Professional Documents
Culture Documents
Rheumatologic Disorders and The Nervous System.6
Rheumatologic Disorders and The Nervous System.6
Uploaded by
monicaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Rheumatologic Disorders and The Nervous System.6
Rheumatologic Disorders and The Nervous System.6
Uploaded by
monicaCopyright:
Available Formats
Rheumatologic Disorders REVIEW ARTICLE
and the Nervous System C O N T I N U UM A U D I O
I NT E R V I E W A V A I L AB L E
ONLINE
By Pantelis P. Pavlakis, MD, PhD
ABSTRACT
PURPOSE: This article describes the neurologic manifestations of systemic
Downloaded from https://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3/TxXCJJj86GD8D9iUqcRIkKrSwWxeGrq+wIl2R43wwI= on 07/16/2020
autoimmune diseases.
RECENT FINDINGS: Systemic autoimmune diseases can be associated with a wide
spectrum of neurologic comorbidities involving the central and peripheral
nervous systems. Systemic lupus erythematosus (SLE) can be associated with
a number of manifestations predominantly affecting the central nervous
system (CNS), whereas peripheral neuropathy is less common. Sjögren
syndrome can be associated with peripheral neuropathy in 10% of cases and
CNS disease in 2% to 5% of cases. The risk of stroke is increased in SLE,
rheumatoid arthritis, temporal arteritis, psoriatic arthritis, and ankylosing
spondylitis. Systemic vasculitides present most commonly with mononeuritis
multiplex but can also affect the CNS. Cognitive dysfunction is a common
symptom among patients with systemic autoimmune diseases, most
commonly seen in patients with SLE or Sjögren syndrome.
SUMMARY: Neurologic manifestations of systemic autoimmune disease are
important to recognize, as they may often be the presenting manifestation
CITE AS:
leading to diagnosis of the systemic disease or may be associated with increased
CONTINUUM (MINNEAP MINN)
morbidity, other complications, or mortality. Timely diagnosis and institution 2020;26(3, NEUROLOGY OF
of appropriate treatment, often requiring multidisciplinary care, is essential to SYSTEMIC DISEASE):591–610.
minimize morbidity and decrease the risk of permanent neurologic deficits.
Address correspondence to
Dr Pantelis Pavlakis, Hospital for
Special Surgery, 535 E 70th St,
N
INTRODUCTION New York, NY, 10021,
pavlakisp@hss.edu.
eurologic manifestations of systemic autoimmune diseases
encompass a wide spectrum of syndromes involving the central RELATIONSHIP DISCLOSURE:
nervous system (CNS) and peripheral nervous system (PNS). Dr Pavlakis has received
personal compensation for
Increased awareness is required as they may be the presenting completing an online
manifestation leading to the diagnosis of a systemic autoimmune survey from Alexion
Pharmaceuticals, Inc.
disease, or they may present in otherwise quiescent systemic disease. However, in
other cases, they may be associated with severe systemic disease and increased risk UNLABELED USE OF
of morbidity and mortality. Their presentation can overlap with other distinct PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
neurologic syndromes, which further complicates their diagnosis and classification Dr Pavlakis discusses the
(TABLE 3-1). Prompt recognition and initiation of treatment is required in many unlabeled/investigational use
cases to prevent permanent neurologic dysfunction or disease progression. of biologic therapies for the
neurologic manifestations of
rheumatologic disorders.
SYSTEMIC LUPUS ERYTHEMATOSUS
A wide spectrum of neurologic manifestations has been observed in patients with © 2020 American Academy
systemic lupus erythematosus (SLE) (TABLE 3-2).1 Some of these, such as of Neurology.
CONTINUUMJOURNAL.COM 591
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
TABLE 3-1 Common/Characteristic Patterns of Neurologic Involvement in
Rheumatologic Diseases
Systemic Lupus Sjögren Rheumatoid Systemic Psoriatic Ankylosing
Erythematosus Syndrome Arthritis Vasculitides Scleroderma Arthritis Spondylitis
Aseptic X X Granulomatosis
meningitis with polyangiitis
Increased risk X X Takayasu X X
of stroke arteritis,
temporal
arteritis,
polyarteritis
nodosa
Seizures X X Can be X
presenting
symptom
of central
nervous system
vasculitis
Cerebral Behçet disease
venous sinus
thrombosis
Central X X Behçet
nervous disease, rarely
system
demyelination
(including
overlapping
neuromyelitis
optica [NMO]
spectrum
disorder)
Peripheral Axonal Small fiber Entrapment Mononeuritis X
neuropathy polyneuropathy, neuropathy, axonal neuropathies, multiplex, axonal
small fiber polyneuropathy, axonal polyneuropathy
neuropathy, mononeuritis polyneuropathy,
mononeuritis multiplex, sensory demyelinating
multiplex, ataxic neuropathy, neuropathy
demyelinating demyelinating
neuropathy neuropathy
Increased X (cervical X
risk of spinal spine)
stenosis
Myopathy X (most X
commonly
inclusion body
myositis)
592 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
headache and mood disorders, may be nonspecific; others, such as stroke, may be
due to an overlapping syndrome (eg, antiphospholipid antibody syndrome) and
may not necessarily be attributable to SLE. As a result, the reported frequency of
neuropsychiatric manifestations has ranged widely. More recent cohorts using
stricter criteria and causal attribution algorithms have estimated the frequency of
neuropsychiatric events to be 13% to 21% in patients with SLE.2 The vast majority
involve the CNS, while PNS involvement can be seen in 8% of patients.2 Early
identification and treatment of neurologic manifestations in patients with SLE is very
important, as patients with SLE and renal or neurologic involvement are considered to
have severe disease, resulting in higher rates of morbidity and mortality.3
The exact mechanisms leading to neurologic manifestations in SLE are unclear.
Microvasculopathy, local inflammatory mediators, and autoantibodies, acting both
directly and indirectly by causing blood-brain barrier dysfunction, have been
implicated.4 Although prior studies have reported an association with specific
autoantibodies, including NR2 glutamate receptor antibodies and ribosomal P
protein antibodies, these results have not been validated in larger cohorts, and their
diagnostic value in clinical practice remains limited.2,4 Antiphospholipid antibodies,
which have been associated with strokes and seizures, are a notable exception.4
Headache5 and mood disorders, including depression,6 have been the most
frequently reported manifestations; however, more recent studies suggest that
the overall frequency of headache is not significantly higher in patients with SLE,
and neither headache nor mood disorders are associated with disease activity,
Neuropsychiatric Syndromes Encountered in Patients With Systemic Lupus TABLE 3-2
Erythematosusa
Central Nervous System Manifestations
◆ Headache
◆ Mood disorders
◆ Psychosis
◆ Stroke
◆ Seizures
◆ Posterior reversible encephalopathy syndrome (PRES)
◆ Myelitis
◆ Optic neuritis
◆ Overlapping multiple sclerosis/neuromyelitis optica (NMO) spectrum disorder
◆ Cognitive dysfunction
Peripheral Neuropathies
◆ Axonal polyneuropathy
◆ Small fiber neuropathy
◆ Mononeuritis multiplex
◆ Demyelinating neuropathy
a
Modified with permission from ACR Ad Hoc Committee on Neuropsychiatric Lupus Nomenclature, Arthritis
Rheumatol.1 © 1999 American College of Rheumatology.
CONTINUUMJOURNAL.COM 593
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
CASE 3-1 A previously healthy 45-year-old woman presented to the emergency
department with 2 days of progressive bilateral leg weakness and
numbness. She reported low-grade fever, malaise, and arthralgia 1 week
earlier and urinary retention 1 day before the onset of her leg symptoms.
Her general examination was notable for malar rash and swollen joints,
which were tender to palpation.
On neurologic examination, her mental status and cranial nerves were
intact. Muscle tone was increased in both legs. Strength was normal in
the arms. In her legs, strength was 3/5 in bilateral hip flexion, knee
flexion, and ankle dorsiflexion. Sensation to touch and pinprick was
decreased below the level of the umbilicus, and vibration sense was
absent in both legs up to the anterior superior iliac spines. Deep tendon
reflexes were normal in the arms and hyperactive (3+) in both knees and
ankles. Babinski sign was present bilaterally. She had a spastic gait and
required two canes to walk.
Blood work was notable for anemia, lymphopenia, and
thrombocytopenia. C3 and C4 complement levels were decreased.
Antinuclear and anti–double-stranded DNA antibodies were positive.
MRI of the thoracic spine showed a T2-hyperintense lesion at T10, which
enhanced after gadolinium administration. Aquaporin-4 antibodies were
negative.
She was immediately treated with IV methylprednisolone 1000 mg, and
after three daily doses, her leg strength and sensation improved partially,
but she was still not able to walk unassisted. Rheumatology was
consulted, and she was diagnosed with systemic lupus erythematosus
(SLE). Treatment with cyclophosphamide was initiated, and 6 months
later she was able to walk unassisted.
COMMENT The history and examination findings in this case localized to the spinal
cord, and MRI confirmed the presence of a myelopathy; her systemic
manifestations (malar rash, arthritis) and laboratory studies (anemia,
lymphopenia, thrombocytopenia, hypocomplementemia, positive
antinuclear and anti–double-stranded DNA antibodies) were suggestive
of SLE.
It is common for neurologic syndromes to be the presenting
manifestation of systemic autoimmune diseases. The differential diagnosis
includes vasculitis (which can also affect the spinal cord but would also be
expected to involve other areas of the central nervous system, such as the
brain, or the peripheral nervous system), multiple sclerosis, or
neuromyelitis optica spectrum disorder (NMOSD). NMOSD can coexist with
SLE or Sjögren syndrome, and aquaporin-4 antibody testing is important in
cases such as this as a positive result would confirm NMOSD as the cause
rather than a neurologic manifestation of the systemic autoimmune
disease. Another important point illustrated in this case is that prompt
initiation of treatment is required to mitigate or prevent permanent
neurologic dysfunction.
594 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
making it difficult to establish a causal relationship with the underlying KEY POINTS
systemic disease.5–7
● Patients with systemic
Psychosis can present in 1.5% of patients with SLE,7 although its frequency has lupus erythematosus,
varied among published studies. The majority of cases are attributable to the rheumatoid arthritis,
underlying disease, occur early in its course, and consist of a single psychotic temporal arteritis, psoriatic
event.2 Male sex, earlier age at time of SLE diagnosis, and history of other arthritis, and ankylosing
spondylitis have increased
neuropsychiatric events have been found to be associated with psychosis.2 This
risk of stroke.
should be differentiated from steroid-induced psychiatric disorders, which may
present as psychosis or mania. Onset after initiation of steroids and lack of other ● Patients with systemic
neuropsychiatric events can be more suggestive of the adverse effects of steroids lupus erythematosus have
rather than primary SLE-related psychosis. increased risk of developing
posterior reversible
Stroke has been reported to occur in 5% to 18% of patients with SLE,8 whereas encephalopathy syndrome.
more recent studies using attribution algorithms estimate stroke frequency at
5.6%.8 SLE has been found to be an independent risk factor for stroke (as have
several of the other conditions in this article), particularly in individuals younger
than age 40 or early in the course of the systemic disease. Ischemic strokes and
transient ischemic attacks comprise 80% of these events.8 Apart from the
traditional vascular risk factors, the presence of antiphospholipid antibodies,
high disease activity scores, a history of prior neuropsychiatric events,8 and being
of African descent9 have also been associated with increased risk of stroke.
