
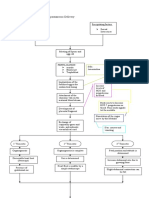
Labor and Birth Process and NURSING MANAGEMENT (Chapter 13 and 14) False Labor Factors That Affect Labor
Labor and Birth Process and NURSING MANAGEMENT (Chapter 13 and 14) False Labor Factors That Affect Labor
You might also like
- Physiology of Normal Spontaneous DeliveryDocument2 pagesPhysiology of Normal Spontaneous DeliverySummer Rain100% (2)
- Harare - Essential Guide To Management of Common Obstetric and GynaecologicDocument98 pagesHarare - Essential Guide To Management of Common Obstetric and GynaecologicTapiwa Munikwa100% (5)
- Lecture 7 - Physiology of LaborDocument30 pagesLecture 7 - Physiology of LaborMelissa Aina Mohd Yusof100% (1)
- Nur - 100 Session 2 - SemillaDocument6 pagesNur - 100 Session 2 - SemillaVon R Semilla100% (1)
- Chapter 15 - Labor and Birth: Ob LectureDocument15 pagesChapter 15 - Labor and Birth: Ob LectureMARIA PEARLITA TANNo ratings yet
- Problem With The PassageDocument3 pagesProblem With The PassageLuiciaNo ratings yet
- MD901F Cataloge PDFDocument2 pagesMD901F Cataloge PDFPT Anugerah Mitra MandiriNo ratings yet
- 7-Onset & Physiology of LaborDocument15 pages7-Onset & Physiology of LaborNlsNo ratings yet
- Intrapartum 1: Intrapartum Period Intrapartal CareDocument10 pagesIntrapartum 1: Intrapartum Period Intrapartal CareJane MartinNo ratings yet
- Ncma217 Week 7Document5 pagesNcma217 Week 7Polly ArcheronNo ratings yet
- Overview: Intrapartum Care:: Oxytocin TheoryDocument5 pagesOverview: Intrapartum Care:: Oxytocin TheoryZach BuenavistaNo ratings yet
- MCN MidtermsDocument39 pagesMCN MidtermsJinnijinniNo ratings yet
- NCM 107 - SL - Mat - 1Document100 pagesNCM 107 - SL - Mat - 1marilexdomagsangNo ratings yet
- Intrapartal PeriodDocument6 pagesIntrapartal PeriodKelsey MacaraigNo ratings yet
- LaborDocument32 pagesLaborJustine Vens G. AgustinNo ratings yet
- Ob Lec - Theories of LaborDocument10 pagesOb Lec - Theories of Labortmjrsvz84mNo ratings yet
- 2 August 28Document20 pages2 August 28Emily ChiaravallotiNo ratings yet
- OB1 3.1 Normal Labor and Delivery IDocument6 pagesOB1 3.1 Normal Labor and Delivery IManjulaNo ratings yet
- Intrartum/Intrapartal Period: Phenomena and Process of Labor and Delivery I. Onset of LaborDocument14 pagesIntrartum/Intrapartal Period: Phenomena and Process of Labor and Delivery I. Onset of Laborclaireaongchua1275No ratings yet
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocument48 pagesNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- Physiology of Parturition PDFDocument17 pagesPhysiology of Parturition PDFNestley TiongsonNo ratings yet
- Hands Out 3 LaborDocument29 pagesHands Out 3 LaborErin SaavedraNo ratings yet
- Finals Com ElearningDocument35 pagesFinals Com ElearningGladys JhayeNo ratings yet
- (ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Document12 pages(ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Karen EstavilloNo ratings yet
- Phy Ist Stag LBRDocument9 pagesPhy Ist Stag LBRAparna KinginiNo ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras AliNo ratings yet
- 3F Intranatal NotesDocument5 pages3F Intranatal NotesAlyssa Claire TumulakNo ratings yet
- Normal Labor: Obstetrics and GynecologyDocument3 pagesNormal Labor: Obstetrics and GynecologyLuis PadillaNo ratings yet
- Problem With The PowersDocument9 pagesProblem With The PowersNicole Claire LegaspiNo ratings yet
- ABC Care PentingDocument4 pagesABC Care PentingDina Ayu SavitriNo ratings yet
- n3633 MM Module 1 Unit 1Document71 pagesn3633 MM Module 1 Unit 1jonscastro450No ratings yet
- Intrapartum Complications: Kristen AzusanoDocument3 pagesIntrapartum Complications: Kristen AzusanokirbsNo ratings yet
