
Disaster Preparedness Attributes and Hospital's Resilience in Malaysia Disaster Preparedness Attributes and Hospital's Resilience in Malaysia
Disaster Preparedness Attributes and Hospital's Resilience in Malaysia Disaster Preparedness Attributes and Hospital's Resilience in Malaysia
You might also like
- Incorporating Resilience Into Business Continuity and Emergency Management For The Petroleum and Process IndustryDocument12 pagesIncorporating Resilience Into Business Continuity and Emergency Management For The Petroleum and Process IndustryypzoNo ratings yet
- Risk-Based Maintenance RBM A QuantitativDocument13 pagesRisk-Based Maintenance RBM A QuantitativandersonviNo ratings yet
- Designing A Questionnaire To Assess Crisis Management Based On A Resilience Engineering ApproachDocument12 pagesDesigning A Questionnaire To Assess Crisis Management Based On A Resilience Engineering ApproachMuhammad FaisalNo ratings yet
- Fallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFDocument11 pagesFallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFmalatebusNo ratings yet
- Health Care Workers and Disaster Preparedness BarrDocument9 pagesHealth Care Workers and Disaster Preparedness BarrIssam MotairekNo ratings yet
- Development and Testing of A Community Flood Resilience Measurement ToolDocument25 pagesDevelopment and Testing of A Community Flood Resilience Measurement ToolHamzaNo ratings yet
- Pish Namaz Zadeh 2020Document17 pagesPish Namaz Zadeh 2020haifariahi02No ratings yet
- اشعهDocument27 pagesاشعهe.budahabNo ratings yet
- Hospital Safety Index (HSI) Analysis in Confronting Disasters: A Case Study From IranDocument6 pagesHospital Safety Index (HSI) Analysis in Confronting Disasters: A Case Study From IranpertiwiNo ratings yet
- 3 PBDocument10 pages3 PBmetech8xNo ratings yet
- Emermed-2012-202282 Questionnaire 2Document10 pagesEmermed-2012-202282 Questionnaire 2Dr. Sahrish SabaNo ratings yet
- 155771Document29 pages155771Echa FaraNo ratings yet
- Assessing Levels of Hospital PreparednessDocument7 pagesAssessing Levels of Hospital PreparednessMaika YoingcoNo ratings yet
- Building Resilience Into Emergency ManagementDocument7 pagesBuilding Resilience Into Emergency ManagementYounes OULMANENo ratings yet
- 51 56, Tesma307, IJEASTDocument6 pages51 56, Tesma307, IJEASTaayush4995No ratings yet
- Hospital Disaster PlanDocument11 pagesHospital Disaster PlanMohammad Muntaz AliNo ratings yet
- Safety Risk Registers: Challenges and Guidance: Chemical EngineeringDocument6 pagesSafety Risk Registers: Challenges and Guidance: Chemical EngineeringBineeshNo ratings yet
- Research Article: Adaptive Failure Identification For Healthcare Risk Analysis and Its Application On E-HealthcareDocument18 pagesResearch Article: Adaptive Failure Identification For Healthcare Risk Analysis and Its Application On E-HealthcareAlejandro CardonaNo ratings yet
- Shuang Zhong Thesis PDFDocument251 pagesShuang Zhong Thesis PDFmalatebusNo ratings yet
- 1 s2.0 S1755599X1830034X MainDocument7 pages1 s2.0 S1755599X1830034X Mainhikmat pramajatiNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065Ica LarissaNo ratings yet
- Risk Management, Quality and SafetyDocument2 pagesRisk Management, Quality and Safetymanuela vilas boasNo ratings yet
- A Comprehensive Analysis of The Literature On The Impact of The Surgical Safety ChecklistDocument7 pagesA Comprehensive Analysis of The Literature On The Impact of The Surgical Safety ChecklistInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IHs Roles & Responsibilities in Emergency ManagementDocument17 pagesIHs Roles & Responsibilities in Emergency ManagementAnandababuNo ratings yet