Focal and generalized seizures have been reported in patients with SLE, and
prospective studies using attribution algorithms have estimated their frequency
at 4.6%.10 They usually occur early in the course of the disease10 and are
associated with higher disease activity, a history of psychosis, and
antiphospholipid or Sm antibodies.4
Posterior reversible encephalopathy syndrome (PRES) has also been
associated with SLE.11 Whether this represents a manifestation of the systemic
disease or the presence of SLE is simply a risk factor for developing PRES is
unclear. PRES is uncommon, seen in 0.69% to 1.8% of patients with SLE.11,12
Recurrent episodes can be seen in 20% of patients with PRES.12 Other risk factors
for PRES present in patients with SLE may include endothelial dysfunction,
which is thought to occur in these patients, or the immunosuppressive
medications that are often used to treat the systemic disease.11 A high index of
suspicion is required, as PRES can mimic other SLE-related neuropsychiatric
syndromes and is associated with greater morbidity and complications, including
intracerebral hemorrhage, more permanent neurologic deficits, and higher
mortality rates.12 Younger females seem to be more frequently affected;
hypertension, renal dysfunction, dyslipidemia, and active SLE have been
associated with PRES in patients with SLE.11 Treatment is mostly supportive,
consisting of blood pressure control and antiepileptic medications when seizures
are present12; high-dose corticosteroids have been used,12 but no randomized
clinical trials have assessed their efficacy.
The frequency of myelitis in SLE has been estimated at 1.2% in larger case
series (CASE 3-1).13 Although uncommon, it is important to diagnose and treat
myelitis promptly as it can cause significant neurologic deficits, with subsequent
effects in morbidity and quality of life. It may be the presenting manifestation or
present later in the course of the disease, and it may accompany active SLE or
disease in remission.13,14 Cases presenting with predominant signs of gray matter
dysfunction (eg, flaccid paresis) have been associated with higher disease
activity,14 double-stranded DNA, and antiphospholipid antibodies, whereas
CONTINUUMJOURNAL.COM 595
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
cases with predominant white matter dysfunction have been associated with
anti–aquaporin-4 (AQP4) seropositivity.14 Antibodies against AQP4 have been
identified in patients with SLE and myelitis; however, these are highly specific
for neuromyelitis optica spectrum disorders (NMOSDs) and are not present in
patients with systemic autoimmunity in the absence of neurologic involvement.15
Therefore, their presence is more suggestive of overlapping NMOSD rather than
a manifestation of the underlying systemic autoimmune disease.
Optic neuropathy is another uncommon manifestation of SLE, either in the
form of demyelinating optic neuritis or anterior ischemic optic neuropathy.16
Testing for antibodies against AQP4 in patients with optic neuritis is important,
as this can present in the absence of myelitis and earlier institution of treatment
could mitigate further neurologic burden in patients with NMOSD.
Peripheral neuropathies have been described in cohorts of patients with SLE in
variable frequencies; based on the results of larger-scale studies, the frequency of
peripheral neuropathy attributable to SLE has been estimated at 3.9%.17 Sensory
and sensorimotor axonal polyneuropathy are most frequently encountered, followed
by small fiber neuropathy.17 These may present with a length-dependent or
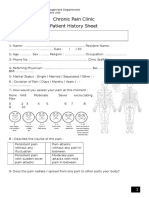
non–length-dependent distribution of symptoms (FIGURE 3-1).17 Mononeuropathy,
mononeuritis multiplex, and, less commonly, acute inflammatory demyelinating
polyradiculoneuropathy (AIDP), chronic inflammatory demyelinating
polyradiculoneuropathy (CIDP), or plexopathy have also been reported.17
The evidence regarding treatment of the neurologic manifestations of SLE is
limited, and its pathogenetic and phenotypic heterogeneity prevent the
development of uniform treatment guidelines. A general approach is that
thrombotic processes are treated with antiplatelet agents or anticoagulation, while
inflammatory processes are treated with corticosteroids and immunosuppression.18
FIGURE 3-1
Non–length-dependent and length-dependent patterns of peripheral neuropathy
distribution, as seen in rheumatologic diseases such as systemic lupus erythematosus (SLE)
and Sjögren syndrome.
Reprinted with permission from Oomatia A, et al, Arthritis Rheumatol.17 © 2014 American College
of Rheumatology.
596 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Severe inflammatory neurologic syndromes, including myelitis, are treated KEY POINTS
with high-dose IV methylprednisolone and additional immunosuppression.
● Neuromyelitis optica
Among various immunosuppressants tried, IV cyclophosphamide has the most spectrum disorders can
evidence supporting its use19; however, its efficacy should be weighed against its overlap with systemic lupus
significant toxicity, including nephrotoxicity, sterility, and malignancies. erythematosus or Sjögren
Various other immunosuppressants have been tried with mixed results. syndrome.
Rituximab has been used with success in cases refractory to cyclophosphamide.20
● Small fiber neuropathy is
It is noteworthy that the majority of literature available on treatment of myelitis the most common
associated with SLE was published before NMOSD was recognized as a distinct peripheral neuropathy in
disorder; therefore, in cases of myelitis, it is very important to identify cases of Sjögren syndrome. It may
overlapping NMOSD, as these should be treated as a coexisting primary present with length-
dependent or non–length-
neurologic disorder.21 dependent distribution
of symptoms and tends
SJÖGREN SYNDROME to be associated with
The PNS is more frequently affected than the CNS in Sjögren syndrome. fewer extraglandular
manifestations than large
Estimated frequencies of both vary significantly among published studies fiber neuropathy.
because of different diagnostic criteria of Sjögren syndrome applied and
differences in the definition of neurologic involvement. Among studies with ● Patients with Sjögren
larger numbers of patients, PNS involvement was seen in 10% of patients,22 while syndrome and small fiber
neuropathy are less
CNS involvement was seen in 2% to 5%.23,24 Neurologic manifestations may be the
frequently seropositive for
initial feature or may present later in the course of the disease22,25,26; they may be anti-Ro and anti-La
associated with mild glandular manifestations or part of active disease with other antibodies. Therefore, their
extraglandular manifestations.22,25,26 Making a diagnosis of Sjögren syndrome in absence should not
preclude the diagnosis of
patients presenting with neurologic syndromes and sicca symptoms (dry eyes and
Sjögren syndrome in an
dry mouth due to lymphocyte infiltration of exocrine glands, which are the otherwise appropriate
hallmark histopathologic findings of Sjögren syndrome) is important, as Sjögren clinical setting.
syndrome can be associated with increased risk of developing lymphoma.27
Sensory neuropathies seem to be the predominant type, and isolated small ● Sensory ataxic
neuropathy (neuronopathy)
fiber neuropathy seems to be the most common neuropathy in Sjögren syndrome can be seen in patients with
(TABLE 3-3).22,23 However, different types of neuropathy may coexist in the same Sjögren syndrome due to
patient. Sensory symptoms may present in a length-dependent or non–length- lymphocyte infiltration of
dependent distribution; a variable degree of autonomic symptoms may be dorsal root ganglia. The
differential diagnosis
present if autonomic fibers are involved. By definition, patients with small fiber includes paraneoplastic
neuropathies have no symptoms or signs of large fiber dysfunction and normal syndromes (usually in cases
nerve conduction studies. Sensory and sensorimotor large fiber axonal of small cell lung carcinoma)
polyneuropathies typically present with length-dependent sensory or motor human immunodeficiency
virus infection, platinum-
symptoms and deficits, and nerve conduction studies show a pattern of
based chemotherapy, or
axonal dysfunction. vitamin B6 toxicity.
Although individual presentations may vary, small fiber neuropathy tends to
present earlier in the course of the disease22 and is less frequently associated
with other extraglandular manifestations (eg, arthritis, Raynaud phenomenon,
pulmonary involvement, interstitial nephritis, glomerulonephritis, purpura)
than large fiber sensory axonal neuropathy,22 and patients are less frequently
seropositive for anti-Ro and anti-La antibodies.28 Therefore, negative serology
does not preclude the diagnosis of Sjögren syndrome in a patient with sicca
symptoms and neurologic involvement.
Sensory ataxic neuropathy is a rare but relentlessly progressive and disabling
form of sensory neuronopathy. Patients may present with variable sensory
symptoms, gait instability, loss of proprioception, and sensory ataxia.22
Pseudoathetoid hand movements may be seen due to loss of proprioception,
CONTINUUMJOURNAL.COM 597
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
which can lead to an initial diagnosis of a movement disorder. The onset may be
subacute or more insidious, and symptoms and signs follow a non–length-
dependent distribution. Strength is normal, and reflexes are absent. Nerve
conduction studies show a non–length-dependent loss of sensory amplitudes or
absent sensory responses with normal motor responses. Pathologic studies have
shown lymphocyte infiltration of the dorsal root ganglia in patients who are
affected,29 while imaging studies have shown T2 hyperintensities on MRI of
the dorsal root ganglia.30 However, the use of these diagnostic modalities in
clinical practice is limited.
Mononeuropathy and mononeuritis multiplex are uncommon but can be
present in Sjögren syndrome, usually in the setting of active systemic disease,
and have been associated with vasculitic involvement of other organs, such as
glomerulonephritis or purpura.31 The clinical presentation is similar to other
vasculitic neuropathies (refer to the section on systemic vasculitides). Serologic
markers of active systemic disease, such as low C4 complement levels,
hypergammaglobulinemia, or even cryoglobulinemia, are usually present.31
Although the diagnosis can often be made on clinical grounds, nerve biopsy
can confirm the diagnosis, showing findings of vasculitis.32 In these cases,
combined nerve and muscle biopsy is recommended to achieve maximal
diagnostic yield.32 Due its rapid onset, prompt diagnosis and treatment of
this neuropathy is required to prevent further neurologic deterioration or
irreversible neurologic deficits.
TABLE 3-3 Overview of Sensory Neuropathies Associated With Sjögren Syndrome
Sensory Ataxic Neuropathy
Sensory Axonal Neuropathy Small Fiber Neuropathy (Ganglionopathy)
Onset Later Earlier/may precede Varies
systemic disease
Other More frequently present Less frequently present Less frequently present
extraglandular
manifestations
Distribution Length dependent Length dependent/ Non–length dependent
non–length dependent
Sensory nerve Axonal dysfunction Normal Axonal dysfunction with
conduction studies multifocal distribution
Serology More frequently positive Less frequently positive Varies
(antinuclear
antibody, anti-Ro,
anti-La)
Differential Diabetes mellitus, vitamin B12 Diabetes mellitus, vitamin Small cell lung carcinoma
diagnosis deficiency, alcohol use disorder, B12 deficiency, alcohol use (often anti-Hu positive), HIV,
neurotoxic medications, disorder, neurotoxic platinum-based chemotherapy
paraproteinemia, HIV, hepatitis medications, HIV, infection, agents, vitamin B6 toxicity
C virus infection, other autoimmune other autoimmune diseases,
diseases, hereditary neuropathies hereditary neuropathies
HIV = human immunodeficiency virus.
