Download as pdf or txt
You might also like
- Wafa Obgyn Smle2021Document146 pagesWafa Obgyn Smle2021Amal100% (1)
- Reviewer - Immunoserology - Part 1Document12 pagesReviewer - Immunoserology - Part 1Joshua Trinidad0% (1)
- MUST To KNOW in Clinical ChemistryDocument53 pagesMUST To KNOW in Clinical ChemistryMonkey LuffyNo ratings yet
- Reviewer - Immunohematology - Part 1Document16 pagesReviewer - Immunohematology - Part 1Joshua TrinidadNo ratings yet
- Cc1-Task 4Document8 pagesCc1-Task 4Joshua TrinidadNo ratings yet
- Cc1-Task 3Document3 pagesCc1-Task 3Joshua Trinidad100% (1)
- Reviewer - Immunohematology - Part 1Document16 pagesReviewer - Immunohematology - Part 1Joshua TrinidadNo ratings yet
- Active Cycle Breathing TechniqueDocument20 pagesActive Cycle Breathing TechniqueRAM100% (2)
- LJMDocument15 pagesLJMDark Nurse100% (6)
- Must To Know HemaDocument44 pagesMust To Know HemaKaycee Gretz LorescaNo ratings yet
- Serologic Tests Part 1Document4 pagesSerologic Tests Part 1Joshua TrinidadNo ratings yet
- Other Blood Group System AssignmentDocument5 pagesOther Blood Group System AssignmentMary ChristelleNo ratings yet
- CSMLS Exam Guide Notes (Referrence Range)Document4 pagesCSMLS Exam Guide Notes (Referrence Range)software4us.2023No ratings yet
- Disorders of Iron Kinetics and Heme MetabolismDocument12 pagesDisorders of Iron Kinetics and Heme MetabolismJoanne JardinNo ratings yet
- ISBB Aaaaa PDFDocument55 pagesISBB Aaaaa PDFSelena de LimaNo ratings yet
- Microscopic Examination of UrineDocument4 pagesMicroscopic Examination of UrineGlaiza Erika Baes GudaNo ratings yet
- CLINICAL CHEMISTRY - Specimen CollectionDocument4 pagesCLINICAL CHEMISTRY - Specimen CollectionthedarkwingNo ratings yet
- Clinical ChemistryDocument7 pagesClinical ChemistryDale SuanoNo ratings yet
- Clinical Chemistry Board ReviewDocument14 pagesClinical Chemistry Board ReviewWellaBaylasNo ratings yet
- C1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDocument8 pagesC1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDIVINA KYLE YGO100% (1)
- Hema Notes (Lec)Document50 pagesHema Notes (Lec)Anonymous 0zrCNQNo ratings yet
- SerologyDocument84 pagesSerologyngsusannasuisum100% (2)
- Histopathology Review BookletDocument21 pagesHistopathology Review BookletMarie Llanes100% (2)
- Serological TestsDocument2 pagesSerological TestsKimberly EspaldonNo ratings yet
- Chapter 1: Introduction To Urinalysis: Urine CompositionDocument74 pagesChapter 1: Introduction To Urinalysis: Urine CompositionMegumi TadokoroNo ratings yet
- ENZYMOLOGYDocument2 pagesENZYMOLOGYCarla Lagar FloresNo ratings yet
- White Cell and Platelet MorphologyDocument7 pagesWhite Cell and Platelet Morphologylamjo5750% (1)
- Pre and Post Analytical Procedures: Subtopic: Receiving, Accessioning, & Releasing of ResultsDocument29 pagesPre and Post Analytical Procedures: Subtopic: Receiving, Accessioning, & Releasing of ResultsShara AboNo ratings yet
- Compre HistopatDocument21 pagesCompre HistopatMark FuerteNo ratings yet
- HistopathDocument23 pagesHistopathElla SalesNo ratings yet
- MUST To KNOW in BacteriologyDocument35 pagesMUST To KNOW in BacteriologyJohn TamayoNo ratings yet
