Download as doc, pdf, or txt
You might also like
- Upto 145kV 40ka 3150A Operating ManualDocument64 pagesUpto 145kV 40ka 3150A Operating Manuala234588% (17)
- ELM-210-D-T2-Aligning Standards and Learning Objectives - Sesalie - NelsonDocument3 pagesELM-210-D-T2-Aligning Standards and Learning Objectives - Sesalie - NelsonSesalie Nelson0% (1)
- CCDM Manual PDFDocument715 pagesCCDM Manual PDFrehanaNo ratings yet
- SITHKOP004 Assessment 2 Project - Docx Resources 4 MayDocument35 pagesSITHKOP004 Assessment 2 Project - Docx Resources 4 MayAditya SharmaNo ratings yet
- Doi: 10.7243/2054-9865-2-2 WHO Modified Partograph: Name (Last, First) Parity/Gravida Date LMP EDD Age Gestation (WKS)Document1 pageDoi: 10.7243/2054-9865-2-2 WHO Modified Partograph: Name (Last, First) Parity/Gravida Date LMP EDD Age Gestation (WKS)Danielle Faye ClerigoNo ratings yet
- 5 - Southern Cross - Iso Pump - 65 X 50 - 160 - 1410-2890 RPMDocument1 page5 - Southern Cross - Iso Pump - 65 X 50 - 160 - 1410-2890 RPMBryan ChaiNo ratings yet
- Bedfordview Take Away Menu March 2024Document2 pagesBedfordview Take Away Menu March 2024Francois SlabbertNo ratings yet
- Searchlight Sonar: ModelDocument4 pagesSearchlight Sonar: Modelsyarifahdwi92No ratings yet
- PAI Engine BrochureDocument20 pagesPAI Engine BrochureUmair MalikNo ratings yet
- Kiara Sinha - 2011-07-06Document1 pageKiara Sinha - 2011-07-06Sweta SinhaNo ratings yet
- Aarohi Sinha - 2011-07-06Document1 pageAarohi Sinha - 2011-07-06Sweta SinhaNo ratings yet
- 1 - Southern Cross - Iso Pump - 50 X 32 - 160 - 1410-2880 RPM PDFDocument1 page1 - Southern Cross - Iso Pump - 50 X 32 - 160 - 1410-2880 RPM PDFIra LtrNo ratings yet
- FL Brochure CompressedDocument4 pagesFL Brochure CompressedSoorya GNo ratings yet
- HMBCDocument1 pageHMBCAchmad WildanNo ratings yet
- Results and DiscussionDocument38 pagesResults and DiscussionKarlo TimbalNo ratings yet
- PrabhaDocument1 pagePrabhaRehanaNo ratings yet
- HistogramDocument1 pageHistogramErica SandersNo ratings yet
- Door ListDocument2 pagesDoor ListlentiNo ratings yet
- Tauane Raizila Ferreira Dos Santos-Tauane Raizila Ferreira Dos Santos MandDocument5 pagesTauane Raizila Ferreira Dos Santos-Tauane Raizila Ferreira Dos Santos Mandtauaneraizila15No ratings yet
- Textbook Comparative Bone Identification Human Subadult To Nonhuman 1St Edition France Ebook All Chapter PDFDocument53 pagesTextbook Comparative Bone Identification Human Subadult To Nonhuman 1St Edition France Ebook All Chapter PDFjames.pinkerton561100% (13)
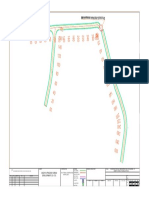
- Basaoda TBD Plan LayoutDocument1 pageBasaoda TBD Plan LayoutANKESH SHRIVASTAVANo ratings yet
- Psychrometric Chart BasicsDocument57 pagesPsychrometric Chart BasicsMuhibullah MuhibNo ratings yet
- Pedoman Early Warning System: Revisi 1Document7 pagesPedoman Early Warning System: Revisi 1Jihan ShelvyNo ratings yet
- Who Growth Charts FullDocument30 pagesWho Growth Charts Fullyohannes feteneNo ratings yet