598 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
A demyelinating neuropathy similar to CIDP has been reported to occur rarely
in association with Sjögren syndrome.33 Patients present with subacute or
insidious-onset proximal and distal weakness, sensory loss, and areflexia. Nerve
conduction studies reveal a demyelinating pattern of dysfunction, and CSF
studies can show elevated protein levels with normal cell count.
Cranial neuropathies have been reported in patients with Sjögren syndrome;
the trigeminal nerve seems to be more frequently involved, and facial
neuropathy and sensorineural hearing loss have been reported.25,34 These may
occur in isolation or with other peripheral neuropathies. However, the
occurrence of multiple cranial neuropathies with headache or systemic
symptoms should raise suspicion for underlying aseptic meningitis or
CNS vasculitis.
Autonomic symptoms of variable severity, including cardiovascular,
gastrointestinal, or genitourinary symptoms, as well as autonomic dysfunction
on respective testing, have been reported in Sjögren syndrome.25 In the majority
of cases, these are of mild severity, whereas clinically overt, severe, autonomic
neuropathy is less common.35 Autonomic neuropathy may occur in isolation or
may be accompanied by other types of neuropathy, usually sensory.25 The
presence of an Adie tonic pupil in a patient with Sjögren syndrome is suggestive
of underlying autonomic dysfunction and should prompt further evaluation.
Myopathy is uncommon in Sjögren syndrome.34 Inclusion body myositis may
be more frequently associated with Sjögren syndrome; in a case series, Sjögren
syndrome was the most common rheumatologic comorbidity, present in 15% of
patients with inclusion body myositis.36
CNS involvement is less commonly encountered in Sjögren syndrome and
is estimated at 2% to 5%.23,24 This usually comprises focal or multifocal CNS
involvement with corresponding deficits,34 which are usually of acute or
subacute onset due to vasculitis or demyelination.34 Optic neuritis34 and
transverse myelitis can also be seen in patients with Sjögren syndrome,34 as
can overlapping NMOSDs37 or, less frequently, multiple sclerosis (MS).38 Less
common syndromes include aseptic meningitis,34 cerebellar ataxia, focal or
generalized seizures, and a motor neuron disease–like syndrome with a
presentation very similar to amyotrophic lateral sclerosis, although its rate of
progression may be slower.34
Symptomatic treatments for neuropathic pain include topical agents, such as
lidocaine or capsaicin, and oral agents, including gabapentin, pregabalin, or
duloxetine. Tricyclic antidepressants, although efficacious for neuropathic pain
treatment, should be used with caution as they can exacerbate sicca symptoms
because of their anticholinergic properties. Physical therapy is very important in
cases of motor or balance deficits.
No randomized placebo-controlled trials of immunotherapies for peripheral
neuropathies associated with Sjögren syndrome have been conducted.
Mononeuritis multiplex and cases of neuropathy with documented vasculitis are
treated with immunotherapies as in any case of vasculitis, including high-dose
corticosteroids, rituximab, azathioprine, or cyclophosphamide.32 Demyelinating
neuropathy can be treated similarly to CIDP, with steroids and IV immunoglobulin
(IVIg).33 Sensory and sensorimotor axonal polyneuropathy are thought to be
less responsive to immunotherapies; however, some cases have improved after
IVIg treatment.39 Axonal neuropathies associated with Sjögren syndrome and
lymphoma have also been reported to improve after treatment with rituximab,
CONTINUUMJOURNAL.COM 599
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).40
Sensory ataxic neuropathy is the most challenging neuropathy to treat, and
patients typically progress despite receiving various immunotherapies, including
corticosteroids, IVIg, plasma exchange, infliximab, or D-penicillamine.
However, cases showing response to rituximab41 or mycophenolate mofetil
have been reported.42 The treatment of small fiber neuropathy is mostly
symptomatic; however, cases have been reported in which symptoms
responded to IVIg.30,43
CNS disease is treated with high-dose IV corticosteroids, and typically an
additional immunosuppressive agent (eg, cyclophosphamide or rituximab) is
also needed. Although no randomized clinical trials have been conducted,
rituximab is often preferred because of less severe toxicity compared to
cyclophosphamide. Other treatments, including plasma exchange, IVIg,
azathioprine, and mycophenolate mofetil have been tried with mixed results.
RHEUMATOID ARTHRITIS
Cervical spinal stenosis due to synovitis and pannus formation is present more
frequently in patients with rheumatoid arthritis, involving the atlantoaxial,
atlantooccipital, or subaxial level.44 It has been associated with longer duration of
disease and increased disease activity.44 Earlier use of biologics may reduce the
risk and burden of degenerative spine disease.45 Presentations may range from
asymptomatic to severe myelopathy. Respiratory involvement or even sudden
death due to medullary compression can be seen in cases of upper cervical or
occipitocervical involvement.46 In suspected cases, MRI should be obtained, as it
is optimal compared to other modalities in evaluating for pannus formation and
visualizing the spinal cord.46 Surgical intervention is indicated in cases with
myelopathic signs or refractory pain.
Aseptic meningitis is a rare manifestation of rheumatoid arthritis and can lead
to severe neurologic impairment. It is often a later manifestation and may present
in the absence of active systemic disease. Presenting symptoms include altered
mental status, headache, seizures, and, rarely, cerebral infarcts in cases
accompanied by cerebral vasculitis.47 In suspected cases, other causes such as
infection and other autoimmune diseases, including sarcoidosis, systemic
vasculitides, and IgG4-related disease, should be excluded. Apart from
meningeal enhancement, the presence of rheumatoid nodules in the meninges
can be a suggestive finding.48 CSF testing shows lymphocytic pleocytosis and
elevated protein levels. In diagnostically challenging cases, meningeal biopsy
may be needed, which may show inflammatory infiltrates, findings of vasculitis,
or rheumatoid nodules. Treatment usually consists of high-dose IV
corticosteroids and immunomodulatory treatments, such as azathioprine or
cyclophosphamide.49 Cases responsive to rituximab have also been reported.50
Entrapment neuropathies are the most common form of peripheral
neuropathy encountered in rheumatoid arthritis. Carpal tunnel syndrome is the
most common focal neuropathy seen, with patients with rheumatoid arthritis
having a threefold increased risk.51 Axonal sensorimotor polyneuropathy can be
seen less frequently. Demyelinating neuropathy has been reported and is seen
more frequently with the use of tumor necrosis factor-α (TNF-α) inhibitors
(refer to the section on neurologic complications of TNF-α inhibitors).
Mononeuritis multiplex associated with vasculitis can be seen, although this is
rare with earlier use of biologic therapies.
600 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Patients with rheumatoid arthritis have a higher frequency of cardiovascular KEY POINTS
disease, including stroke, and a higher resulting mortality rate.52 This is thought
● Patients with rheumatoid
to derive from a combination of traditional risk factors and systemic arthritis have increased risk
inflammation.52 Management includes lifestyle and traditional vascular risk of cervical spinal stenosis,
factor modification as well as treating the systemic disease, which theoretically particularly at the
should mitigate the atherogenic effects of chronic inflammation; however, atlantooccipital,
atlantoaxial, or subaxial
studies addressing the effect of biologic therapies on cardiovascular disease in
level.
rheumatoid arthritis have yielded mixed results.
● Pannus formation is a
SYSTEMIC VASCULITIDES mechanism by which
Vasculitis can affect the nervous system either in the form of a primary vasculitic patients with rheumatoid
arthritis can develop
syndrome, such as the ones described in this section, or as a manifestation of a cervical spinal stenosis. The
systemic autoimmune disease (such as SLE, Sjögren syndrome, or rheumatoid imaging modality of choice
arthritis). However, the latter is not encountered as frequently as it was to detect it is MRI.
previously, as the immunotherapies used now are more efficacious in controlling
● Mononeuritis multiplex is
these systemic diseases. Peripheral neuropathy is the most frequent neurologic the most common
manifestation seen in primary vasculitic syndromes; it may occur concurrently peripheral neuropathy
with CNS manifestations or in isolation, usually as mononeuritis multiplex associated with vasculitis.
(CASE 3-2) and less frequently as distal symmetric polyneuropathy.53 Clinical Over time, confluent
neurologic deficits can
features suggestive of a vasculitic neuropathy include constitutional symptoms,
mimic a distal symmetric
subacute-onset neurologic deficits corresponding to the individual nerve(s) polyneuropathy.
distribution accompanied by pain, and stepwise progression; however, the
progression may be insidious, and confluent neurologic deficits over time can ● Combined nerve and
mimic a distal symmetric polyneuropathy.53 Elevated erythrocyte sedimentation muscle biopsy increases the
sensitivity for vasculitis
rate and C-reactive protein may be present, as well as cryoglobulins in certain diagnosis.
cases. Electrophysiologic studies show an axonal dysfunction pattern but may
reveal transient pseudoconduction block over the area of nerve infarction, which ● In a patient with known or
later subsides after wallerian degeneration occurs.53 Although often diagnosed suspected systemic
autoimmune disease or
on clinical and electrophysiologic grounds, histopathology can confirm the constitutional symptoms,
diagnosis; in these cases, combined nerve and muscle biopsy is recommended coexisting deficits of
to increase the diagnostic yield. subacute onset that localize
Vasculitis may affect the CNS as a manifestation of an underlying systemic to the central and peripheral
nervous systems should
autoimmune disease (such as SLE, rheumatoid arthritis, or Sjögren syndrome) or
raise the suspicion of
a primary systemic vasculitic syndrome (such as antineutrophil cytoplasmic vasculitis.
antibody [ANCA]–associated vasculitides, polyarteritis nodosa, Takayasu
arteritis, or giant cell arteritis). It should be differentiated from primary CNS
vasculitis, other systemic autoimmune diseases such as neurosarcoidosis, CNS
infections, or demyelinating disease.
The presence of constitutional symptoms and other organ involvement,
including mononeuritis multiplex, is suggestive of a systemic process rather
than a vasculitis confined to the CNS. Clinical presentation consists of acute- or
subacute-onset focal or multifocal deficits. Mental status changes, headache,
or seizures may also be present. Meningeal enhancement, which is often
accompanied by multiple cranial neuropathies, cerebral infarcts, or
hemorrhages, may be present on MRI. CSF studies show lymphocytosis and
elevated protein in the majority of cases and can be helpful in distinguishing from
other causes, such as infections. As MRI and CSF studies often yield nonspecific
findings, vessel imaging can be helpful in confirming the clinical diagnosis.