- Disaster-Planning 2Document30 pagesDisaster-Planning 2Daryl Emmanuel ChuaNo ratings yet
- Residents Disaster Preparedness After The MeinongDocument12 pagesResidents Disaster Preparedness After The MeinongVerlina Intan WulandariNo ratings yet
- The Risk Management of Medical Device-Related Pressure Ulcers Based On The Australian/ New Zealand StandardDocument11 pagesThe Risk Management of Medical Device-Related Pressure Ulcers Based On The Australian/ New Zealand StandardJugurtha BoutlikhetNo ratings yet
- Asian Nursing ResearchDocument7 pagesAsian Nursing ResearchWayan Dyego SatyawanNo ratings yet
- Burgess Limerick 20229 ErgonomicsInterventionFinalReportJan2006Document93 pagesBurgess Limerick 20229 ErgonomicsInterventionFinalReportJan2006Eduardo JimenezNo ratings yet
- 1MSSH GuideNotes Assess-Mit-Planning 070110Document108 pages1MSSH GuideNotes Assess-Mit-Planning 070110npcdocNo ratings yet
- Development of A Hospital Medical Surge PreparednessDocument24 pagesDevelopment of A Hospital Medical Surge Preparednessbayu prabuNo ratings yet
- Bruneau Et Al 2003Document20 pagesBruneau Et Al 2003Taikhum VahanvatyNo ratings yet
- Disaster Management Managing The Calamities Through Operations ResearchDocument9 pagesDisaster Management Managing The Calamities Through Operations ResearchInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal Kesehatan Masyarakat: Hospital Fire Risk Analysis With Hazard, Vulnerability, Capacity, Risk Assessment ModelDocument6 pagesJurnal Kesehatan Masyarakat: Hospital Fire Risk Analysis With Hazard, Vulnerability, Capacity, Risk Assessment ModelhadianatyaNo ratings yet
- Art Art 2Document7 pagesArt Art 2Jhonny NogueraNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065Mircod SenseNo ratings yet
- The Importance of Disaster Management & Impact of Natural Disasters On HospitalsDocument13 pagesThe Importance of Disaster Management & Impact of Natural Disasters On HospitalssukhmanchawlaNo ratings yet
- Surge Capacity of Hospitals in EmergenciesDocument9 pagesSurge Capacity of Hospitals in Emergenciesbayu prabuNo ratings yet
- Community Disaster Resilience - A Systematic Review On Assessment Models and Tools - PLOS Currents Disasters PDFDocument18 pagesCommunity Disaster Resilience - A Systematic Review On Assessment Models and Tools - PLOS Currents Disasters PDFyrriuNo ratings yet
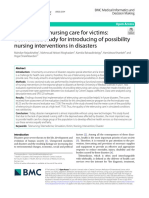
- Providing Telenursing Care For Victims: A Simulated Study For Introducing of Possibility Nursing Interventions in DisastersDocument9 pagesProviding Telenursing Care For Victims: A Simulated Study For Introducing of Possibility Nursing Interventions in DisastersDaadi Damiyar GeorginaNo ratings yet
- Skin Protection Seminars To Prevent Occupational Skin Diseas - 2018 - Safety andDocument10 pagesSkin Protection Seminars To Prevent Occupational Skin Diseas - 2018 - Safety andthalia mayoriNo ratings yet
- Operations Research in Disaster Preparedness and Response: The Public Health PerspectiveDocument21 pagesOperations Research in Disaster Preparedness and Response: The Public Health PerspectiveCap GarciaNo ratings yet
- Defining Safety Hazards & Risks in Mining Industry: A Case-Study in United StatesDocument9 pagesDefining Safety Hazards & Risks in Mining Industry: A Case-Study in United StatesJudith MungombeNo ratings yet