- Board Exam Topic ChecklistDocument3 pagesBoard Exam Topic ChecklistVianney Angeli LorenzanaNo ratings yet
- Clinical Chemistry KeyNotes For Board ExaminationDocument12 pagesClinical Chemistry KeyNotes For Board ExaminationPrincess Alen Aguilar100% (2)
- Study Stacks - Chemistry Table Review PDFDocument14 pagesStudy Stacks - Chemistry Table Review PDF장주연100% (1)
- Chapter Blood: RBC Platelet HemostasisDocument89 pagesChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- Hematology 2Document89 pagesHematology 2Marie Llanes100% (1)
- Immunology and Serology TestsDocument2 pagesImmunology and Serology TestsPearlregine Cianne MirandaNo ratings yet
- Aubf Chemical Examination Credits To The OwnerDocument19 pagesAubf Chemical Examination Credits To The Ownerchippai100% (2)
- Methods of Studying Fungi: Dr. Alice Alma C. BungayDocument74 pagesMethods of Studying Fungi: Dr. Alice Alma C. BungayKaycee Gretz LorescaNo ratings yet
- Microbiology, Bailey - S and Scotts Chapter 28, Moraxella and Related Orgs. by MT1232Document3 pagesMicrobiology, Bailey - S and Scotts Chapter 28, Moraxella and Related Orgs. by MT1232Aisle Malibiran PalerNo ratings yet
- ML7111 MCQs Answers March 2020Document15 pagesML7111 MCQs Answers March 2020Cleo SalvadorNo ratings yet
- Clinical Chemistry ReviewDocument6 pagesClinical Chemistry Reviewclower112100% (1)
- CHEM 2 CH 29 Review QuestionsDocument2 pagesCHEM 2 CH 29 Review QuestionsthrowawyNo ratings yet
- Clinical ChemistryDocument8 pagesClinical Chemistryleizej29No ratings yet
- Medtech Laws DelfinDocument16 pagesMedtech Laws DelfinNeririNo ratings yet
- MUST To KNOW in Clinical MicrosDocument43 pagesMUST To KNOW in Clinical MicrosMerhella Amor Suerte MendozaNo ratings yet
- Group 6 - Immunohematology - Blood BankingDocument8 pagesGroup 6 - Immunohematology - Blood Bankingjulo_05No ratings yet
- Klubsybear Additional Recalls: Hematology A.karyolysisDocument2 pagesKlubsybear Additional Recalls: Hematology A.karyolysisMartin ClydeNo ratings yet
- Blood BankDocument32 pagesBlood Bankpikachu100% (1)
- IMS - Intro To Immunology and SerologyDocument3 pagesIMS - Intro To Immunology and SerologyJeanne RodiñoNo ratings yet
- Immuno-Serology & Blood Banking Case StudyDocument8 pagesImmuno-Serology & Blood Banking Case StudyRomie SolacitoNo ratings yet
- Common Plating Media For Clinical Bacteriology (From Bailey & Scott's Diagnostic Microbiology, 12th Ed)Document2 pagesCommon Plating Media For Clinical Bacteriology (From Bailey & Scott's Diagnostic Microbiology, 12th Ed)Elizabeth Enjambre HernaniNo ratings yet
- Pass Ascp 2020 LatestDocument6 pagesPass Ascp 2020 LatestLorelie ChenNo ratings yet
- Correctly: IncorrectlyDocument70 pagesCorrectly: IncorrectlyDjdjjd Siisus100% (1)
- CC Conversion-FactorsDocument1 pageCC Conversion-FactorsAndrei Tumarong AngoluanNo ratings yet
- Hematology2 - Laboratory TestsDocument3 pagesHematology2 - Laboratory Testskthmnts100% (1)
- Recalls 4Document1 pageRecalls 4Ritz Bautista BalanayNo ratings yet
- Immuno Serology ReviewDocument16 pagesImmuno Serology ReviewM CNo ratings yet
- Blood Bank ProceduresDocument33 pagesBlood Bank Procedures99noname100% (1)
