Download as docx, pdf, or txt
You might also like
- Tessa Bailey - Find Her-Tessa Bailey (2019)Document58 pagesTessa Bailey - Find Her-Tessa Bailey (2019)Doğuş DereliköylüNo ratings yet
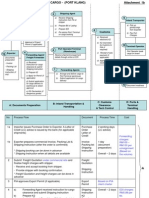
- Export + Import Process Flow - Break Bulk Cargo 27072010Document11 pagesExport + Import Process Flow - Break Bulk Cargo 27072010Ahmad Fauzi Mehat100% (1)
- DHIS Monthly Reporting Form (PHC Facilities)Document4 pagesDHIS Monthly Reporting Form (PHC Facilities)Usman89% (9)
- Muscular DystrophyDocument33 pagesMuscular DystrophyNurdina AfiniNo ratings yet
- Information About Muscular DystrophyDocument15 pagesInformation About Muscular DystrophyAcidViperNo ratings yet
- What Is Claw HandDocument36 pagesWhat Is Claw HandAndya YudhiNo ratings yet
- Tob 12.2Document28 pagesTob 12.2LT DRAGONXNo ratings yet
- By Mayo Clinic Staff: Duchenne Muscular DystrophyDocument6 pagesBy Mayo Clinic Staff: Duchenne Muscular DystrophyKatrina Clarisse HutallaNo ratings yet
- Disorders of Skeletal MuscleDocument31 pagesDisorders of Skeletal Muscleapi-19916399No ratings yet
- Muscular DystrophyDocument89 pagesMuscular Dystrophyvijay1234568883No ratings yet
- What Is Muscle Dystrophy?Document4 pagesWhat Is Muscle Dystrophy?Ryan GoldsteinNo ratings yet
- Muscular Dystrophy......Document30 pagesMuscular Dystrophy......Rupika SodhiNo ratings yet
- Associating Back Pain and Multiple SclerosisDocument2 pagesAssociating Back Pain and Multiple SclerosisAlex CostaNo ratings yet
- AGMCDocument38 pagesAGMCsmrutiptNo ratings yet
- Topic 17Document10 pagesTopic 17Bharathi Sneha PeriasamyNo ratings yet
- Muscle Cramps: Go ToDocument10 pagesMuscle Cramps: Go ToDewi AmeliyahNo ratings yet
- A Simple Guide to Muscle Dystrophy Disease and Related ConditionsFrom EverandA Simple Guide to Muscle Dystrophy Disease and Related ConditionsRating: 2 out of 5 stars2/5 (1)
- A Case To PointDocument5 pagesA Case To PointCJ PorrasNo ratings yet
- Amyotrophic Lateral SclerosisDocument17 pagesAmyotrophic Lateral SclerosisDheeraj RaiNo ratings yet
- Born With Four Wheels: Muscular DystrophyDocument11 pagesBorn With Four Wheels: Muscular DystrophyJohanNo ratings yet
- 13 Myopathic DisordersDocument58 pages13 Myopathic Disordersapi-19916399No ratings yet
- Muscular DystrophyDocument64 pagesMuscular DystrophysridharNo ratings yet
- Bio Investigatory Project of Class 12Document34 pagesBio Investigatory Project of Class 12Aditya Kadapa75% (4)
- Ayurvedic Treatment of Muscular DystrophyDocument9 pagesAyurvedic Treatment of Muscular DystrophyMukesh JainNo ratings yet
- Muscle Disorders: Dystrophic Muscular Diseasesare A Group of Mostly Hereditary Disorders Characterized by ProgressiveDocument2 pagesMuscle Disorders: Dystrophic Muscular Diseasesare A Group of Mostly Hereditary Disorders Characterized by ProgressiveSam NderituNo ratings yet
- Presentation 5 PBLDocument27 pagesPresentation 5 PBLJerin XavierNo ratings yet
- Limb-Girdle Muscular Dystrophy 2B (LGMD 2B)Document3 pagesLimb-Girdle Muscular Dystrophy 2B (LGMD 2B)Sarada Prasad NayakNo ratings yet
- Duchenne Muscular DystrophyDocument3 pagesDuchenne Muscular DystrophyhanzreinherNo ratings yet