- MCHN FinalsDocument26 pagesMCHN FinalsMahdiyah AgasNo ratings yet
- Onset of LaborDocument4 pagesOnset of LaborK louiseNo ratings yet
- Maternal Reviewer MidtermmDocument5 pagesMaternal Reviewer Midtermmriveraapriljan22No ratings yet
- What Is LaborDocument8 pagesWhat Is LaborEdsylaine BumatayNo ratings yet
- Faal Partus: Naifah Luthfiyah Putri 15-009Document58 pagesFaal Partus: Naifah Luthfiyah Putri 15-009NaifahLuthfiyahPutriNo ratings yet
- Maternal & Child Health Nursing Flashcards QuizletDocument1 pageMaternal & Child Health Nursing Flashcards QuizletJosh PagnamitanNo ratings yet
- Intrapartum-Unit ExamDocument2 pagesIntrapartum-Unit ExamChris AnnNo ratings yet
- OB2 - Problems With The PowerDocument10 pagesOB2 - Problems With The PowerYanaNo ratings yet
- Labor and DeliveryDocument7 pagesLabor and DeliveryMikaella CondeNo ratings yet
- ANNOTATIONDocument2 pagesANNOTATIONVaniegrace Angel BalagonNo ratings yet
- Client Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipDocument2 pagesClient Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipLyssa Monique67% (3)
- 1 Labor and Delivery ProcessDocument13 pages1 Labor and Delivery ProcessBardiaga JmayNo ratings yet
- COMPONENTS OF LABOR - 5PsDocument5 pagesCOMPONENTS OF LABOR - 5PslumpiaNo ratings yet
- LESSON-PLAN-ON-PHYSIOLogical Changes During PregnancyDocument22 pagesLESSON-PLAN-ON-PHYSIOLogical Changes During PregnancyV.srivaniNo ratings yet
- Puerperium (Trans)Document7 pagesPuerperium (Trans)Charlie65129No ratings yet
- MALPRESENTATIONDocument13 pagesMALPRESENTATIONLady Jane CaguladaNo ratings yet
- Normal Labor and DeliveryDocument142 pagesNormal Labor and DeliveryRosalie RoselloNo ratings yet
- Abnormal Labor and Infertility 2016 PDFDocument12 pagesAbnormal Labor and Infertility 2016 PDFLarissa TacalanNo ratings yet
- Abnormal Labor + InfertilityDocument12 pagesAbnormal Labor + InfertilityKristine VanzuelaNo ratings yet
- Normal LaborDocument42 pagesNormal Laborhacker ammerNo ratings yet
- Definition: Related Diagnostic TestsDocument8 pagesDefinition: Related Diagnostic TestsQuinn Xylon VillanuevaNo ratings yet
- 10.theories of LaborDocument18 pages10.theories of LaborJulia Ramos100% (1)
- Holistic Pregnancy Manual: Maternal Health Manuals, #1From EverandHolistic Pregnancy Manual: Maternal Health Manuals, #1No ratings yet
- It Takes Two... And a Uterus: The Ultimate Guide to Understanding and Enhancing Your FertilityFrom EverandIt Takes Two... And a Uterus: The Ultimate Guide to Understanding and Enhancing Your FertilityNo ratings yet
- Teen Girl Guide to Puberty: Understanding Hormonal Changes, Body care and Personal HygieneFrom EverandTeen Girl Guide to Puberty: Understanding Hormonal Changes, Body care and Personal HygieneNo ratings yet
- How to Boost Your Fertility and Get Pregnant FastFrom EverandHow to Boost Your Fertility and Get Pregnant FastRating: 5 out of 5 stars5/5 (1)
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-IDocument6 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (1)
- OB Drug Study - OxytocinDocument3 pagesOB Drug Study - OxytocinJustin AncogNo ratings yet
- Fetal Distress: Philip J. SteerDocument7 pagesFetal Distress: Philip J. Steeryenni anggrainiNo ratings yet
- Partograph NextDocument50 pagesPartograph NextPrag GK Subedi0% (1)
- Fetal Assessment DRDocument1 pageFetal Assessment DRMicah Lou CalambaNo ratings yet
- Conduct of Normal Labor and DeliveryDocument141 pagesConduct of Normal Labor and DeliveryRea Dominique CabanillaNo ratings yet
- Carla Hernandez 100Document4 pagesCarla Hernandez 100JhunnieEy ReyesNo ratings yet
- Post-Term Labor - NCPDocument7 pagesPost-Term Labor - NCPCameron De GuzmanNo ratings yet