- WBC AbnormalitiesDocument37 pagesWBC AbnormalitiesMajj MajjNo ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- Hematology 2 TEST QUESTIONSDocument4 pagesHematology 2 TEST QUESTIONSa a r o n b a u t i s t aNo ratings yet
- Hematology 2 Lesson 1Document9 pagesHematology 2 Lesson 1janNo ratings yet
- A. Two Forms of Carbohydrates: 1. Draw The FollowingDocument7 pagesA. Two Forms of Carbohydrates: 1. Draw The FollowingJoshua TrinidadNo ratings yet
- Automated Antimicrobial Susceptibility Test MethodDocument2 pagesAutomated Antimicrobial Susceptibility Test MethodJoshua TrinidadNo ratings yet
- CC1 11Document2 pagesCC1 11Joshua TrinidadNo ratings yet
- Case Study: QuestionsDocument2 pagesCase Study: QuestionsJoshua TrinidadNo ratings yet
- CC1 8Document4 pagesCC1 8Joshua Trinidad0% (1)
- Draw, Label and Define The Basic Instrumentation of A SpectrophotometerDocument6 pagesDraw, Label and Define The Basic Instrumentation of A SpectrophotometerJoshua TrinidadNo ratings yet
- A CLIA Waived Test Requires That OperatorsDocument3 pagesA CLIA Waived Test Requires That OperatorsJoshua TrinidadNo ratings yet
- Serologic Tests Part 1Document4 pagesSerologic Tests Part 1Joshua TrinidadNo ratings yet
- Cc1-Task 1Document2 pagesCc1-Task 1Joshua TrinidadNo ratings yet
- Mastigophora TableDocument1 pageMastigophora TableJoshua TrinidadNo ratings yet
- Serologic Tests Part 3Document2 pagesSerologic Tests Part 3Joshua TrinidadNo ratings yet
- Serologic Tests Part 5Document3 pagesSerologic Tests Part 5Joshua TrinidadNo ratings yet
- Bacteriostatic Agents: Drugs Which Bind To The 50s Ribosomal UnitDocument3 pagesBacteriostatic Agents: Drugs Which Bind To The 50s Ribosomal UnitJoshua Trinidad100% (1)
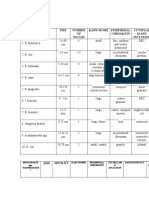
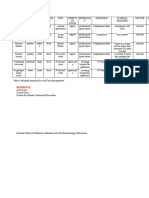
- Table 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionDocument3 pagesTable 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionJoshua TrinidadNo ratings yet
- Sporozoa TableDocument2 pagesSporozoa TableJoshua TrinidadNo ratings yet
- Wuchereria Bancrofti Brugia Malayi Loa Loa Onchocerca Volvulus Mansonella Perstans Mansonella Ozzardi Dracunculus MedinensisDocument4 pagesWuchereria Bancrofti Brugia Malayi Loa Loa Onchocerca Volvulus Mansonella Perstans Mansonella Ozzardi Dracunculus MedinensisJoshua TrinidadNo ratings yet
- Make A Tabulated Summary For Nematodes (Round Worms) : HabitatDocument4 pagesMake A Tabulated Summary For Nematodes (Round Worms) : HabitatJoshua TrinidadNo ratings yet
- Coccidia TableDocument2 pagesCoccidia TableJoshua TrinidadNo ratings yet
- Cestodes - TableDocument5 pagesCestodes - TableJoshua TrinidadNo ratings yet
- Week 1 and 2 - IntroductionDocument5 pagesWeek 1 and 2 - IntroductionJoshua TrinidadNo ratings yet
- Reviewer - Immmunohematology - Part 2Document29 pagesReviewer - Immmunohematology - Part 2Joshua TrinidadNo ratings yet
- Reviewer - Immunoserology - Part 2 PDFDocument33 pagesReviewer - Immunoserology - Part 2 PDFJoshua TrinidadNo ratings yet
- Reviewer - Immunohematology - Part 1Document16 pagesReviewer - Immunohematology - Part 1Joshua TrinidadNo ratings yet
- Reviewer - Immunoserology - Part 2 PDFDocument33 pagesReviewer - Immunoserology - Part 2 PDFJoshua TrinidadNo ratings yet