- Solidc - Curvas PerformaceDocument8 pagesSolidc - Curvas Performacedouglas alvesNo ratings yet
- Sandwich Plate Aluminium PlateDocument3 pagesSandwich Plate Aluminium Plateyaswanth179No ratings yet
- Fisher ET-EAT-ETR PBDocument28 pagesFisher ET-EAT-ETR PBIrwin CastroNo ratings yet
- Aries Agro - Hdcsec 2014Document19 pagesAries Agro - Hdcsec 2014jigarchhatrolaNo ratings yet
- Dr. Zaenal Mutaqien (Promotive and Sport Medicine)Document27 pagesDr. Zaenal Mutaqien (Promotive and Sport Medicine)Red DemonNo ratings yet
- CHT Hfa Boys Z 5 19yearsDocument1 pageCHT Hfa Boys Z 5 19yearsRhea JavierNo ratings yet
- CHT Hfa Boys Z 5 19years PDFDocument1 pageCHT Hfa Boys Z 5 19years PDFchipta lestariNo ratings yet
- Who Height-For-Age Boys 5 19yearsDocument1 pageWho Height-For-Age Boys 5 19yearsAulia Rahman NasrunNo ratings yet
- Height-For-Age BOYS: 5 To 19 Years (Z-Scores)Document1 pageHeight-For-Age BOYS: 5 To 19 Years (Z-Scores)chipta lestari100% (1)
- Who Height-For-Age Boys 5 19years PDFDocument1 pageWho Height-For-Age Boys 5 19years PDFAulia Rahman NasrunNo ratings yet
- OMS. Altura para Idade Meninos - 5-19 Anos. em Z Score.Document1 pageOMS. Altura para Idade Meninos - 5-19 Anos. em Z Score.Lucas Alves SalesNo ratings yet
- Height-For-Age BOYS: 5 To 19 Years (Z-Scores)Document1 pageHeight-For-Age BOYS: 5 To 19 Years (Z-Scores)A YNo ratings yet
- v2 Pews Form 12 23 Months National 0 3Document2 pagesv2 Pews Form 12 23 Months National 0 3SriwulandariNo ratings yet
- Antennas and Cables: Zywall VPN FirewallDocument8 pagesAntennas and Cables: Zywall VPN FirewallCuong TranNo ratings yet
- TacometrosDocument1 pageTacometrosAriel AldanaNo ratings yet
- STEEL-Model - PDF 2Document1 pageSTEEL-Model - PDF 2Ahmed MohamedNo ratings yet
- Fundamental Stock Market IndicatorDocument6 pagesFundamental Stock Market IndicatorbulbtommyNo ratings yet
- Ugarte Maria. Max. SupDocument1 pageUgarte Maria. Max. SupEnzoMNo ratings yet
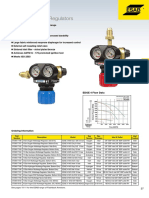
- Regulators Edge 4 Series RegulatorsDocument1 pageRegulators Edge 4 Series RegulatorsDries VandezandeNo ratings yet
- A Graphical Representation of Inverse VRML Uptake: FSW Air EAN X 32% Eanx 36%Document1 pageA Graphical Representation of Inverse VRML Uptake: FSW Air EAN X 32% Eanx 36%pmech consultantNo ratings yet
- National Directorate For Fire and Emergency Management: Eeping Ommunities AfeDocument121 pagesNational Directorate For Fire and Emergency Management: Eeping Ommunities Afenathaniscool67325729No ratings yet
- Pompa Icar EcofilDocument2 pagesPompa Icar EcofilTito SaranaNo ratings yet
- Garden Part of Cave RestaurantDocument29 pagesGarden Part of Cave RestaurantMarjan FaberNo ratings yet
- Psychrometric Chart BasicsDocument64 pagesPsychrometric Chart BasicsAditya Untung NugrohoNo ratings yet
- PsychrometricChartBasics LectureDocument54 pagesPsychrometricChartBasics Lecturemeen19111087 KFUEITNo ratings yet
- Psychrometric Chart BasicsDocument64 pagesPsychrometric Chart BasicsHemantSharmaNo ratings yet