Magnetic resonance angiography (MRA), CT angiography, and conventional
angiography can show abnormalities in large and medium vessel vasculitides,
CONTINUUMJOURNAL.COM 601
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
CASE 3-2 A 35-year-old man presented to the emergency department reporting
excruciating left dorsal foot pain and left footdrop, which he noticed upon
awakening the day before. He denied ever having problems with back pain or
pain radiating down his legs. Four weeks earlier, he had developed persistent
numbness in the right fourth and fifth fingers. Six months earlier, he had
developed a dry cough and sinusitislike symptoms, which persisted despite
being treated with over-the-counter antihistamines and later a course of
azithromycin. On review of systems, he described having an episode of
hematuria 1 week earlier.
On general examination, his temperature was 38.3°C (101°F), and his vital
signs were otherwise normal. He had a palpable maculopapular
erythematous rash on his distal legs. On neurologic examination, his mental
status and cranial nerves were intact. Strength in the arms was normal except
for right finger abduction and flexion of the fourth and fifth digits, which were
3/5. Strength in the legs was normal except for left ankle dorsiflexion and
eversion, which were 2/5. Sensation was decreased to light touch and
pinprick in the palmar and dorsal aspects of the right fifth digit, the medial
half of the right fourth digit, the left dorsal foot, and left lateral calf. Reflexes
were symmetric, and Babinski sign was absent bilaterally.
Blood work was notable for leukocytosis and elevated blood urea nitrogen
and creatinine levels. Erythrocyte sedimentation rate and C-reactive protein
were elevated, and cytoplasmic antineutrophil cytoplasmic antibodies
(c-ANCA) and cryoglobulins were present. Urinalysis showed proteinuria, and
microscopic analysis showed red blood cell and protein casts.
He was started on IV methylprednisolone for 3 days, and then rituximab
infusions were initiated. He later underwent renal biopsy, which showed
pauci-immune glomerulonephritis and granulomas. Electrodiagnostic studies
done after 3 weeks showed evidence of right ulnar and left common fibular
(peroneal) axonal neuropathies.
COMMENT In this case, the subacute onset and stepwise progression of symptoms
localizing to individual nerve distributions raise the suspicion of a
mononeuritis multiplex. The presence of constitutional symptoms and pain,
which reflects the underlying nerve infarction, as well as vasculitic involvement
of other organs (such as palpable purpura in the skin and glomerulonephritis)
are also typical of systemic vasculitides. In this case, the presence of sinusitis
and renal involvement with pauci-immune glomerulonephritis and c-ANCA are
suggestive of granulomatosis with polyangiitis (previously known as Wegener
granulomatosis). Electrodiagnostic studies in patients with mononeuritis
multiplex reflect the multifocal distribution of symptoms and deficits, showing
axonal dysfunction in the affected nerves. However, electrodiagnostic testing is
not helpful in the acute phase, as abnormalities may not be present during
the first 3 to 4 weeks after symptom onset. In diagnostically challenging
cases, combined nerve and muscle biopsy is recommended to maximize
diagnostic yield. Although the diagnosis of vasculitis is confirmed by
pathology, treatment should be initiated as soon as possible to prevent
permanent neurologic dysfunction and further progression of the disease.
602 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
while their sensitivity is lower in small vessel vasculitides. Novel vessel imaging KEY POINTS
techniques, such as high-resolution vessel wall imaging, are becoming more readily
● Peripheral neuropathy is
available and eventually will provide noninvasive alternative diagnostic modalities. present in more than 50% of
In diagnostically challenging cases, brain or meningeal biopsy may be needed. patients with polyarteritis
nodosa and is often a
Takayasu Arteritis presenting manifestation.
Headache and dizziness are common symptoms in patients with Takayasu
● Pituitary involvement can
arteritis,54 and the frequency of stroke or transient ischemic attacks has been be seen in granulomatosis
estimated to be between 10% and 20%.55 Stenosis or occlusion of large arteries, with polyangiitis.
such as the common carotid or subclavian, is often seen in these cases.54
Intracranial hemorrhage is less common and has been associated with descending
aortic or renal artery stenosis.54 In a series of consecutive patients with Takayasu
arteritis undergoing vessel imaging, 13% of patients had intracranial vessel
abnormalities and cerebral aneurysms were present in 3.9%.56
Temporal Arteritis
Headache is a common presenting symptom of patients with temporal (giant
cell) arteritis. Of patients with temporal arteritis, 30% have been estimated to
sustain permanent vision loss.57 Of cases of vision loss, 90% are due to anterior
ischemic optic neuropathy, followed by central retinal artery occlusion.57 Rarely,
extraocular muscle weakness may coexist because of cranial nerve
involvement.58 Clinical symptoms or ultrasonographic findings of temporal
artery involvement, hypertension, atrial fibrillation, carotid artery stenosis, and
increased CHADS2 (congestive heart failure, hypertension, age 75 years or older,
diabetes mellitus, and previous stroke/transient ischemic attack) score have been
associated with increased risk of visual impairment.57 Patients with temporal
arteritis and involvement of large vessels, such as the aorta and its branches, have
increased risk of stroke and relatively decreased inflammatory markers
compared to patients without large vessel involvement.59 Limb claudication is
also more common in patients with large vessel involvement and may present in
the absence of other manifestations of temporal arteritis.59
Polyarteritis Nodosa
Peripheral neuropathy affects 50% to 70% of patients with polyarteritis nodosa
and in the majority is a presenting manifestation.60 The majority of cases consist
of mononeuritis multiplex, followed less frequently by length-dependent axonal
sensorimotor or sensory polyneuropathy.60 CNS involvement is less common in
polyarteritis nodosa, presenting as headache, encephalopathy, stroke, and,
rarely, intracranial hemorrhage.
ANCA-associated Vasculitides
Peripheral neuropathy is the most common neurologic manifestation of granulomatosis
with polyangiitis (previously known as Wegener granulomatosis); however, cerebral
and meningeal involvement, upper cranial nerve, and pituitary involvement61 are also
seen. These are thought to reflect both vasculitic involvement and granulomatous
spread from the sinuses, which are a typical site of disease involvement. Cases with
pituitary involvement should be differentiated from tuberculosis, neurosarcoidosis,
Crohn disease, giant cell arteritis, and IgG4-related systemic disease.
Peripheral neuropathy, usually in the form of mononeuritis multiplex and less
commonly in the form of distal symmetric polyneuropathy, seems to be more
CONTINUUMJOURNAL.COM 603
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
frequently seen in eosinophilic granulomatosis with polyangiitis compared to the
other small vessel vasculitides.62 CNS involvement is rare in eosinophilic
granulomatosis with polyangiitis and microscopic polyangiitis.63
BEHÇET DISEASE
Behçet disease can affect the CNS in 3% to 10% of patients, whereas peripheral
neuropathy is rare, seen in 0.3% of patients.64 The majority of patients with CNS
manifestations present with parenchymal involvement due to small vessel
vasculitis, whereas 20% of patients with neuro-Behçet disease develop cerebral
venous sinus thrombosis.65 Interestingly, parenchymal disease and cerebral
venous sinus thrombosis tend not to coexist in the same patient. Symptom onset
in cerebral venous sinus thrombosis is typically insidious, as only 10% of patients
present with acute symptoms; in two-thirds of patients, concurrent peripheral
thrombotic events are present, usually deep vein thrombosis in the legs.65
Parenchymal disease typically manifests as a subacute, progressive brainstem
syndrome. Typical MRI findings include brainstem T2 hyperintensities, often
extending to the diencephalon, followed by atrophy and necrosis.66
Myelitis has been rarely described in patients with Behçet disease; this has been
reported to occur either later in the course of the disease or as a presenting
manifestation and tends to be accompanied with uveitis.67 The majority of the
reported cases were treated with corticosteroids and cyclophosphamide, with
mixed results.67
Optic neuritis is another uncommon manifestation of Behçet disease.
Compared to other neurologic syndromes, it is more likely to be the presenting
manifestation of the disease, as half of cases may be present before the onset of
systemic manifestations.68 Uveitis is often an associated comorbidity. About
one-third of patients have been reported to have concurrent neurologic
involvement in the form of parenchymal disease or MS-like syndromes, and one
case of optic neuritis occurring along with longitudinally extensive myelitis and
negative AQP4 antibodies has been reported.68
SCLERODERMA
Myopathy is a common neuromuscular manifestation seen in patients with both
systemic sclerosis and localized scleroderma69; however, this can be difficult to
distinguish from overlapping primary inflammatory myopathies in many cases.
Focal and generalized seizures have been associated with limited scleroderma.70
Brain MRI may show increased white matter lesion burden.70 Focal neurologic
signs and cranial neuropathies can be seen less commonly69; although vasculitis
can complicate scleroderma, CNS vasculitis is rare.71
Peripheral neuropathy has been reported in 5% of patients with scleroderma,
after excluding confounding etiologies.72 Autonomic dysfunction of variable
degree is also seen, in the form of gastrointestinal symptoms, abnormal
gastrointestinal motility testing,73 or abnormal cardiovascular reflex testing.74
SERONEGATIVE SPONDYLARTHROPATHIES
Patients with ankylosing spondylitis are at increased risk of nerve root
compression ranging from symptomatic radiculopathy to cauda equina
syndrome as a result of vertebral fractures,75 local degenerative changes, dural
ectasia, or tethering.76 Patients with psoriatic arthritis have increased prevalence
of vascular risk factors.77 Patients with ankylosing spondylitis or psoriatic
604 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
arthritis have a higher risk of cardiovascular disease, including a slightly higher KEY POINTS
risk of stroke compared to the general population.78
● Cerebral venous sinus
thrombosis is associated
COGNITIVE DYSFUNCTION AND RHEUMATIC DISEASES with Behçet disease and is
Cognitive symptoms are among the most common neurologic symptoms in often of insidious onset.
patients with systemic autoimmune diseases,79 ranging from mild, ill-defined,
● Cognitive symptoms are
cognitive dysfunction often termed brain fog to more severe cognitive symptoms.
common among patients
The lack of objective tests can make the evaluation and classification of these with systemic autoimmune
symptoms difficult in day-to-day clinical practice. Overall, patient-reported diseases, ranging from mild
symptoms tend to be more prevalent than neuropsychiatric syndromes subjective cognitive
diagnosed by various objective testing methods.80 Chronic somatic symptoms, symptoms to more severe
cognitive dysfunction.
including pain, and systemic inflammation are confounding factors contributing
to patient-reported symptoms and further complicate their evaluation. In ● Patients with rapidly
cases of rapidly progressing cognitive dysfunction, it is important to rule out progressing cognitive
concurrent neurologic syndromes, such as aseptic meningitis, CNS vasculitis, or decline should be evaluated
for other central nervous
other neurologic processes (eg, infections, autoimmune encephalitis, or prion system processes, such as
diseases), which can present in a similar manner. As in every patient with vasculitis, infections,
cognitive symptoms, thyroid function and vitamin B12 levels should be assessed, aseptic meningitis,
especially given the increased frequency of coexisting Hashimoto thyroiditis autoimmune encephalitis, or
prion diseases.
and atrophic gastritis in patients with systemic autoimmune diseases.