- Introduction of Labour MonitoringDocument29 pagesIntroduction of Labour MonitoringMishti MokarramaNo ratings yet
- Apfs 2012 MidDocument79 pagesApfs 2012 Middaniel meresaNo ratings yet
- OB I For 2nd YearDocument122 pagesOB I For 2nd YeardiribaNo ratings yet
- Labor and DeliveryDocument14 pagesLabor and Deliverydexter100% (15)
- Shoulder DystociaDocument20 pagesShoulder DystociaDanielle Francis Hirang0% (1)
- Osce - Non Stress Test Remarks YES NODocument3 pagesOsce - Non Stress Test Remarks YES NOKALAI AKSHAYANo ratings yet
- Nursing Care of The Family During Labor and BirthDocument16 pagesNursing Care of The Family During Labor and BirthGladys YaresNo ratings yet
- ფიზიოლოგიური მშობიარობის მართვაDocument30 pagesფიზიოლოგიური მშობიარობის მართვაAchi BeridzeNo ratings yet
- Government College of Nursing Jodhpur (Raj.)Document5 pagesGovernment College of Nursing Jodhpur (Raj.)priyanka100% (1)
- Mengukur DJJDocument6 pagesMengukur DJJYuni PurwatiNo ratings yet
- Radha Antenatal Fetal Well Being1Document32 pagesRadha Antenatal Fetal Well Being1Shaells JoshiNo ratings yet
- Nlex - MCNDocument19 pagesNlex - MCNAileen AlphaNo ratings yet
- Obg Unit - 4Document55 pagesObg Unit - 4Preeti ChouhanNo ratings yet
- Chapter 9 (Margot-Desevo)Document11 pagesChapter 9 (Margot-Desevo)Jesse ParkNo ratings yet
- Obs-UM - Paper - 1Document16 pagesObs-UM - Paper - 1Muhammad Abbas AliNo ratings yet
- Antepartum Fetal Surveillance ACOG Bulletin 2014-1Document11 pagesAntepartum Fetal Surveillance ACOG Bulletin 2014-1William Rodriguez CoronadoNo ratings yet
- Sonicaid Team CTG - Operators Manual PDFDocument113 pagesSonicaid Team CTG - Operators Manual PDFDaniel Galindo100% (1)
- MCHN Finals 1st-QuizDocument20 pagesMCHN Finals 1st-QuizhknNo ratings yet
- Contraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsDocument3 pagesContraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsSagar HanamasagarNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Physiology of Normal Spontaneous DeliveryDocument2 pagesPhysiology of Normal Spontaneous DeliverySummer Rain100% (2)
- Harare - Essential Guide To Management of Common Obstetric and GynaecologicDocument98 pagesHarare - Essential Guide To Management of Common Obstetric and GynaecologicTapiwa Munikwa100% (5)
- Lecture 7 - Physiology of LaborDocument30 pagesLecture 7 - Physiology of LaborMelissa Aina Mohd Yusof100% (1)
- Nur - 100 Session 2 - SemillaDocument6 pagesNur - 100 Session 2 - SemillaVon R Semilla100% (1)
- Chapter 15 - Labor and Birth: Ob LectureDocument15 pagesChapter 15 - Labor and Birth: Ob LectureMARIA PEARLITA TANNo ratings yet
- Problem With The PassageDocument3 pagesProblem With The PassageLuiciaNo ratings yet
- MD901F Cataloge PDFDocument2 pagesMD901F Cataloge PDFPT Anugerah Mitra MandiriNo ratings yet
- 7-Onset & Physiology of LaborDocument15 pages7-Onset & Physiology of LaborNlsNo ratings yet
- Intrapartum 1: Intrapartum Period Intrapartal CareDocument10 pagesIntrapartum 1: Intrapartum Period Intrapartal CareJane MartinNo ratings yet
- Ncma217 Week 7Document5 pagesNcma217 Week 7Polly ArcheronNo ratings yet
- Overview: Intrapartum Care:: Oxytocin TheoryDocument5 pagesOverview: Intrapartum Care:: Oxytocin TheoryZach BuenavistaNo ratings yet
- MCN MidtermsDocument39 pagesMCN MidtermsJinnijinniNo ratings yet
- NCM 107 - SL - Mat - 1Document100 pagesNCM 107 - SL - Mat - 1marilexdomagsangNo ratings yet
- Intrapartal PeriodDocument6 pagesIntrapartal PeriodKelsey MacaraigNo ratings yet
- LaborDocument32 pagesLaborJustine Vens G. AgustinNo ratings yet
- Ob Lec - Theories of LaborDocument10 pagesOb Lec - Theories of Labortmjrsvz84mNo ratings yet