- Jurnal Peningkatan Keselamatan PasienDocument11 pagesJurnal Peningkatan Keselamatan Pasiensusi dwi fitriNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065gabigardasNo ratings yet
- Welcome To Our COVID Resource Page For EngineeringDocument5 pagesWelcome To Our COVID Resource Page For EngineeringfaniNo ratings yet
- 2564-Article Text-17430-2-10-20231124Document14 pages2564-Article Text-17430-2-10-20231124Rhey PrimeNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument10 pagesMedical Devices Inspection and Maintenance A Literature ReviewlchirinoscautinhoNo ratings yet
- Building Urban Resilience For Disaster RDocument8 pagesBuilding Urban Resilience For Disaster RDah IkbalNo ratings yet
- 10 1111@nin 12390Document14 pages10 1111@nin 12390YLA KATRINA BONILLANo ratings yet
- Journal 3Document7 pagesJournal 3Chytia NurhalizahNo ratings yet
- Entry Presentation GNpresentationDocument16 pagesEntry Presentation GNpresentationAarsol AdvanceNo ratings yet
- Penelitian TerdahuluDocument6 pagesPenelitian TerdahuluRia YuliartiNo ratings yet
- Disaster Cycle.Document14 pagesDisaster Cycle.jacob gNo ratings yet
- Jurnal PX Safety PDFDocument7 pagesJurnal PX Safety PDFChairunnisa Permata SariNo ratings yet
- The Sendai Framework For Disaster Risk Reduction: Renewing The Global Commitment To People's Resilience, Health, and Well-BeingDocument13 pagesThe Sendai Framework For Disaster Risk Reduction: Renewing The Global Commitment To People's Resilience, Health, and Well-BeingNATHANIEL YACASNo ratings yet
- Rapid Need Assessment JournalDocument16 pagesRapid Need Assessment Journalzubaidah muizNo ratings yet
- IntroductionDocument47 pagesIntroductionarpna sjsNo ratings yet
- Health System Resilience: A Literature Review of Empirical ResearchDocument26 pagesHealth System Resilience: A Literature Review of Empirical ResearchmalatebusNo ratings yet
- Resilient Health Care: A Systematic Review of Conceptualisations, Study Methods and Factors That Develop ResilienceDocument21 pagesResilient Health Care: A Systematic Review of Conceptualisations, Study Methods and Factors That Develop ResiliencemalatebusNo ratings yet
- What Makes Health Systems Resilient Against Infectious Disease Outbreaks and Natural Hazards? Results From A Scoping ReviewDocument9 pagesWhat Makes Health Systems Resilient Against Infectious Disease Outbreaks and Natural Hazards? Results From A Scoping ReviewmalatebusNo ratings yet
- Fallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFDocument11 pagesFallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFmalatebusNo ratings yet
- Steps Free PowerPoint TemplateDocument5 pagesSteps Free PowerPoint TemplatemalatebusNo ratings yet
- Shuang Zhong Thesis PDFDocument251 pagesShuang Zhong Thesis PDFmalatebusNo ratings yet
- Process Free PowerPoint TemplateDocument5 pagesProcess Free PowerPoint TemplatemalatebusNo ratings yet
- Movement FinanceDocument44 pagesMovement FinancemalatebusNo ratings yet
- Arham Visit ItineraryDocument1 pageArham Visit ItinerarymalatebusNo ratings yet
- BSC in Health CareDocument230 pagesBSC in Health CaremalatebusNo ratings yet
- Review of The Use of The Balanced Scorecard in Healthcare BMCDDocument38 pagesReview of The Use of The Balanced Scorecard in Healthcare BMCDmalatebusNo ratings yet
- Induction Folder HeirarchyDocument1 pageInduction Folder HeirarchymalatebusNo ratings yet
- IELSP Application Form Cohort 10Document18 pagesIELSP Application Form Cohort 10malatebusNo ratings yet
- Fema 253 PDFDocument402 pagesFema 253 PDFmbiancar100% (2)
- Chemical Terrorism DisasterDocument164 pagesChemical Terrorism DisasterAnshu ShahNo ratings yet