SLE has been extensively studied, and patients with SLE seem to have ● Cognitive dysfunction is
increased risk of both cognitive dysfunction and dementia, according to a seen more frequently in
number of studies.81 Cognitive dysfunction has been reported at similar rates systemic lupus
in Sjögren syndrome79 and less frequently in rheumatoid arthritis.81,82 erythematosus and Sjögren
syndrome, followed by
Cognitive symptoms have been less extensively investigated compared to other rheumatoid arthritis.
manifestations of rheumatologic diseases; however, available studies suggest that
cognitive dysfunction may correlate with disease activity in SLE83 and rheumatoid ● Tumor necrosis factor-α
arthritis.84 The underlying pathogenic mechanisms remain largely unknown, inhibitors can cause
central demyelination or
although limited evidence indicates that hypoperfusion may be associated with demyelinating neuropathies.
cognitive dysfunction, suggesting that microvasculopathy could be a potential
pathogenetic mechanism.85 Autoantibodies, such as NR2 glutamate receptor
antibodies,86 ribosomal P protein antibodies,87 and M1 muscarinic acetylcholine
receptor antibodies,88 have been identified in subsets of patients with SLE or Sjögren
syndrome and CNS involvement and have been found to cause neuronal
dysfunction in animal models. However, they have poor specificity in distinguishing
between neuropsychiatric manifestations,86 and their clinical utility remains limited.
Overall, these observations suggest that intrinsic pathogenic mechanisms
likely exist in autoimmune diseases leading to cognitive dysfunction, which are
further augmented by comorbid chronic pain, depression, or the effects of
chronic disease on cognition. However, the presence of confounding factors and
lack of reliable biomarkers hinder our ability to further classify and
systematically study the cognitive symptoms of these patients.
NEUROLOGIC COMPLICATIONS OF TUMOR NECROSIS
FACTOR-α INHIBITORS
Central and peripheral demyelinating syndromes have been associated with
TNF-α inhibitors. Although initial animal studies showed encouraging results in
treatment of experimental autoimmune encephalomyelitis, subsequent clinical
trials in patients with MS showed that TNF-α inhibition increased disease activity
and worsened patient outcomes.89 Various demyelinating syndromes of the CNS
CONTINUUMJOURNAL.COM 605
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
KEY POINT have been reported in patients with rheumatologic diseases, mostly after
treatment with etanercept and infliximab, which constitute more than 80% of
● Demyelinating
neuropathy associated with
reported cases.90 Adalimumab has less commonly been associated with central
tumor necrosis factor-α demyelinating syndromes (16% of reported cases), while only 1% of reported cases
inhibitors persists after their were treated with golimumab.90 Time of neurologic symptom onset from
cessation and requires initiation of treatment can vary widely, from days to years, but the median time
treatment with IV
of onset has been reported to range between 5 and 17 months.90,91 The majority of
immunoglobulin.
the demyelinating syndromes reported were MS-like syndromes, optic neuritis,
and, less commonly, transverse myelitis or tumefactive demyelinating lesions.91
Rarely, progressive multifocal leukoencephalopathy has been reported after
TNF-α inhibitor treatment.92 In 36% of demyelinating events, full recovery was
reported after discontinuing treatment, while 21% achieved partial recovery; in 28%
neurologic symptoms persisted, and three fatalities were reported, two cases with
progressive multifocal leukoencephalopathy and one with an MS-like syndrome.90
Apart from central demyelination, TNF-α inhibitors have also been associated
with peripheral demyelination; clinical and electrophysiologic findings and CSF
studies are identical to CIDP.93 Demyelinating neuropathy may appear early or late
in the course of treatment and persists despite discontinuation of TNF-α
inhibitors.93 Response to corticosteroids is poor, and treatment with IVIg is
required.93 Other types of neuropathy, including multifocal motor neuropathy
(MMN) with conduction block,94 sensory polyradiculopathy,95 and small fiber
neuropathy,96 have also been reported to occur after treatment with TNF-α
inhibitors. Motor neuropathy and sensory polyradiculopathy cases were reported
to improve with IVIg treatment, whereas in small fiber neuropathies, symptoms
improved after discontinuing TNF-α inhibitors.
CONCLUSION
Neurologic manifestations of systemic autoimmune diseases pose a number of
challenges to clinicians; many of these manifestations are rare and present before
the development of or in the absence of active systemic disease. In addition,
significant overlap exists with other primary neurologic disorders or adverse
effects of biologic therapies used to treat the systemic disease. Neurologic
manifestations of rheumatologic diseases are important to recognize as they can
be associated with increased morbidity or even mortality; patients may require
closer monitoring for certain complications. In addition, a subset of these
manifestations can be rapidly progressive and, if not treated early, can lead to
significant irreversible neurologic dysfunction and resulting morbidity.
Therefore, increased awareness and multidisciplinary care are required to
diagnose and institute treatment in a timely manner.
REFERENCES
1 ACR Ad Hoc Committee on Neuropsychiatric 2 Hanly JG, Li Q, Su L, et al. Psychosis in systemic
Lupus Nomenclature. The American College of lupus erythematosus: results from an
Rheumatology nomenclature and case International Inception Cohort Study. Arthritis
definitions for neuropsychiatric lupus Rheum 2019;71(2):281–9. doi:10.1002/art.40764.
syndromes. Arthritis Rheum 1999;42(4):599–608.
doi:10.1002/1529-0131(199904)42:4<599::
AID-ANR2>3.0.CO;2-F.
606 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
3 Zirkzee E, Huizinga T, Bollen E, et al. Mortality in 15 Asgari N, Jarius S, Laustrup H, et al. Aquaporin-4-
neuropsychiatric systemic lupus erythematosus autoimmunity in patients with systemic lupus
(NPSLE). Lupus 2014;23(1):31–38. doi: erythematosus: a predominantly population-
10.1177/0961203313512540. based study. Mult Scler 2018;24(3):331–339.
doi:10.1177/1352458517699791.
4 Hanly JG. Diagnosis and management of
neuropsychiatric SLE. Nat Rev Rheumatol 2014; 16 de Andrade FA, Guimarães Moreira Balbi G,
10(6):338–347. doi:10.1038/nrrheum.2014.15. Bortoloti de Azevedo LG, et al. Neuro-
ophthalmologic manifestations in systemic lupus
5 Mitsikostas DD, Sfikakis PP, Goadsby PJ. A meta-
erythematosus. Lupus 2017;26(5):522–528.
analysis for headache in systemic lupus
doi:10.1177/0961203316683265.
erythematosus: the evidence and the myth. Brain
2004;127(pt 5):1200–1209. doi:10.1093/brain/awh146. 17 Oomatia A, Fang H, Petri M, Birnbaum J.
Peripheral neuropathies in systemic lupus
6 Kwan A, Marzouk S, Ghanean H, et al. Assessment
erythematosus: clinical features, disease
of the psychometric properties of patient-
associations, and immunologic characteristics
reported outcomes of depression and anxiety in
evaluated over a twenty-five-year study period.
systemic lupus erythematosus. Semin Arthritis
Arthritis Rheumatol 2014;66(4):1000–1009.
Rheum 2019;49(2):260–266. doi:10.1016/j.
doi:10.1002/art.38302.
semarthrit.2019.03.004.
18 Fanouriakis A, Kostopoulou M, Alunno A, et al.
7 Hanly JG, Su L, Urowitz MB, et al. Mood disorders
2019 Update of the EULAR recommendations
in systemic lupus erythematosus: results from an
for the management of systemic lupus
international inception cohort study. Arthritis
erythematosus. Ann Rheum Dis 2019;78(6):
Rheumatol 2015;67(7):1837–1847. doi:10.1002/
736–745. doi:10.1136/annrheumdis-2019-215089.
art.39111.
19 Fanouriakis A, Pamfil C, Sidiropoulos P, et al.
8 Hanly JG, Li Q, Su L, et al. Cerebrovascular events
Cyclophosphamide in combination with
in systemic lupus erythematosus: results from an
glucocorticoids for severe neuropsychiatric
international inception cohort study. Arthritis
systemic lupus erythematosus: a retrospective,
Care Res (Hoboken) 2018;70(10):1478–1487.
observational two-centre study. Lupus 2016;
doi:10.1002/acr.23509.
25(6):627–636. doi:10.1177/0961203315622821.
9 Barbhaiya M, Feldman CH, Guan H, et al. Racial/
20 Iwata S, Saito K, Hirata S, et al. Efficacy and safety
ethnic variation in stroke rates and risks among
of anti-CD20 antibody rituximab for patients with
patients with systemic lupus erythematosus.
refractory systemic lupus erythematosus. Lupus
Semin Arthritis Rheum 2019;48(5):840–846.
2018;27(5):802–811. doi:10.1177/0961203317749047.
doi:10.1016/j.semarthrit.2018.07.012.
21 Flanagan EP. Neuromyelitis optica spectrum
10 Hanly JG, Urowitz MB, Su L, et al. Seizure
disorder and other non–multiple sclerosis central
disorders in systemic lupus erythematosus
nervous system inflammatory diseases. Continuum
results from an international, prospective,
(Minneap Minn) 2019;25(3, Multiple Sclerosis and
inception cohort study. Ann Rheum Dis 2012;71(9):
Other CNS Inflammatory Diseases):815–844.
1502–1509. doi:10.1136/annrheumdis-2011-201089.
doi:10.1212/CON.0000000000000742.
11 Merayo-Chalico J, Apodaca E, Barrera-Vargas A,
22 Pavlakis P, Alexopoulos H, Kosmidis M, et al.
et al. Clinical outcomes and risk factors for
Peripheral neuropathies in Sjögren’s syndrome:
posterior reversible encephalopathy syndrome
a critical update on clinical features and
in systemic lupus erythematosus: a multicentric
pathogenetic mechanisms. J Autoimmun 2012;
case-control study. J Neurol Neurosurg
39(1–2):27–33. doi:10.1016/j.jaut.2012.01.003.
Psychiatry 2016;87(3):287–294. doi:10.1136/jnnp-
2014-310145. 23 Carvajal Alegria G, Guellec D, et al. Epidemiology
of neurological manifestations in Sjogren’s
12 Damrongpipatkul U, Oranratanachai K, Kasitanon
syndrome: data from the French ASSESS cohort.
N, et al. Clinical features, outcome, and
RMD Open 2016;2(1):e000179. doi:10.1136/
associated factors for posterior reversible
rmdopen-2015-000179.
encephalopathy in Thai patients with systemic
lupus erythematosus: a case-control study. 24 Ramos-Casals M, Solans R, Rosas J, et al. Primary
Clin Rheumatol 2018;37(3):691–702. doi:10.1007/ Sjogren syndrome in Spain: clinical and
s10067-017-3892-2. immunologic expression in 1010 patients.
Medicine (Baltimore) 2008;87(4):210–219.
13 Costallat BL, Ferreira DM, Costallat LT,
doi:10.1097/MD.0b013e318181e6af.