- 2 August 28Document20 pages2 August 28Emily ChiaravallotiNo ratings yet
- OB1 3.1 Normal Labor and Delivery IDocument6 pagesOB1 3.1 Normal Labor and Delivery IManjulaNo ratings yet
- Intrartum/Intrapartal Period: Phenomena and Process of Labor and Delivery I. Onset of LaborDocument14 pagesIntrartum/Intrapartal Period: Phenomena and Process of Labor and Delivery I. Onset of Laborclaireaongchua1275No ratings yet
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocument48 pagesNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- Physiology of Parturition PDFDocument17 pagesPhysiology of Parturition PDFNestley TiongsonNo ratings yet
- Hands Out 3 LaborDocument29 pagesHands Out 3 LaborErin SaavedraNo ratings yet
- Finals Com ElearningDocument35 pagesFinals Com ElearningGladys JhayeNo ratings yet
- (ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Document12 pages(ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Karen EstavilloNo ratings yet
- Phy Ist Stag LBRDocument9 pagesPhy Ist Stag LBRAparna KinginiNo ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras AliNo ratings yet
- 3F Intranatal NotesDocument5 pages3F Intranatal NotesAlyssa Claire TumulakNo ratings yet
- Normal Labor: Obstetrics and GynecologyDocument3 pagesNormal Labor: Obstetrics and GynecologyLuis PadillaNo ratings yet
- Problem With The PowersDocument9 pagesProblem With The PowersNicole Claire LegaspiNo ratings yet
- ABC Care PentingDocument4 pagesABC Care PentingDina Ayu SavitriNo ratings yet
- n3633 MM Module 1 Unit 1Document71 pagesn3633 MM Module 1 Unit 1jonscastro450No ratings yet
- Intrapartum Complications: Kristen AzusanoDocument3 pagesIntrapartum Complications: Kristen AzusanokirbsNo ratings yet
- MCHN FinalsDocument26 pagesMCHN FinalsMahdiyah AgasNo ratings yet
- Onset of LaborDocument4 pagesOnset of LaborK louiseNo ratings yet
- Maternal Reviewer MidtermmDocument5 pagesMaternal Reviewer Midtermmriveraapriljan22No ratings yet
- What Is LaborDocument8 pagesWhat Is LaborEdsylaine BumatayNo ratings yet
- Faal Partus: Naifah Luthfiyah Putri 15-009Document58 pagesFaal Partus: Naifah Luthfiyah Putri 15-009NaifahLuthfiyahPutriNo ratings yet
- Maternal & Child Health Nursing Flashcards QuizletDocument1 pageMaternal & Child Health Nursing Flashcards QuizletJosh PagnamitanNo ratings yet
- Intrapartum-Unit ExamDocument2 pagesIntrapartum-Unit ExamChris AnnNo ratings yet
- OB2 - Problems With The PowerDocument10 pagesOB2 - Problems With The PowerYanaNo ratings yet
- Labor and DeliveryDocument7 pagesLabor and DeliveryMikaella CondeNo ratings yet
- ANNOTATIONDocument2 pagesANNOTATIONVaniegrace Angel BalagonNo ratings yet
- Client Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipDocument2 pagesClient Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipLyssa Monique67% (3)
- 1 Labor and Delivery ProcessDocument13 pages1 Labor and Delivery ProcessBardiaga JmayNo ratings yet
- COMPONENTS OF LABOR - 5PsDocument5 pagesCOMPONENTS OF LABOR - 5PslumpiaNo ratings yet
- LESSON-PLAN-ON-PHYSIOLogical Changes During PregnancyDocument22 pagesLESSON-PLAN-ON-PHYSIOLogical Changes During PregnancyV.srivaniNo ratings yet
- Puerperium (Trans)Document7 pagesPuerperium (Trans)Charlie65129No ratings yet
- MALPRESENTATIONDocument13 pagesMALPRESENTATIONLady Jane CaguladaNo ratings yet
- Normal Labor and DeliveryDocument142 pagesNormal Labor and DeliveryRosalie RoselloNo ratings yet
- Abnormal Labor and Infertility 2016 PDFDocument12 pagesAbnormal Labor and Infertility 2016 PDFLarissa TacalanNo ratings yet
- Abnormal Labor + InfertilityDocument12 pagesAbnormal Labor + InfertilityKristine VanzuelaNo ratings yet
