Activities - 115041Document5 pagesShould or Shouldnt Direct Method Activities - 115041mahmoud korieshNo ratings yet
- Name - No - ClassDocument1 pageName - No - Classmahmoud korieshNo ratings yet
- 2sea Animals Game Games - 8420Document14 pages2sea Animals Game Games - 8420mahmoud korieshNo ratings yet
- 3wild Animals Game Games - 8419Document15 pages3wild Animals Game Games - 8419mahmoud korieshNo ratings yet
- On ..My Birthday at .8 Am. in . The Morning. at .Night. in Winter. On MondayDocument3 pagesOn ..My Birthday at .8 Am. in . The Morning. at .Night. in Winter. On Mondaymahmoud korieshNo ratings yet
- Julian2014 PDFDocument9 pagesJulian2014 PDFmahmoud korieshNo ratings yet
- 117 Torque Action Debris Breaker Pws DsheetDocument1 page117 Torque Action Debris Breaker Pws Dsheetmahmoud korieshNo ratings yet
- Schmid 1973Document14 pagesSchmid 1973mahmoud korieshNo ratings yet
- OilfieldTechnology November 2015 PDFDocument76 pagesOilfieldTechnology November 2015 PDFmahmoud korieshNo ratings yet
- Fournier 2000Document15 pagesFournier 2000mahmoud korieshNo ratings yet
- Fournier 2000Document15 pagesFournier 2000mahmoud korieshNo ratings yet
- Breaking StrengthDocument1 pageBreaking Strengthmahmoud korieshNo ratings yet
- Top Squeeze or Top Fill: Improved Secondary Cementing For Geothermal WellsDocument4 pagesTop Squeeze or Top Fill: Improved Secondary Cementing For Geothermal Wellsmahmoud korieshNo ratings yet
- Update On Arthritis in Kids and Adults: Jia, Ra and OaDocument68 pagesUpdate On Arthritis in Kids and Adults: Jia, Ra and OaDian Hayuningtyas PNo ratings yet
- Bases Moleculares Enfermedades NeurodegenerativasDocument53 pagesBases Moleculares Enfermedades NeurodegenerativasLaura Paola Corredor NietoNo ratings yet
- Effect of Night Class On Academic PerforDocument19 pagesEffect of Night Class On Academic PerforWilliam DizonNo ratings yet
- Ozone Therapy A New Exemplar in DentistryDocument5 pagesOzone Therapy A New Exemplar in DentistryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Type 3 Cytokines IL-17A and IL-22 Drive TGF - Dependent Liver FibrosisDocument16 pagesType 3 Cytokines IL-17A and IL-22 Drive TGF - Dependent Liver FibrosisAndrio PalayukanNo ratings yet
- DITIADocument5 pagesDITIADian PertiwiNo ratings yet
- Arch Facial Plast SurgDocument5 pagesArch Facial Plast SurgEliann GabaldónNo ratings yet
- Nutrition and Exercise ImmunologyDocument204 pagesNutrition and Exercise ImmunologytodayisnovemberNo ratings yet
- Drug StudyDocument4 pagesDrug Studyjazmine_caritos100% (2)
- Jurnal Stress OksidatifDocument8 pagesJurnal Stress OksidatifDesi RatnaningtyasNo ratings yet
- Immunomodulatory Effects of Polysaccharides From Edible Fungus - A ReviewDocument8 pagesImmunomodulatory Effects of Polysaccharides From Edible Fungus - A ReviewAlonso Ornelas GonzalezNo ratings yet
- Pathogenic Fungal Infection in The Lung: Zhi Li, Gen Lu and Guangxun MengDocument20 pagesPathogenic Fungal Infection in The Lung: Zhi Li, Gen Lu and Guangxun Mengbanteng wibisonoNo ratings yet
- Thoracoscopy MinimalDocument32 pagesThoracoscopy MinimalThomas KurianNo ratings yet
- PhytophotodermatitisDocument3 pagesPhytophotodermatitisjaggu5005No ratings yet
- Hypoalbuminemia: Pathogenesis and Clinical SignificanceDocument13 pagesHypoalbuminemia: Pathogenesis and Clinical SignificanceLuna Ivanka Al FatihNo ratings yet
- 2019 2 6 - enDocument4 pages2019 2 6 - enmisulica2010No ratings yet
- Endothelial ACKR3 Drives Atherosclerosis by PromotDocument18 pagesEndothelial ACKR3 Drives Atherosclerosis by PromotspraptamaNo ratings yet
- Immunology Made Simple AF FinalDocument77 pagesImmunology Made Simple AF FinalStudy EverydayNo ratings yet
- Enzyme Promiscuity in Earthworm Serine Protease: Substrate Versatility and Therapeutic PotentialDocument8 pagesEnzyme Promiscuity in Earthworm Serine Protease: Substrate Versatility and Therapeutic PotentialKhánh HuyềnNo ratings yet
- Histology of PulpDocument61 pagesHistology of PulpLom SimloteNo ratings yet
- BC Lioton SKDocument71 pagesBC Lioton SKAlejandra Cale Radowitz0% (1)
- Phenylbutazone Review-Dr. Lawrence R. SomaDocument12 pagesPhenylbutazone Review-Dr. Lawrence R. SomaAndi Ade NurqalbiNo ratings yet
- Events - in - Acute - Inflammation FlowchartDocument1 pageEvents - in - Acute - Inflammation FlowchartHarini KarthikeyanNo ratings yet
- 2021 Feb Black Seed Oil Infographic (Final Approved)Document1 page2021 Feb Black Seed Oil Infographic (Final Approved)Prastica Diah PratiwiNo ratings yet
- Binding Immunoglobulin During DiseaseDocument12 pagesBinding Immunoglobulin During DiseaseAGLNo ratings yet
- Oxygen Ontents - Reading - ExcerptDocument23 pagesOxygen Ontents - Reading - ExcerptBabli Lovely Nicky100% (1)
- Diet and Liver Disease PDFDocument42 pagesDiet and Liver Disease PDFRaghad.SNo ratings yet
- Yi Jin JingDocument17 pagesYi Jin Jingflorinhangan67% (3)