- Cep CBRN Response eDocument16 pagesCep CBRN Response enchimzaweNo ratings yet
- COMAH Guidance For The Surface Engineering Sector: Comah Major Accident Scenarios and Risk ReductionDocument15 pagesCOMAH Guidance For The Surface Engineering Sector: Comah Major Accident Scenarios and Risk ReductionHaroon RasheedNo ratings yet
- My Role During EmergencyDocument5 pagesMy Role During EmergencyPrem Shanker Rawat100% (1)
- Preparing Metro Manila Toward Urban Resiliency Prospects and RetrospectsDocument19 pagesPreparing Metro Manila Toward Urban Resiliency Prospects and RetrospectsWilvic Jan GacitaNo ratings yet
- NSTP-CWTS-Module 3 Disaster Awareness - Preparedness and ManagementEDitedDocument50 pagesNSTP-CWTS-Module 3 Disaster Awareness - Preparedness and ManagementEDitedPamie Penelope Bayoga100% (2)
- Isrs7 PSM Brochure Rev 7 - tcm155-273420Document12 pagesIsrs7 PSM Brochure Rev 7 - tcm155-273420Fani Purnama HasanNo ratings yet
- Mehedi Hasan Rimon: Education and TrainingDocument3 pagesMehedi Hasan Rimon: Education and TrainingMehedi Hasan RimonNo ratings yet
- Sample Bpops PlanDocument2 pagesSample Bpops PlanCasey Del Gallego EnrileNo ratings yet
- Instructions: Read The Passages Below. Together With Your Group, Identify The Risks Involved inDocument6 pagesInstructions: Read The Passages Below. Together With Your Group, Identify The Risks Involved inAdrian Kenneth Dequiña TandiamaNo ratings yet
- Briefer Operation ListoDocument2 pagesBriefer Operation ListoRosalie T. Orbon-TamondongNo ratings yet
- HSE Audit Checklist - Site BasedDocument19 pagesHSE Audit Checklist - Site BasedOws Anish100% (2)
- Roles and Responsibilities of DRRM TeamDocument13 pagesRoles and Responsibilities of DRRM TeamJohn Matthew CerenoNo ratings yet
- Covid 19 Impact On BahrainDocument5 pagesCovid 19 Impact On BahrainephraimNo ratings yet
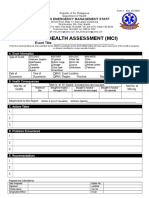
- Rapid Health Assessment (Mci) : Event TitleDocument2 pagesRapid Health Assessment (Mci) : Event TitleMrr ThoNo ratings yet
- Earthquake & MMEIRSDocument87 pagesEarthquake & MMEIRSPanzer MausNo ratings yet
- IVAN RISYANDI SANYOTO - DisastermanagementDocument5 pagesIVAN RISYANDI SANYOTO - DisastermanagementBocah PetualangNo ratings yet
- Chapter 2 Controls NewDocument46 pagesChapter 2 Controls NewNor Amirah RosliNo ratings yet
- ProposalDocument7 pagesProposalkarinaNo ratings yet
- The Role of The Security Sector in Covid 19 Response PagesDocument12 pagesThe Role of The Security Sector in Covid 19 Response PagesRaquel VallegaNo ratings yet
- Earthquake Drill PresentationDocument19 pagesEarthquake Drill Presentationjowindel mandabon100% (1)
- Republic Act 10121: Philippine Disaster Risk Reduction and Management Act of 2010Document3 pagesRepublic Act 10121: Philippine Disaster Risk Reduction and Management Act of 2010Celeste EstuyeNo ratings yet
- Comprehensive School Safety Monitoring ToolDocument8 pagesComprehensive School Safety Monitoring ToolRosella Lyka BoadillaNo ratings yet
- Chatham 911 ReportDocument13 pagesChatham 911 ReportAdam Van BrimmerNo ratings yet
- Contacts 6 25 2014Document130 pagesContacts 6 25 2014heru2910No ratings yet
- ISO 45001 Annex SL Reference SheetDocument2 pagesISO 45001 Annex SL Reference SheetyakinNo ratings yet
- Washer Compactor and Grit Classifier CleaningDocument18 pagesWasher Compactor and Grit Classifier CleaningKarthi Keyan R KNo ratings yet
- Food SafetyDocument50 pagesFood SafetyEvent Safety Management ServiceNo ratings yet