- Anaphy Lec DiseaseDocument8 pagesAnaphy Lec DiseaseJules ConcepcionNo ratings yet
- Unit5 Handicap ModuleDocument14 pagesUnit5 Handicap Moduleted deangNo ratings yet
- Motor Neuron DiseaseDocument8 pagesMotor Neuron DiseaseyigoNo ratings yet
- Myasthenia GravisDocument8 pagesMyasthenia Gravisapi-19929147100% (1)
- 007 - Later Onset 2012 PDFDocument3 pages007 - Later Onset 2012 PDFberkay ustunNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document8 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)octiaraesyaNo ratings yet
- Muscular Dystrophy and Its Ayurvedic PerspectivesDocument149 pagesMuscular Dystrophy and Its Ayurvedic PerspectivesMuktha ShenoyNo ratings yet
- Multiple Sclerosis: Demyelination-Damages The Myelin Sheath and Neurons This Damage Slows Down orDocument6 pagesMultiple Sclerosis: Demyelination-Damages The Myelin Sheath and Neurons This Damage Slows Down orNorhana ManasNo ratings yet
- Activity 4 MedtermDocument3 pagesActivity 4 Medtermsandra seguienteNo ratings yet
- Muscular Dystrophy NoteDocument6 pagesMuscular Dystrophy NoteMd. Sherajul HaqueNo ratings yet
- Capstone PresentationDocument18 pagesCapstone Presentationapi-580341048No ratings yet
- Chronic Inflammatory Demyelinating Polyneuropathy - CIDPDocument13 pagesChronic Inflammatory Demyelinating Polyneuropathy - CIDPcarbonelNo ratings yet
- Give A 3-Sentence Summary of The Pertinent Features of The Case. What Other Details in TheDocument4 pagesGive A 3-Sentence Summary of The Pertinent Features of The Case. What Other Details in TheMiguel Andrei MedinaNo ratings yet
- Haramaya University: College of Health and Medical Science Department of Midwifery NeurologyDocument54 pagesHaramaya University: College of Health and Medical Science Department of Midwifery NeurologyMerwan KemalNo ratings yet
- Duchenne Muscular DystrophyDocument18 pagesDuchenne Muscular DystrophyLusi MunawarohNo ratings yet
- DYSTROPHYDocument15 pagesDYSTROPHYleeyan2wenty6No ratings yet
- INFANT ORIDocument13 pagesINFANT ORIFRIDAY ACHIMUGUNo ratings yet
- Ankylosing SpondilytisDocument4 pagesAnkylosing Spondilytisandreas kevinNo ratings yet
- Multiple SclerosisDocument17 pagesMultiple SclerosisSyiozz PoongundranNo ratings yet
- MyopathiesDocument26 pagesMyopathiesfarwafurqan1No ratings yet
- CASE STUDY AND QUESTIONS: To Be Completed by The 13 September Week 8 Case Study 8 AllanDocument8 pagesCASE STUDY AND QUESTIONS: To Be Completed by The 13 September Week 8 Case Study 8 Allanapi-468597987No ratings yet
- Motor Neuron DiseaseDocument18 pagesMotor Neuron Diseasevyas621995No ratings yet
- Spasticity-Overview - HandoutDocument3 pagesSpasticity-Overview - HandoutemauguerNo ratings yet
- Multiple SclerosisDocument10 pagesMultiple Sclerosisapi-247937188No ratings yet
- Myasthenia GravisDocument6 pagesMyasthenia GravisNader Smadi100% (2)
- Multiple SclerosisDocument15 pagesMultiple Sclerosiscloud kumoishNo ratings yet
- Muscular DystrophyDocument15 pagesMuscular Dystrophyrajeevsonali100% (1)
- Multiple SclerosisDocument8 pagesMultiple SclerosisNader Smadi100% (1)
- Locomotor ImpairmentDocument11 pagesLocomotor ImpairmentAbhishek BiswalNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Orthopaedia Sports Medicine0012020digitalDocument7 pagesOrthopaedia Sports Medicine0012020digitalHengame SJNo ratings yet