- Reviewer - Immunoserology - Part 2 PDFDocument33 pagesReviewer - Immunoserology - Part 2 PDFJoshua TrinidadNo ratings yet
- Macroglossia PDFDocument7 pagesMacroglossia PDFpaolaNo ratings yet
- 0 - Case Presentation On Uti, CKDDocument20 pages0 - Case Presentation On Uti, CKDAbin PNo ratings yet
- Chapter 20 With Comments - Acinetobacter - StenotrophomonasDocument13 pagesChapter 20 With Comments - Acinetobacter - StenotrophomonasGordon JamesonNo ratings yet
- Sarcomas SurgeryDocument8 pagesSarcomas SurgeryJüdith Marie Reyes BauntoNo ratings yet
- Acute Otitis Media in AdultsDocument15 pagesAcute Otitis Media in AdultschristineNo ratings yet
- Nursing Care Plan Impaired Skin IntegrityDocument2 pagesNursing Care Plan Impaired Skin Integritycuicuita100% (3)
- Module1 Overview HivinfectionDocument20 pagesModule1 Overview HivinfectionCristine BarrozaNo ratings yet
- Casumpang V. Cortejo G.R. No. 171127 - March 11, 2015 FactsDocument1 pageCasumpang V. Cortejo G.R. No. 171127 - March 11, 2015 FactsjaymeebqNo ratings yet
- Microbiology Lab Diagnosis by ARC PDFDocument21 pagesMicrobiology Lab Diagnosis by ARC PDFZahid iqbalNo ratings yet
- Typhoid Enteric Fever From UiA Volume 32 Final WebDocument4 pagesTyphoid Enteric Fever From UiA Volume 32 Final WebJayesh KumarNo ratings yet
- Chronic Rhinosinusitis NewDocument26 pagesChronic Rhinosinusitis NewDewanggaWahyuPrajaNo ratings yet
- Protocolo Stars CrashDocument24 pagesProtocolo Stars CrashteranrobleswaltergabrielNo ratings yet
- Aesculus Is Especially Indicated For People With Low Back Pain Who Also Have A TendencyDocument2 pagesAesculus Is Especially Indicated For People With Low Back Pain Who Also Have A Tendencyradmilo32No ratings yet
- Clerkship Manual 2021-22Document176 pagesClerkship Manual 2021-22Umair QasimNo ratings yet
- SpondilodiscitisDocument4 pagesSpondilodiscitisMihnea VulpeNo ratings yet
- Interview Guide For Nursing Health HistoryDocument3 pagesInterview Guide For Nursing Health HistoryDersly LaneNo ratings yet
- Ecgs Made Easy 5th Edition Aehlert Test BankDocument14 pagesEcgs Made Easy 5th Edition Aehlert Test BankQuinn50% (2)
- Blood Transfusion FinalDocument8 pagesBlood Transfusion FinalejkohNo ratings yet
- Bacillus Anthracis: - MorfologiDocument3 pagesBacillus Anthracis: - MorfologiCiendy ShintyaNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)
- Chronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric WongDocument7 pagesChronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric Wongjamil aldasriNo ratings yet
- Poster PPT TemplateDocument2 pagesPoster PPT TemplateNur Ainatul AtiqahNo ratings yet
- Knee Case Study 1Document4 pagesKnee Case Study 1superhoofy7186100% (1)
- PyelonephritisDocument24 pagesPyelonephritisfatihahannisahumairaNo ratings yet
- Isoxsuprine: Isoxsuprine Is Used ForDocument2 pagesIsoxsuprine: Isoxsuprine Is Used ForBryan Nartatez BautistaNo ratings yet
- Definition and Description of Schizprenia in The DSM-5Document8 pagesDefinition and Description of Schizprenia in The DSM-5Danekka TanNo ratings yet
- Med Surg Chapter 39Document6 pagesMed Surg Chapter 39Sherry Pencotty Barger100% (6)