- Typhoon Haiyan: The Response So Far and Vital Lessons For RecoveryDocument18 pagesTyphoon Haiyan: The Response So Far and Vital Lessons For RecoveryOxfamNo ratings yet
































































































Download as pdf or txt
You might also like
- Incorporating Resilience Into Business Continuity and Emergency Management For The Petroleum and Process IndustryDocument12 pagesIncorporating Resilience Into Business Continuity and Emergency Management For The Petroleum and Process IndustryypzoNo ratings yet
- Risk-Based Maintenance RBM A QuantitativDocument13 pagesRisk-Based Maintenance RBM A QuantitativandersonviNo ratings yet
- Designing A Questionnaire To Assess Crisis Management Based On A Resilience Engineering ApproachDocument12 pagesDesigning A Questionnaire To Assess Crisis Management Based On A Resilience Engineering ApproachMuhammad FaisalNo ratings yet
- Fallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFDocument11 pagesFallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFmalatebusNo ratings yet
- Health Care Workers and Disaster Preparedness BarrDocument9 pagesHealth Care Workers and Disaster Preparedness BarrIssam MotairekNo ratings yet
- Development and Testing of A Community Flood Resilience Measurement ToolDocument25 pagesDevelopment and Testing of A Community Flood Resilience Measurement ToolHamzaNo ratings yet
- Pish Namaz Zadeh 2020Document17 pagesPish Namaz Zadeh 2020haifariahi02No ratings yet
- اشعهDocument27 pagesاشعهe.budahabNo ratings yet
- Hospital Safety Index (HSI) Analysis in Confronting Disasters: A Case Study From IranDocument6 pagesHospital Safety Index (HSI) Analysis in Confronting Disasters: A Case Study From IranpertiwiNo ratings yet
- 3 PBDocument10 pages3 PBmetech8xNo ratings yet
- Emermed-2012-202282 Questionnaire 2Document10 pagesEmermed-2012-202282 Questionnaire 2Dr. Sahrish SabaNo ratings yet
- 155771Document29 pages155771Echa FaraNo ratings yet
- Assessing Levels of Hospital PreparednessDocument7 pagesAssessing Levels of Hospital PreparednessMaika YoingcoNo ratings yet
- Building Resilience Into Emergency ManagementDocument7 pagesBuilding Resilience Into Emergency ManagementYounes OULMANENo ratings yet
- 51 56, Tesma307, IJEASTDocument6 pages51 56, Tesma307, IJEASTaayush4995No ratings yet
- Hospital Disaster PlanDocument11 pagesHospital Disaster PlanMohammad Muntaz AliNo ratings yet
- Safety Risk Registers: Challenges and Guidance: Chemical EngineeringDocument6 pagesSafety Risk Registers: Challenges and Guidance: Chemical EngineeringBineeshNo ratings yet
- Research Article: Adaptive Failure Identification For Healthcare Risk Analysis and Its Application On E-HealthcareDocument18 pagesResearch Article: Adaptive Failure Identification For Healthcare Risk Analysis and Its Application On E-HealthcareAlejandro CardonaNo ratings yet
- Shuang Zhong Thesis PDFDocument251 pagesShuang Zhong Thesis PDFmalatebusNo ratings yet
- 1 s2.0 S1755599X1830034X MainDocument7 pages1 s2.0 S1755599X1830034X Mainhikmat pramajatiNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065Ica LarissaNo ratings yet
- Risk Management, Quality and SafetyDocument2 pagesRisk Management, Quality and Safetymanuela vilas boasNo ratings yet
- A Comprehensive Analysis of The Literature On The Impact of The Surgical Safety ChecklistDocument7 pagesA Comprehensive Analysis of The Literature On The Impact of The Surgical Safety ChecklistInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IHs Roles & Responsibilities in Emergency ManagementDocument17 pagesIHs Roles & Responsibilities in Emergency ManagementAnandababuNo ratings yet