- Variogram Tutorial: Randal Barnes Golden Software, IncDocument23 pagesVariogram Tutorial: Randal Barnes Golden Software, IncOusmane NdourNo ratings yet
- ESAB ExtractPage25-26cDocument8 pagesESAB ExtractPage25-26cDries VandezandeNo ratings yet
- Tauane Raizila Ferreira Dos Santos-Tauane Raizila Ferreira Dos Santos MX 3Document5 pagesTauane Raizila Ferreira Dos Santos-Tauane Raizila Ferreira Dos Santos MX 3tauaneraizila15No ratings yet
- 2 To 20 Years: Boys Cerebral Palsy GMFCS V, Feeds Orally Weight For Age PercentilesDocument3 pages2 To 20 Years: Boys Cerebral Palsy GMFCS V, Feeds Orally Weight For Age PercentilesJohanna RobayoNo ratings yet
- Microeconomics Production TheoryDocument29 pagesMicroeconomics Production Theorysagar dhakalNo ratings yet
- B5NT PDFDocument3 pagesB5NT PDFDewi PrasetiaNo ratings yet
- PDF - PdpiefDocument4 pagesPDF - Pdpiefhowa howaNo ratings yet
- G5TFDocument3 pagesG5TFDiana LaraNo ratings yet
- RullgrapDocument1 pageRullgrapcetak nasriNo ratings yet
- QUESTIONDocument2 pagesQUESTIONdanielNo ratings yet
- Alice ProposalDocument6 pagesAlice ProposaldanielNo ratings yet
- HCF 203 AssignmentDocument4 pagesHCF 203 AssignmentdanielNo ratings yet
- Mupukuta IndexDocument7 pagesMupukuta IndexdanielNo ratings yet
- Godfrey Moffat: Number 11 Brentwood RD MT Pleasant HarareDocument1 pageGodfrey Moffat: Number 11 Brentwood RD MT Pleasant HararedanielNo ratings yet
- MNLDocument1 pageMNLdanielNo ratings yet
- MupukutaDocument4 pagesMupukutadanielNo ratings yet
- Hiph ApplicationsDocument1 pageHiph ApplicationsdanielNo ratings yet
- Muzdok: Dear (Recipient Name)Document1 pageMuzdok: Dear (Recipient Name)danielNo ratings yet
- 29.HIV in GynaecologyDocument20 pages29.HIV in GynaecologydanielNo ratings yet
- Antepartum HaemorrhageDocument13 pagesAntepartum HaemorrhagedanielNo ratings yet
- Gracious ChagondaDocument1 pageGracious ChagondadanielNo ratings yet
- CV For Valentine KajawuDocument8 pagesCV For Valentine KajawudanielNo ratings yet
- Prof J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabweDocument17 pagesProf J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabwedanielNo ratings yet
- Ultrasound ScanDocument11 pagesUltrasound ScandanielNo ratings yet
- Lower Genital Tract InfectionDocument3 pagesLower Genital Tract InfectiondanielNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Utero-Vaginal ProlapseDocument8 pagesUtero-Vaginal ProlapsedanielNo ratings yet
- Instruments and X RayDocument30 pagesInstruments and X RaydanielNo ratings yet
- Upper Genital Tract InfectionDocument2 pagesUpper Genital Tract InfectiondanielNo ratings yet
- Vaginal Prolapse: by DR MutevheDocument32 pagesVaginal Prolapse: by DR MutevhedanielNo ratings yet
- Vesicovaginal FistulaDocument54 pagesVesicovaginal FistuladanielNo ratings yet
- Management of Amenorrhoea: 1999 Obstetrics & Gynaecology by Duy ThaiDocument2 pagesManagement of Amenorrhoea: 1999 Obstetrics & Gynaecology by Duy ThaidanielNo ratings yet
- Miscarriages and Ectopic PregnanciesDocument4 pagesMiscarriages and Ectopic PregnanciesdanielNo ratings yet