- Normal LaborDocument42 pagesNormal Laborhacker ammerNo ratings yet
- Definition: Related Diagnostic TestsDocument8 pagesDefinition: Related Diagnostic TestsQuinn Xylon VillanuevaNo ratings yet
- 10.theories of LaborDocument18 pages10.theories of LaborJulia Ramos100% (1)
- Holistic Pregnancy Manual: Maternal Health Manuals, #1From EverandHolistic Pregnancy Manual: Maternal Health Manuals, #1No ratings yet
- It Takes Two... And a Uterus: The Ultimate Guide to Understanding and Enhancing Your FertilityFrom EverandIt Takes Two... And a Uterus: The Ultimate Guide to Understanding and Enhancing Your FertilityNo ratings yet
- Teen Girl Guide to Puberty: Understanding Hormonal Changes, Body care and Personal HygieneFrom EverandTeen Girl Guide to Puberty: Understanding Hormonal Changes, Body care and Personal HygieneNo ratings yet
- How to Boost Your Fertility and Get Pregnant FastFrom EverandHow to Boost Your Fertility and Get Pregnant FastRating: 5 out of 5 stars5/5 (1)
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-IDocument6 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (1)
- OB Drug Study - OxytocinDocument3 pagesOB Drug Study - OxytocinJustin AncogNo ratings yet
- Fetal Distress: Philip J. SteerDocument7 pagesFetal Distress: Philip J. Steeryenni anggrainiNo ratings yet
- Partograph NextDocument50 pagesPartograph NextPrag GK Subedi0% (1)
- Fetal Assessment DRDocument1 pageFetal Assessment DRMicah Lou CalambaNo ratings yet
- Conduct of Normal Labor and DeliveryDocument141 pagesConduct of Normal Labor and DeliveryRea Dominique CabanillaNo ratings yet
- Carla Hernandez 100Document4 pagesCarla Hernandez 100JhunnieEy ReyesNo ratings yet
- Post-Term Labor - NCPDocument7 pagesPost-Term Labor - NCPCameron De GuzmanNo ratings yet
- Introduction of Labour MonitoringDocument29 pagesIntroduction of Labour MonitoringMishti MokarramaNo ratings yet
- Apfs 2012 MidDocument79 pagesApfs 2012 Middaniel meresaNo ratings yet
- OB I For 2nd YearDocument122 pagesOB I For 2nd YeardiribaNo ratings yet
- Labor and DeliveryDocument14 pagesLabor and Deliverydexter100% (15)
- Shoulder DystociaDocument20 pagesShoulder DystociaDanielle Francis Hirang0% (1)
- Osce - Non Stress Test Remarks YES NODocument3 pagesOsce - Non Stress Test Remarks YES NOKALAI AKSHAYANo ratings yet
- Nursing Care of The Family During Labor and BirthDocument16 pagesNursing Care of The Family During Labor and BirthGladys YaresNo ratings yet
- ფიზიოლოგიური მშობიარობის მართვაDocument30 pagesფიზიოლოგიური მშობიარობის მართვაAchi BeridzeNo ratings yet
- Government College of Nursing Jodhpur (Raj.)Document5 pagesGovernment College of Nursing Jodhpur (Raj.)priyanka100% (1)
- Mengukur DJJDocument6 pagesMengukur DJJYuni PurwatiNo ratings yet
- Radha Antenatal Fetal Well Being1Document32 pagesRadha Antenatal Fetal Well Being1Shaells JoshiNo ratings yet
- Nlex - MCNDocument19 pagesNlex - MCNAileen AlphaNo ratings yet
- Obg Unit - 4Document55 pagesObg Unit - 4Preeti ChouhanNo ratings yet
- Chapter 9 (Margot-Desevo)Document11 pagesChapter 9 (Margot-Desevo)Jesse ParkNo ratings yet
- Obs-UM - Paper - 1Document16 pagesObs-UM - Paper - 1Muhammad Abbas AliNo ratings yet
- Antepartum Fetal Surveillance ACOG Bulletin 2014-1Document11 pagesAntepartum Fetal Surveillance ACOG Bulletin 2014-1William Rodriguez CoronadoNo ratings yet
- Sonicaid Team CTG - Operators Manual PDFDocument113 pagesSonicaid Team CTG - Operators Manual PDFDaniel Galindo100% (1)
- MCHN Finals 1st-QuizDocument20 pagesMCHN Finals 1st-QuizhknNo ratings yet
- Contraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsDocument3 pagesContraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsSagar HanamasagarNo ratings yet