- Disaster-Planning 2Document30 pagesDisaster-Planning 2Daryl Emmanuel ChuaNo ratings yet
- Residents Disaster Preparedness After The MeinongDocument12 pagesResidents Disaster Preparedness After The MeinongVerlina Intan WulandariNo ratings yet
- The Risk Management of Medical Device-Related Pressure Ulcers Based On The Australian/ New Zealand StandardDocument11 pagesThe Risk Management of Medical Device-Related Pressure Ulcers Based On The Australian/ New Zealand StandardJugurtha BoutlikhetNo ratings yet
- Asian Nursing ResearchDocument7 pagesAsian Nursing ResearchWayan Dyego SatyawanNo ratings yet
- Burgess Limerick 20229 ErgonomicsInterventionFinalReportJan2006Document93 pagesBurgess Limerick 20229 ErgonomicsInterventionFinalReportJan2006Eduardo JimenezNo ratings yet
- 1MSSH GuideNotes Assess-Mit-Planning 070110Document108 pages1MSSH GuideNotes Assess-Mit-Planning 070110npcdocNo ratings yet
- Development of A Hospital Medical Surge PreparednessDocument24 pagesDevelopment of A Hospital Medical Surge Preparednessbayu prabuNo ratings yet
- Bruneau Et Al 2003Document20 pagesBruneau Et Al 2003Taikhum VahanvatyNo ratings yet
- Disaster Management Managing The Calamities Through Operations ResearchDocument9 pagesDisaster Management Managing The Calamities Through Operations ResearchInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal Kesehatan Masyarakat: Hospital Fire Risk Analysis With Hazard, Vulnerability, Capacity, Risk Assessment ModelDocument6 pagesJurnal Kesehatan Masyarakat: Hospital Fire Risk Analysis With Hazard, Vulnerability, Capacity, Risk Assessment ModelhadianatyaNo ratings yet
- Art Art 2Document7 pagesArt Art 2Jhonny NogueraNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065Mircod SenseNo ratings yet
- The Importance of Disaster Management & Impact of Natural Disasters On HospitalsDocument13 pagesThe Importance of Disaster Management & Impact of Natural Disasters On HospitalssukhmanchawlaNo ratings yet
- Surge Capacity of Hospitals in EmergenciesDocument9 pagesSurge Capacity of Hospitals in Emergenciesbayu prabuNo ratings yet
- Community Disaster Resilience - A Systematic Review On Assessment Models and Tools - PLOS Currents Disasters PDFDocument18 pagesCommunity Disaster Resilience - A Systematic Review On Assessment Models and Tools - PLOS Currents Disasters PDFyrriuNo ratings yet
- Providing Telenursing Care For Victims: A Simulated Study For Introducing of Possibility Nursing Interventions in DisastersDocument9 pagesProviding Telenursing Care For Victims: A Simulated Study For Introducing of Possibility Nursing Interventions in DisastersDaadi Damiyar GeorginaNo ratings yet
- Skin Protection Seminars To Prevent Occupational Skin Diseas - 2018 - Safety andDocument10 pagesSkin Protection Seminars To Prevent Occupational Skin Diseas - 2018 - Safety andthalia mayoriNo ratings yet
- Operations Research in Disaster Preparedness and Response: The Public Health PerspectiveDocument21 pagesOperations Research in Disaster Preparedness and Response: The Public Health PerspectiveCap GarciaNo ratings yet
- Defining Safety Hazards & Risks in Mining Industry: A Case-Study in United StatesDocument9 pagesDefining Safety Hazards & Risks in Mining Industry: A Case-Study in United StatesJudith MungombeNo ratings yet
- Jurnal Peningkatan Keselamatan PasienDocument11 pagesJurnal Peningkatan Keselamatan Pasiensusi dwi fitriNo ratings yet
- Iso 14971 8-B2017065Document6 pagesIso 14971 8-B2017065gabigardasNo ratings yet