Appenzeller S. Myelopathy in systemic lupus
erythematosus: clinical, laboratory, radiological 25 Mori K, Iijima M, Koike H, et al. The wide spectrum
and progression findings in a cohort of 1,193 of clinical manifestations in Sjögren's syndrome-
patients [Article in English, Portuguese]. Rev Bras associated neuropathy. Brain 2005;128(pt 11):
Reumatol Engl Ed 2016;56(3):240–251. doi:10.1016/ 2518–2534. doi:10.1093/brain/awh605.
j.rbre.2016.03.006.
26 Pavlakis PP, Alexopoulos H, Kosmidis ML, et al.
14 Birnbaum J, Petri M, Thompson R, et al. Peripheral neuropathies in Sjögren syndrome: a
Distinct subtypes of myelitis in systemic lupus new reappraisal. J Neurol Neurosurg Psychiatry
erythematosus. Arthritis Rheum 2009;60(11): 2011;82(7):798–802. doi:10.1136/jnnp.2010.222109.
3378–3387. doi:10.1002/art.24937.
CONTINUUMJOURNAL.COM 607
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
27 Ioannidis JP, Vassiliou VA, Moutsopoulos HM. 39 Rist S, Sellam J, Hachulla E, et al. Experience
Long-term risk of mortality and lymphoproliferative of intravenous immunoglobulin therapy in
disease and predictive classification of primary neuropathy associated with primary Sjogren's
Sjögren's syndrome. Arthritis Rheum 2002;46(3): syndrome: a national multicentric retrospective
741–747. doi:10.1002/art.10221. study. Arthritis Care Res (Hoboken) 2011;63(9):
1339–1344. doi:10.1002/acr.20495.
28 Sene D, Cacoub P, Authier FJ, et al. Sjögren
syndrome-associated small fiber neuropathy: 40 Voulgarelis M, Giannouli S, Tzioufas AG,
characterization from a prospective series of Moutsopoulos HM. Long term remission of
40 cases. Medicine 2013;92(5):e10–e18. Sjögren's syndrome associated aggressive
doi:10.1097/MD.0000000000000005. B cell non-Hodgkin’s lymphomas following
combined B cell depletion therapy and CHOP
29 Malinow K, Yannakakis GD, Glusman SM, et al.
(cyclophosphamide, doxorubicin, vincristine,
Subacute sensory neuronopathy secondary to
prednisone). Ann Rheum Dis 2006;65(8):
dorsal root ganglionitis in primary Sjögren’s
1033–1037. doi:10.1136/ard.2005.046193.
syndrome. Ann Neurol 1986;20(4):535–537.
doi:10.1002/ana.410200416. 41 Gorson KC, Natarajan N, Ropper AH, Weinstein R.
Rituximab treatment in patients with
30 Birnbaum J, Duncan T, Owoyemi K, et al. Use
IVIg-dependent immune polyneuropathy: a
of a novel high-resolution magnetic resonance
prospective pilot trial. Muscle Nerve 2007;35(1):
neurography protocol to detect abnormal dorsal
66–69. doi:10.1002/mus.20664.
root Ganglia in Sjögren patients with neuropathic
pain: case series of 10 patients and review of 42 Pereira PR, Viala K, Maisonobe T, et al. Sjögren
the literature. Medicine 2014;93(3):121–134. sensory neuronopathy (Sjögren ganglionopathy):
doi:10.1097/MD.0000000000000024. long-term outcome and treatment response in a
series of 13 cases. Medicine 2016;95(19):e3632.
31 Skopouli FN, Dafni U, Ioannidis JP, Moutsopoulos
doi:10.1097/MD.0000000000003632.
HM. Clinical evolution, and morbidity and
mortality of primary Sjögren’s syndrome. Semin 43 Morozumi S, Kawagashira Y, Iijima M, et al.
Arthritis Rheum 2000;29(5):296–304. doi:10.1016/ Intravenous immunoglobulin treatment for
s0049-0172(00)80016-5. painful sensory neuropathy associated with
Sjögren’s syndrome. J Neurol Sci 2009;279(1–2):
32 Terrier B, Lacroix C, Guillevin L, et al. Diagnostic
57–61. doi:10.1016/j.jns.2008.12.018.
and prognostic relevance of neuromuscular
biopsy in primary Sjögren’s syndrome-related 44 Younes M, Belghali S, Kriâa S, et al. Compared
neuropathy. Arthritis Rheum 2007;57(8): imaging of the rheumatoid cervical spine:
1520–1529. doi:10.1002/art.23102. Prevalence study and associated factors. Joint
Bone Spine 2009;76(4):361–368. doi:10.1016/j.
33 Sanvito L, Wong SL, Rajabally YA. Chronic
jbspin.2008.10.010.
inflammatory demyelinating polyneuropathy
associated with alopecia totalis and Sjögren 45 Kauppi MJ, Neva MH, Laiho K, et al. Rheumatoid
syndrome. Muscle Nerve 2012;45(5):762–763. atlantoaxial subluxation can be prevented by
doi:10.1002/mus.23339. intensive use of traditional disease modifying
antirheumatic drugs. J Rheumatol 2009;36(2):
34 Delalande S, de Seze J, Fauchais AL, et al.
273–278. doi:10.3899/jrheum.080429.
Neurologic manifestations in primary Sjögren
syndrome: a study of 82 patients. Medicine 46 DeQuattro K, Imboden JB. Neurologic
(Baltimore) 2004;83(5):280–291. doi:10.1097/01. manifestations of rheumatoid arthritis. Rheum
md.0000141099.53742.16. Dis Clin North Am 2017;43(4):561–571. doi:10.1016/j.
rdc.2017.06.005.
35 Wright RA, Grant IA, Low PA. Autonomic
neuropathy associated with sicca complex. 47 Schuster S, Braass H, Iking-Konert C, et al.
J Auton Nerv Syst 1999;75(1):70–76. doi:10.1016/ Rheumatoid meningitis: a rare cause of aseptic
s0165-1838(98)00164-7. meningitis with frequently stroke-like episodes.
Neurol Clin Pract 2018;8(5):451–455. doi:10.1212/
36 Dobloug GC, Antal EA, Sveberg L, et al. High
CPJ.0000000000000504.
prevalence of inclusion body myositis in Norway;
a population-based clinical epidemiology study. 48 Matsushima M, Yaguchi H, Niino M, et al. MRI and
Eur J Neurol 2015;22(4):672-e41. doi:10.1111/ pathological findings of rheumatoid meningitis.
ene.12627. J Clin Neurosci 2010;17(1):129–132. doi:10.1016/j.
jocn.2009.01.033.
37 Pittock SJ, Lennon VA, de Seze J, et al.
Neuromyelitis optica and non organ-specific 49 Kato T, Hoshi K-i, Sekijima Y, et al. Rheumatoid
autoimmunity. Arch Neurol 2008;65(1):78–83. meningitis: an autopsy report and review of the
doi:10.1001/archneurol.2007.17. literature. Clin Rheumatol 2003;22(6):475–480.
doi:10.1007/s10067-003-0788-0.
38 Annunziata P, De Santi L, Di Rezze S, et al. Clinical
features of Sjogren’s syndrome in patients with 50 Harrison NS, Kishore S, Majithia V. Rheumatoid
multiple sclerosis. Acta Neurol Scand 2011;124(2): meningitis: successful remission with rituximab.
109–114. doi:10.1111/j.1600-0404.2010.01428.x. BMJ Case Rep 2018;11(1):pii: e226642. doi:10.1136/
bcr-2018-226642.
608 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
51 Shiri R. Arthritis as a risk factor for carpal 65 Shi J, Huang X, Li G, et al. Cerebral venous sinus
tunnel syndrome: a meta-analysis. Scand J thrombosis in Behçet’s disease: a retrospective
Rheumatol 2016;45(5):339–346. doi:10. case-control study. Clin Rheumatol 2018;37(1):
3109/03009742.2015.1114141. 51–57. doi:10.1007/s10067-017-3718-2.
52 Blum A, Adawi M. Rheumatoid arthritis (RA) and 66 Borhani Haghighi A, Sarhadi S, Farahangiz S. MRI
cardiovascular disease. Autoimmun Rev 2019; findings of neuro-Behcet’s disease. Clin
18(7):679–690. doi:10.1016/j.autrev.2019.05.005. Rheumatol 2011;30(6):765–770. doi:10.1007/
s10067-010-1650-9.
53 Gwathmey KG, Burns TM, Collins MP, Dyck PJ.
Vasculitic neuropathies. Lancet Neurol 2014;13(1): 67 Bitik B, Ucar M, Tezcan ME, et al. Transverse
67–82. doi:10.1016/S1474-4422(13)70236-9. myelitis in Behcet's disease: a series of four
cases and review of the literature. Clin Exp
54 Yang L, Zhang H, Jiang X, et al. Clinical features
Rheumatol 2013;31(3 suppl 77):20–24.
and outcomes of Takayasu arteritis with
neurological symptoms in China: a retrospective 68 Akdal G, Toydemir HE, Saatci AO, et al.
study. J Rheumatol 2015;42(10):1846–1852. Characteristics of optic neuropathy in Behçet
doi:10.3899/jrheum.150097. disease. Neurol Neuroimmunol Neuroinflamm
2018;5(5):e490. doi:10.1212/NXI.0000000000000490.
55 Duarte MM, Geraldes R, Sousa R, et al. Stroke and
transient ischemic attack in Takayasu’s arteritis: a 69 Amaral TN, Peres FA, Lapa AT, et al. Neurologic
systematic review and meta-analysis. J Stroke involvement in scleroderma: a systematic
Cerebrovasc Dis 2016;25(4):781–791. doi:10.1016/j. review. Semin Arthritis Rheum 2013;43(3):
jstrokecerebrovasdis.2015.12.005. 335–347. doi:10.1016/j.semarthrit.2013.05.002.
56 Bond KM, Nasr D, et al. Intracranial and 70 Tollefson MM, Witman PM. En coup de sabre
extracranial neurovascular manifestations of morphea and Parry-Romberg syndrome: a
Takayasu arteritis. AJNR Am J Neuroradiol 2017; retrospective review of 54 patients. J Am Acad
38(4):766–772. doi:10.3174/ajnr.A5095. Dermatol 2007;56(2):257–263. doi:10.1016/j.
jaad.2006.10.959.
57 Czihal M, Tschaidse J, Bernau C, et al. Ocular
ischaemic complications in giant cell arteritis: 71 Abers MS, Iluonakhamhe EK, Goldsmith CE, Kass
CHADS2-score predicts risk of permanent JS. Central nervous system vasculitis secondary
visual impairment. Clin Exp Rheumatol to systemic sclerosis. J Clin Neurosci 2013;20(8):
2019;37 suppl 17(2):61–64. 1168–1170. doi:10.1016/j.jocn.2012.09.022.