- 2-Anatomy of The PelvisDocument29 pages2-Anatomy of The PelvisdanielNo ratings yet
- Estimate Electrical Guwahati UniversityDocument19 pagesEstimate Electrical Guwahati UniversityTandon Abhilash BorthakurNo ratings yet
- 11 English Mixed Test Paper 02Document4 pages11 English Mixed Test Paper 02Robin AhujaNo ratings yet
- Tipi InstructionsDocument32 pagesTipi InstructionsZenrof100% (1)
- Piyush Kumar RaiDocument6 pagesPiyush Kumar RaiAyisha PatnaikNo ratings yet
- SITXHRM009 Assessment 1 - Short AnswersDocument13 pagesSITXHRM009 Assessment 1 - Short AnswerssolucionesredesecNo ratings yet
- Ions & Ionic Bonds (Multiple Choice) QPDocument7 pagesIons & Ionic Bonds (Multiple Choice) QPBăng Băng LêNo ratings yet
- About EEIP: Interview With Dusan JakovljevicDocument2 pagesAbout EEIP: Interview With Dusan JakovljevicEnergy Efficiency in Industrial Processes (EEIP)No ratings yet
- Adeshwar Nursing Institute Khamhargaon, Jagdalpur: Community Health Nursing Lesson Plan ON Wound DressingDocument8 pagesAdeshwar Nursing Institute Khamhargaon, Jagdalpur: Community Health Nursing Lesson Plan ON Wound DressingNitesh BhuraNo ratings yet
- Ind Pharm 5th SemDocument12 pagesInd Pharm 5th Semsuyash jainNo ratings yet
- Jan W. Gooch, Biosketch - Jan. 2015Document15 pagesJan W. Gooch, Biosketch - Jan. 2015jan w goochNo ratings yet
- Reassembly: 1. Assemble Piston and Connecting RodDocument7 pagesReassembly: 1. Assemble Piston and Connecting Roddawitmesfin9No ratings yet
- Joy Hermalyn CV 2020Document5 pagesJoy Hermalyn CV 2020api-518378178No ratings yet
- Action Research Proposal Tandas EstimaDocument11 pagesAction Research Proposal Tandas EstimaHilaria EstimaNo ratings yet
- KIP7770 KService ManualDocument659 pagesKIP7770 KService Manualjoe100% (1)
- Placa Mãe HD7Document3 pagesPlaca Mãe HD7ALBANO2No ratings yet
- TRANSMISSION LINE COMMISSIONING Publication - No.292 PDFDocument46 pagesTRANSMISSION LINE COMMISSIONING Publication - No.292 PDFmohit mudgal100% (6)
- Antecedentes 2Document26 pagesAntecedentes 2Carlos Mario Ortiz MuñozNo ratings yet
- Scaling BenchmarkDocument7 pagesScaling BenchmarkJuan Pablo Henríquez ValenciaNo ratings yet
- Transforming Small Local Business To Widely Recognized BrandsDocument6 pagesTransforming Small Local Business To Widely Recognized BrandsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- E School Management SystemDocument36 pagesE School Management SystemShivangi Priya VlogsNo ratings yet
- History of MeditationDocument4 pagesHistory of MeditationChinmay KumtakarNo ratings yet
- EBS Period Close Analyzer-CompressedDocument29 pagesEBS Period Close Analyzer-CompressedRaoof AhmedNo ratings yet
- Who Invented The Periodic TableDocument1 pageWho Invented The Periodic TableJny An AparenteNo ratings yet
- Office of The RegistrarDocument3 pagesOffice of The RegistrarAdemolaNo ratings yet
- List Rickt Divx (01 - 09 10)Document22 pagesList Rickt Divx (01 - 09 10)Mila MulianiNo ratings yet