- Welcome To Our COVID Resource Page For EngineeringDocument5 pagesWelcome To Our COVID Resource Page For EngineeringfaniNo ratings yet
- 2564-Article Text-17430-2-10-20231124Document14 pages2564-Article Text-17430-2-10-20231124Rhey PrimeNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument10 pagesMedical Devices Inspection and Maintenance A Literature ReviewlchirinoscautinhoNo ratings yet
- Building Urban Resilience For Disaster RDocument8 pagesBuilding Urban Resilience For Disaster RDah IkbalNo ratings yet
- 10 1111@nin 12390Document14 pages10 1111@nin 12390YLA KATRINA BONILLANo ratings yet
- Journal 3Document7 pagesJournal 3Chytia NurhalizahNo ratings yet
- Entry Presentation GNpresentationDocument16 pagesEntry Presentation GNpresentationAarsol AdvanceNo ratings yet
- Penelitian TerdahuluDocument6 pagesPenelitian TerdahuluRia YuliartiNo ratings yet
- Disaster Cycle.Document14 pagesDisaster Cycle.jacob gNo ratings yet
- Jurnal PX Safety PDFDocument7 pagesJurnal PX Safety PDFChairunnisa Permata SariNo ratings yet
- The Sendai Framework For Disaster Risk Reduction: Renewing The Global Commitment To People's Resilience, Health, and Well-BeingDocument13 pagesThe Sendai Framework For Disaster Risk Reduction: Renewing The Global Commitment To People's Resilience, Health, and Well-BeingNATHANIEL YACASNo ratings yet
- Rapid Need Assessment JournalDocument16 pagesRapid Need Assessment Journalzubaidah muizNo ratings yet
- IntroductionDocument47 pagesIntroductionarpna sjsNo ratings yet
- Health System Resilience: A Literature Review of Empirical ResearchDocument26 pagesHealth System Resilience: A Literature Review of Empirical ResearchmalatebusNo ratings yet
- Resilient Health Care: A Systematic Review of Conceptualisations, Study Methods and Factors That Develop ResilienceDocument21 pagesResilient Health Care: A Systematic Review of Conceptualisations, Study Methods and Factors That Develop ResiliencemalatebusNo ratings yet
- What Makes Health Systems Resilient Against Infectious Disease Outbreaks and Natural Hazards? Results From A Scoping ReviewDocument9 pagesWhat Makes Health Systems Resilient Against Infectious Disease Outbreaks and Natural Hazards? Results From A Scoping ReviewmalatebusNo ratings yet
- Fallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFDocument11 pagesFallah-Aliabadi2020 Article TowardsDevelopingAModelForTheE PDFmalatebusNo ratings yet
- Steps Free PowerPoint TemplateDocument5 pagesSteps Free PowerPoint TemplatemalatebusNo ratings yet
- Shuang Zhong Thesis PDFDocument251 pagesShuang Zhong Thesis PDFmalatebusNo ratings yet
- Process Free PowerPoint TemplateDocument5 pagesProcess Free PowerPoint TemplatemalatebusNo ratings yet
- Movement FinanceDocument44 pagesMovement FinancemalatebusNo ratings yet
- Arham Visit ItineraryDocument1 pageArham Visit ItinerarymalatebusNo ratings yet
- BSC in Health CareDocument230 pagesBSC in Health CaremalatebusNo ratings yet
- Review of The Use of The Balanced Scorecard in Healthcare BMCDDocument38 pagesReview of The Use of The Balanced Scorecard in Healthcare BMCDmalatebusNo ratings yet
- Induction Folder HeirarchyDocument1 pageInduction Folder HeirarchymalatebusNo ratings yet
- IELSP Application Form Cohort 10Document18 pagesIELSP Application Form Cohort 10malatebusNo ratings yet
- Fema 253 PDFDocument402 pagesFema 253 PDFmbiancar100% (2)
- Chemical Terrorism DisasterDocument164 pagesChemical Terrorism DisasterAnshu ShahNo ratings yet
- Cep CBRN Response eDocument16 pagesCep CBRN Response enchimzaweNo ratings yet