58 Ross M, Bursztyn L, Superstein R, Gans M. 72 Paik JJ, Mammen AL, Wigley FM, et al.
Multiple cranial nerve palsies in giant cell Symptomatic and electrodiagnostic features of
arteritis. J Neuroophthalmol 2017;37(4):398–400. peripheral neuropathy in scleroderma. Arthritis
doi:10.1097/WNO.0000000000000529. Care Res (Hoboken) 2016;68(8):1150–1157.
doi:10.1002/acr.22818.
59 de Boysson H, Liozon E, Espitia O, et al. Different
patterns and specific outcomes of large-vessel 73 Zikos TA, Clarke JO, Triadafilopoulos G, et al. A
involvements in giant cell arteritis. J Autoimmun positive correlation between gastric and
2019;103:102283. doi:10.1016/j.jaut.2019.05.011. esophageal dysmotility suggests common
causality. Dig Dis Sci 2018;63(12):3417–3424.
60 de Boysson H, Guillevin L. Polyarteritis nodosa
doi:10.1007/s10620-018-5175-4.
neurologic manifestations. Neurol Clin 2019;37(2):
345–357. doi:10.1016/j.ncl.2019.01.007. 74 Rodrigues GD, Tobaldini E, Bellocchi C, et al.
Cardiac autonomic modulation at rest and during
61 Kapoor E, Cartin-Ceba R, Specks U, et al. Pituitary
orthostatic stress among different systemic
dysfunction in granulomatosis with polyangiitis:
sclerosis subsets. Eur J Intern Med 2019;66:
the Mayo Clinic experience. J Clin Endocrinol
75–80. doi:10.1016/j.ejim.2019.06.003.
Metabol 2014;99(11):3988–3994. doi:10.1210/
jc.2014-1962. 75 Werner BC, Samartzis D, Shen FH. Spinal
fractures in patients with ankylosing spondylitis:
62 Cattaneo L, Chierici E, Pavone L, et al. Peripheral
etiology, diagnosis, and management. J Am Acad
neuropathy in Wegener's granulomatosis,
Orthop Surg 2016;24(4):241–249. doi:10.5435/
Churg-Strauss syndrome and microscopic
JAAOS-D-14-00149.
polyangiitis. J Neurol Neurosurg Psychiatry 2007;
78(10):1119–1123. doi:10.1136/jnnp.2006.111013. 76 Ha SW, Son BC. Cauda equina syndrome
associated with dural ectasia in chronic
63 Adams HP Jr. Cerebral vasculitis. Handb Clin
ankylosing spondylitis. J Korean Neurosurg Soc
Neurol 2014;119:475–494. doi:10.1016/B978-0-
2014;56(6):517–520. doi:10.3340/jkns.2014.56.
7020-4086-3.00031-X.
6.517.
64 Davatchi F, Shahram F, Chams-Davatchi C, et al.
77 Husted JA, Thavaneswaran A, Chandran V, et al.
Behcet’s disease in Iran: analysis of 6500 cases.
Cardiovascular and other comorbidities in
Int J Rheum Dis 2010;13(4):367–373. doi:10.1111/
patients with psoriatic arthritis: a comparison
j.1756-185X.2010.01549.x.
with patients with psoriasis. Arthritis Care Res
(Hoboken) 2011;63(12):1729–1735. doi:10.1002/
acr.20627.
CONTINUUMJOURNAL.COM 609
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
RHEUMATOLOGIC DISORDERS
78 Bengtsson K, Forsblad-d'Elia H, Lie E, et al. Are 87 Ho RC, Thiaghu C, Ong H, et al. A meta-analysis of
ankylosing spondylitis, psoriatic arthritis and serum and cerebrospinal fluid autoantibodies in
undifferentiated spondyloarthritis associated neuropsychiatric systemic lupus erythematosus.
with an increased risk of cardiovascular events? Autoimmun Rev 2016;15(2):124–138. doi:10.1016/j.
A prospective nationwide population-based autrev.2015.10.003.
cohort study. Arthritis Res Ther 2017;19(1):102.
88 Reina S, Sterin-Borda L, Orman B, Borda E.
doi:10.1186/s13075-017-1315-z.
Autoantibodies against cerebral muscarinic
79 Harboe E, Tjensvoll AB, Maroni S, et al. cholinoceptors in Sjögren syndrome: functional
Neuropsychiatric syndromes in patients with and pathological implications. J Neuroimmunol
systemic lupus erythematosus and primary 2004;150(1–2):107–115. doi:10.1016/j.
Sjögren syndrome: a comparative population- jneuroim.2004.01.019.
based study. Ann Rheum Dis 2009;68(10):
89 TNF neutralization in MS: results of a
1541–1546. doi:10.1136/ard.2008.098301.
randomized, placebo-controlled multicenter
80 Shin SY, Katz P, Julian L. Relationship between study. The Lenercept Multiple Sclerosis Study
perceived cognitive dysfunction and objective Group and The University of British Columbia
neuropsychological performance in persons with MS/MRI Analysis Group. Neurology 1999;53(3):
rheumatoid arthritis. Arthritis Care Res (Hoboken) 457–465. doi:10.1212/WNL.53.3.457.
2013;65(3):481–486. doi:10.1002/acr.21814.
90 Kemanetzoglou E, Andreadou E. CNS
81 Rayes HA, Tani C, Kwan A, et al. What is the demyelination with TNF-α blockers. Curr
prevalence of cognitive impairment in lupus and Neurol Neurosci Rep 2017;17(4):36. doi:10.1007/
which instruments are used to measure it? A s11910-017-0742-1.
systematic review and meta-analysis. Semin
91 Mohan N, Edwards ET, Cupps TR, et al.
Arthritis Rheum 2018;48(2):240–255. doi:10.1016/j.
Demyelination occurring during anti-tumor
semarthrit.2018.02.007.
necrosis factor alpha therapy for inflammatory
82 Meade T, Manolios N, Cumming SR, et al. arthritides. Arthritis Rheum 2001;44(12):
Cognitive impairment in rheumatoid arthritis: a 2862–2869. doi:10.1002/1529-0131(200112)44:
systematic review. Arthritis Care Res 2018;70(1): 12<2862::aid-art474>3.0.co;2-w.
39–52. doi:10.1002/acr.23243.
92 Molloy ES, Calabrese LH. Progressive multifocal
83 Lopez-Longo FJ, Carol N, Almoguera MI, et al. leukoencephalopathy associated with immuno-
Cerebral hypoperfusion detected by SPECT in suppressive therapy in rheumatic diseases:
patients with systemic lupus erythematosus is evolving role of biologic therapies. Arthritis
related to clinical activity and cumulative tissue Rheum 2012;64(9):3043–3043. doi:10.1002/
damage. Lupus 2003;12(11):813–819. doi: art.34468.
10.1191/0961203303lu470oa.
93 Alshekhlee A, Basiri K, Miles JD, et al. Chronic
84 Lee JH, Kim GT, Kim YK, Lee SG. Cognitive inflammatory demyelinating polyneuropathy
function of patients with rheumatoid arthritis is associated with tumor necrosis factor-alpha
associated with disease activity but not carotid antagonists. Muscle Nerve 2010;41(5):723–727.
atherosclerotic changes. Clin Exp Rheumatol doi:10.1002/mus.21584.
2018;36(5):856–861.
94 Rowan CR, Tubridy N, Cullen G. Multifocal motor
85 Le Guern V, Belin C, Henegar C, et al. Cognitive neuropathy associated with infliximab. J Crohns
function and 99mTc-ECD brain SPECT are Colitis 2015;9(12):1174–1175. doi:10.1093/ecco-jcc/
significantly correlated in patients with primary jjv137.
Sjögren syndrome: a case-control study.
95 Naruse H, Nagashima Y, Maekawa R, et al.
Ann Rheum Dis 2010;69(1):132–137. doi:10.1136/
Successful treatment of infliximab-associated
ard.2008.090811.
immune-mediated sensory polyradiculopathy
86 Tay SH, Fairhurst A-M, Mak A. Clinical utility of with intravenous immunoglobulin. J Clin Neurosci
circulating anti-N-methyl-D-aspartate receptor 2013;20(11):1618–1619. doi:10.1016/j.jocn.2012.12.016.
subunits NR2A/B antibody for the diagnosis of
96 Birnbaum J, Bingham CO 3rd. Non-length-
neuropsychiatric syndromes in systemic lupus
dependent and length-dependent small-fiber
erythematosus and Sjögren's syndrome: an
neuropathies associated with tumor necrosis
updated meta-analysis. Autoimmun Rev 2017;
factor (TNF)-inhibitor therapy in patients with
16(2):114–122. doi:10.1016/j.autrev.2016.12.002.
rheumatoid arthritis: expanding the spectrum
of neurological disease associated with
TNF-inhibitors. Semin Arthritis Rheum 2014;43(5):
638–647. doi:10.1016/j.semarthrit.2013.10.007.