- Untitled PresentationDocument16 pagesUntitled PresentationtasneemsofiNo ratings yet
- Muscular Dystrophy CharactheristicsDocument3 pagesMuscular Dystrophy CharactheristicsKurt RzkyNo ratings yet
- Week FiveDocument10 pagesWeek Fiveعـَــٻاس مَـــشتاقNo ratings yet
- Polymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandPolymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (2)
- Circut Diagram For GlucometerDocument22 pagesCircut Diagram For GlucometerSaranyaNo ratings yet
- Envir Otect Power Cable Install ManualDocument49 pagesEnvir Otect Power Cable Install ManualRashi MrBRDNo ratings yet
- MUSIC Quarter 3Document13 pagesMUSIC Quarter 3RaeNo ratings yet
- Chemistry Practical Procedure Systematic Analysis of Salt STD: Xi & XiiDocument9 pagesChemistry Practical Procedure Systematic Analysis of Salt STD: Xi & XiivarshiniNo ratings yet
- List of Coolers and HeatersDocument2 pagesList of Coolers and HeatersadityasahayNo ratings yet
- Lightnng Protection As Per IEC 62305Document40 pagesLightnng Protection As Per IEC 62305Mahesh Chandra Manav100% (1)
- Anatomy by DR Naser AlBarbariDocument24 pagesAnatomy by DR Naser AlBarbariTanmay JhulkaNo ratings yet
- User S Manual Bedienungsanleitung: Version 1.0 October 1998Document32 pagesUser S Manual Bedienungsanleitung: Version 1.0 October 1998Ojit QuizonNo ratings yet
- Revelation I Excerpt PDFDocument10 pagesRevelation I Excerpt PDFMikhael ChangNo ratings yet
- Zeiss Erosion ModuleDocument13 pagesZeiss Erosion ModulepakhiddeyasNo ratings yet
- Prenatal Diagnosis of Brainstem AnomaliesDocument34 pagesPrenatal Diagnosis of Brainstem AnomaliesVishnu priya kokkulaNo ratings yet
- Avago HLCP j100, HDSP 48xxDocument7 pagesAvago HLCP j100, HDSP 48xxvelizarkoNo ratings yet
- Tutorial L298N Driver MotorDocument5 pagesTutorial L298N Driver MotorHairul Anam SNo ratings yet
- Turbojet EnginesDocument22 pagesTurbojet EnginesAldo SamuelNo ratings yet
- Prepared by - Snehal ChintalaDocument78 pagesPrepared by - Snehal ChintalaSnehal ChintalaNo ratings yet
- Cable HDMI 10 MetrosDocument3 pagesCable HDMI 10 Metroschristian eduardoNo ratings yet
- Ecs2602 Tests Bank-1Document97 pagesEcs2602 Tests Bank-1corlia100% (2)
- A2QVP2 TrainingDocument9 pagesA2QVP2 Trainingdanny wangNo ratings yet
- Electromagnetic WavesDocument173 pagesElectromagnetic WavesatiqdhepNo ratings yet
- Polynomial FunctionDocument36 pagesPolynomial FunctionfaithreignNo ratings yet
- Calibration Curve Between Pressure Drop and Mass Flow RateDocument2 pagesCalibration Curve Between Pressure Drop and Mass Flow RateMikail IsmailNo ratings yet
- MSD Numbers 0410612020 Am: ClosingDocument11 pagesMSD Numbers 0410612020 Am: ClosingSanjeev JayaratnaNo ratings yet
- Lesson 02 PDFDocument13 pagesLesson 02 PDFJeremy TohNo ratings yet
- JNTUH R09 Percentage & Credits Calculator-1Document16 pagesJNTUH R09 Percentage & Credits Calculator-1msg2dpNo ratings yet
- Definitive Guide Robot Welding Torches v1.0Document50 pagesDefinitive Guide Robot Welding Torches v1.0AlexgriNo ratings yet
- 03051Document2 pages03051JojolasNo ratings yet
- ObjectivesDocument7 pagesObjectivesPeeka booNo ratings yet