- COMAH Guidance For The Surface Engineering Sector: Comah Major Accident Scenarios and Risk ReductionDocument15 pagesCOMAH Guidance For The Surface Engineering Sector: Comah Major Accident Scenarios and Risk ReductionHaroon RasheedNo ratings yet
- My Role During EmergencyDocument5 pagesMy Role During EmergencyPrem Shanker Rawat100% (1)
- Preparing Metro Manila Toward Urban Resiliency Prospects and RetrospectsDocument19 pagesPreparing Metro Manila Toward Urban Resiliency Prospects and RetrospectsWilvic Jan GacitaNo ratings yet
- NSTP-CWTS-Module 3 Disaster Awareness - Preparedness and ManagementEDitedDocument50 pagesNSTP-CWTS-Module 3 Disaster Awareness - Preparedness and ManagementEDitedPamie Penelope Bayoga100% (2)
- Isrs7 PSM Brochure Rev 7 - tcm155-273420Document12 pagesIsrs7 PSM Brochure Rev 7 - tcm155-273420Fani Purnama HasanNo ratings yet
- Mehedi Hasan Rimon: Education and TrainingDocument3 pagesMehedi Hasan Rimon: Education and TrainingMehedi Hasan RimonNo ratings yet
- Sample Bpops PlanDocument2 pagesSample Bpops PlanCasey Del Gallego EnrileNo ratings yet
- Instructions: Read The Passages Below. Together With Your Group, Identify The Risks Involved inDocument6 pagesInstructions: Read The Passages Below. Together With Your Group, Identify The Risks Involved inAdrian Kenneth Dequiña TandiamaNo ratings yet
- Briefer Operation ListoDocument2 pagesBriefer Operation ListoRosalie T. Orbon-TamondongNo ratings yet
- HSE Audit Checklist - Site BasedDocument19 pagesHSE Audit Checklist - Site BasedOws Anish100% (2)
- Roles and Responsibilities of DRRM TeamDocument13 pagesRoles and Responsibilities of DRRM TeamJohn Matthew CerenoNo ratings yet
- Covid 19 Impact On BahrainDocument5 pagesCovid 19 Impact On BahrainephraimNo ratings yet
- Rapid Health Assessment (Mci) : Event TitleDocument2 pagesRapid Health Assessment (Mci) : Event TitleMrr ThoNo ratings yet
- Earthquake & MMEIRSDocument87 pagesEarthquake & MMEIRSPanzer MausNo ratings yet
- IVAN RISYANDI SANYOTO - DisastermanagementDocument5 pagesIVAN RISYANDI SANYOTO - DisastermanagementBocah PetualangNo ratings yet
- Chapter 2 Controls NewDocument46 pagesChapter 2 Controls NewNor Amirah RosliNo ratings yet
- ProposalDocument7 pagesProposalkarinaNo ratings yet
- The Role of The Security Sector in Covid 19 Response PagesDocument12 pagesThe Role of The Security Sector in Covid 19 Response PagesRaquel VallegaNo ratings yet
- Earthquake Drill PresentationDocument19 pagesEarthquake Drill Presentationjowindel mandabon100% (1)
- Republic Act 10121: Philippine Disaster Risk Reduction and Management Act of 2010Document3 pagesRepublic Act 10121: Philippine Disaster Risk Reduction and Management Act of 2010Celeste EstuyeNo ratings yet
- Comprehensive School Safety Monitoring ToolDocument8 pagesComprehensive School Safety Monitoring ToolRosella Lyka BoadillaNo ratings yet
- Chatham 911 ReportDocument13 pagesChatham 911 ReportAdam Van BrimmerNo ratings yet
- Contacts 6 25 2014Document130 pagesContacts 6 25 2014heru2910No ratings yet
- ISO 45001 Annex SL Reference SheetDocument2 pagesISO 45001 Annex SL Reference SheetyakinNo ratings yet
- Washer Compactor and Grit Classifier CleaningDocument18 pagesWasher Compactor and Grit Classifier CleaningKarthi Keyan R KNo ratings yet
- Food SafetyDocument50 pagesFood SafetyEvent Safety Management ServiceNo ratings yet
- Typhoon Haiyan: The Response So Far and Vital Lessons For RecoveryDocument18 pagesTyphoon Haiyan: The Response So Far and Vital Lessons For RecoveryOxfamNo ratings yet