610 JUNE 2020
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- Cerebral Herniation Syndromes and Intracranial HypertensionFrom EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNo ratings yet
- Corporate CollusionDocument118 pagesCorporate CollusionfbomxdijzyorNo ratings yet
- Treatment Algorithm For Multiple Sclerosis Disease Modifying TherapiesDocument22 pagesTreatment Algorithm For Multiple Sclerosis Disease Modifying TherapiesDiana StancaNo ratings yet
- Vital SignsDocument10 pagesVital SignslisalovNo ratings yet
- Omicron & Delta Viruses Infection Long Hauler Symptoms Diagnosis Patients and Physicians Management HandbookFrom EverandOmicron & Delta Viruses Infection Long Hauler Symptoms Diagnosis Patients and Physicians Management HandbookNo ratings yet
- Insomnia in The Elderly 123Document8 pagesInsomnia in The Elderly 123lalaNo ratings yet
- Focal Epilepsy Causes and Clinical Features - UpToDateDocument44 pagesFocal Epilepsy Causes and Clinical Features - UpToDateBenjamínGalvanNo ratings yet
- CEFALEA Evaluation of Headache in Adults - UpToDateDocument23 pagesCEFALEA Evaluation of Headache in Adults - UpToDateJOSE ANTONIO ALBARRAN MENDOZANo ratings yet
- Vasculitis and NeuropathiesDocument14 pagesVasculitis and Neuropathiesjawad.melhem100% (1)
- 26 - Tic Disorders in ChildhoodDocument12 pages26 - Tic Disorders in ChildhoodAnastasia RaileanNo ratings yet
- Chronic Traumatic Encephalopathy.12Document21 pagesChronic Traumatic Encephalopathy.12wmtxbbNo ratings yet
- Primary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersDocument10 pagesPrimary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Traumatic Brain Injury & Post Concussion Syndrome:Do's & Dont's A Personal JourneyFrom EverandTraumatic Brain Injury & Post Concussion Syndrome:Do's & Dont's A Personal JourneyNo ratings yet
- Prof BSP-Akinetic Rigid Synd - PDDocument139 pagesProf BSP-Akinetic Rigid Synd - PDSavitha BasriNo ratings yet
- Sensory PolyneuropathiesDocument26 pagesSensory PolyneuropathiesAnderson TravassosNo ratings yet
- Conversion Disorder (2018)Document12 pagesConversion Disorder (2018)Maria Von ShaftNo ratings yet
- Allen 2017Document22 pagesAllen 2017Jere AyerbeNo ratings yet
- 2002, Vol.86, Issues 3, DementiaDocument219 pages2002, Vol.86, Issues 3, DementiaCesar GentilleNo ratings yet
- Neuroimaging Clinics - Imaging of Head TraumaDocument184 pagesNeuroimaging Clinics - Imaging of Head TraumaSimion Iulian100% (1)
- Fibromialgia - UptodateDocument21 pagesFibromialgia - UptodateaeadaNo ratings yet
- Sports Concussion and Neck Trauma: Preventing Injury for Future GenerationsFrom EverandSports Concussion and Neck Trauma: Preventing Injury for Future GenerationsNo ratings yet
- Emergency Clinical Diagnosis 2017Document292 pagesEmergency Clinical Diagnosis 2017Ouma KinéNo ratings yet
- Debilidad Muscular en UciDocument16 pagesDebilidad Muscular en UcipakokorreaNo ratings yet
- Head InjuryDocument31 pagesHead InjuryBoby SuryawanNo ratings yet
- Cranial NeuralgiasDocument14 pagesCranial NeuralgiasHabib G. Moutran BarrosoNo ratings yet
- Myasthenia Gravis: 1 Signs and SymptomsDocument9 pagesMyasthenia Gravis: 1 Signs and SymptomsBugMyNutsNo ratings yet
- Seizures in Childhood: John Bradford Ingram M.D. Assistant Professor of Pediatrics Division of Child NeurologyDocument50 pagesSeizures in Childhood: John Bradford Ingram M.D. Assistant Professor of Pediatrics Division of Child NeurologyTaylor ChristianNo ratings yet
- Neuroimaging in Acute StrokeDocument23 pagesNeuroimaging in Acute StrokeSnezana Mihajlovic100% (1)
- Jur DingDocument7 pagesJur DingRegina CaeciliaNo ratings yet
- Peripheral Nerve DisordersDocument65 pagesPeripheral Nerve DisordersAdhityaRizkyPratamaNo ratings yet
- Approach To Peripheral Neuropathy For Primary Care ClinicianDocument7 pagesApproach To Peripheral Neuropathy For Primary Care ClinicianGevania ArantzaNo ratings yet
- Cns TBC ImagingDocument54 pagesCns TBC ImaginginriantoNo ratings yet
- Guillian Barre SyndromeDocument11 pagesGuillian Barre SyndromemohamedNo ratings yet
- Inflamed Blood Vessels (Vasculitis), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Blood Vessels (Vasculitis), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Epilepsy - Definition, Classification, Pathophysiology, and EpidemiologyDocument7 pagesEpilepsy - Definition, Classification, Pathophysiology, and EpidemiologyMartín FleiNo ratings yet
- (What Do I Do Now - ) Sara C. LaHue, Morris Levin - Emergency Neurology (What Do I Do Now - ) - Oxford University Press (2021)Document241 pages(What Do I Do Now - ) Sara C. LaHue, Morris Levin - Emergency Neurology (What Do I Do Now - ) - Oxford University Press (2021)Andreea AtănăsoaeiNo ratings yet
- Evaluating MyopathyDocument17 pagesEvaluating MyopathyAbulSayeedDoulahNo ratings yet
- Neurology Update 2014Document56 pagesNeurology Update 2014lakshminivas PingaliNo ratings yet
- Guillain Barre SyndromeDocument6 pagesGuillain Barre SyndromeErtania NirmalaNo ratings yet
- Neuromyelitis Optica Spectrum Disorders.15Document33 pagesNeuromyelitis Optica Spectrum Disorders.15Marco Macavilca CruzNo ratings yet
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzNo ratings yet
- Status Epilepticus in Critically Ill PatientsDocument11 pagesStatus Epilepticus in Critically Ill PatientsAkbal Nur KarimNo ratings yet
- 2006, Vol.24, Issues 1, Brain Injury and Cardiac ArrestDocument169 pages2006, Vol.24, Issues 1, Brain Injury and Cardiac ArrestKishore Reddy BhavanamNo ratings yet
- The Second Edition Expert Consensus Statements On The Use of IVIg in NeurologyDocument134 pagesThe Second Edition Expert Consensus Statements On The Use of IVIg in NeurologyRonald DewaNo ratings yet
- Guillain BarreDocument20 pagesGuillain BarreRama JosuaNo ratings yet
- Pediatric Neurology Referral Guidelines: Table of ContentsDocument10 pagesPediatric Neurology Referral Guidelines: Table of ContentsEvannelson WardhanaNo ratings yet
- Epilepsy SleepDocument19 pagesEpilepsy SleepValois MartínezNo ratings yet
- Sleep TelemedicineDocument11 pagesSleep Telemedicinesavvy_as_98-1No ratings yet
- Brain Injury Rewiring for Loved Ones: A Lifeline to New ConnectionsFrom EverandBrain Injury Rewiring for Loved Ones: A Lifeline to New ConnectionsNo ratings yet
- Spontaneous Intracerebral Hemorrhage: Pathogenesis, Clinical Features, and DiagnosisDocument25 pagesSpontaneous Intracerebral Hemorrhage: Pathogenesis, Clinical Features, and DiagnosisBryan Tam ArevaloNo ratings yet
- G Barre ReviewDocument11 pagesG Barre ReviewLeyla Valdebenito AlidNo ratings yet
- Parkinson S Disease and Related Disorders Part II PDFDocument570 pagesParkinson S Disease and Related Disorders Part II PDFskyclad_21No ratings yet
- Dizziness - PPPD Information SheetDocument8 pagesDizziness - PPPD Information Sheettan_siqi100% (1)
- 02 Normal ''Suspicious'' EEGDocument10 pages02 Normal ''Suspicious'' EEGasNo ratings yet
- The Aetiologies of Epilepsy 2021Document16 pagesThe Aetiologies of Epilepsy 2021Ichrak GhachemNo ratings yet
- Carotid Artery Dissection PDFDocument3 pagesCarotid Artery Dissection PDFOdranoelRichamNo ratings yet
- 2023 - Pitfalls in Scalp EEG - Current Obstacles and Future Directions - SandorDocument21 pages2023 - Pitfalls in Scalp EEG - Current Obstacles and Future Directions - SandorJose Carlos Licea BlancoNo ratings yet
- C. Peter N. Watson, Anne A. Gershon, Michael N. Oxman (Eds.) - Herpes Zoster - Postherpetic Neuralgia and Other Complications - Focus On Treatment and Prevention (2017, ADIS) PDFDocument447 pagesC. Peter N. Watson, Anne A. Gershon, Michael N. Oxman (Eds.) - Herpes Zoster - Postherpetic Neuralgia and Other Complications - Focus On Treatment and Prevention (2017, ADIS) PDFJulianm8888No ratings yet
- 2008 - Neurofibromatoses - KaufmnanDocument203 pages2008 - Neurofibromatoses - KaufmnanPablo Antonio Antonio100% (1)
- Diagnosis Approach of Optic Neuritis 2155 9562 1000345Document13 pagesDiagnosis Approach of Optic Neuritis 2155 9562 1000345Juaan AvilaNo ratings yet
- ISO STANDARDS - Health Care TechnologyDocument9 pagesISO STANDARDS - Health Care TechnologyvesnaNo ratings yet
- Family Genogram in General MedicineDocument6 pagesFamily Genogram in General MedicineEsteban MatusNo ratings yet
- Descongestión en Lugar de Ultrafiltración CurrentOpinion, 2024Document8 pagesDescongestión en Lugar de Ultrafiltración CurrentOpinion, 2024LetyPerezTovarNo ratings yet
- Order 26634Document7 pagesOrder 26634Best EssaysNo ratings yet
- Chapter 9 - Endocrine GlandsDocument12 pagesChapter 9 - Endocrine GlandsICSE GURUNo ratings yet
- EyesDocument2 pagesEyesCzayanne Belle AdreceNo ratings yet
- The Protocols of Biomimetic Restorative Dentistry - 2002 To 2017 - June 2017 - Inside DentistryDocument7 pagesThe Protocols of Biomimetic Restorative Dentistry - 2002 To 2017 - June 2017 - Inside DentistryDaniel LoezaNo ratings yet
- OPHTHALMOLOGY Mind MapsDocument360 pagesOPHTHALMOLOGY Mind MapsHilda RenteriaNo ratings yet
- Sietins, Emils - CV (15062023)Document5 pagesSietins, Emils - CV (15062023)Emīls SietiņšNo ratings yet
- Multipel Vulnus IncisivumDocument11 pagesMultipel Vulnus IncisivumDeaz CressendoNo ratings yet
- AlcoholhistoryDocument14 pagesAlcoholhistoryapi-515964514No ratings yet
- LGBT Dalam IslamDocument35 pagesLGBT Dalam IslamJon FooNo ratings yet
- Health ProblemsDocument16 pagesHealth Problemschilindri1No ratings yet
- Conducting Vaginal Delivery Ym PDFDocument2 pagesConducting Vaginal Delivery Ym PDFyasodha maharajNo ratings yet
- Alpha Arbutin 2% + HA: About Usage DetailsDocument1 pageAlpha Arbutin 2% + HA: About Usage DetailsNahNo ratings yet
- Stress and Its Effect On Job SatisfactionDocument26 pagesStress and Its Effect On Job Satisfactionahmed zaheer50% (2)
- Cold Chain SpotterDocument16 pagesCold Chain SpotterPravin SurendranNo ratings yet
- Electrical InjuryDocument8 pagesElectrical InjuryFidya MayastriNo ratings yet
- According To GreenDocument2 pagesAccording To Greencate karanjaNo ratings yet
- Teaching Students With Autism Spectrum Disorder - Journal MalloryDocument36 pagesTeaching Students With Autism Spectrum Disorder - Journal Malloryapi-5215405080% (1)
- Ch.1+2 CMHNDocument48 pagesCh.1+2 CMHNMohammed Taysier QudaihNo ratings yet
- CLinical AbstractDocument5 pagesCLinical AbstractLovelyn BuenaflorNo ratings yet
- Research Project - Prostitution On StageDocument8 pagesResearch Project - Prostitution On StageKenyatta DeshazierNo ratings yet
- National Service Training ProgramDocument23 pagesNational Service Training ProgramAngelica EstacionNo ratings yet
- Classification and Coding of NeoplasmsDocument18 pagesClassification and Coding of NeoplasmsNajmul HasanNo ratings yet
- NHS FPX 6004 Assessment 3 Training Session For Policy ImplementationDocument7 pagesNHS FPX 6004 Assessment 3 Training Session For Policy ImplementationEmma WatsonNo ratings yet
- 7 Neutral ZoneDocument32 pages7 Neutral Zoneفاطمة الجش.No ratings yet
- Quiz MentalDocument31 pagesQuiz MentalEmma IntiaNo ratings yet
- Arterial Stiffness-1Document21 pagesArterial Stiffness-1yoeldp100% (2)