Download as pdf or txt
You might also like
- Pathophysiology The Biologic Basis For Disease in Adults and Children 8th Edition Mccance Test BankDocument36 pagesPathophysiology The Biologic Basis For Disease in Adults and Children 8th Edition Mccance Test Bankturnmiddayu0ppsx100% (26)
- Pathophysiology The Biologic Basis For Disease in Adults and Children 8th Edition Mccance Test BankDocument25 pagesPathophysiology The Biologic Basis For Disease in Adults and Children 8th Edition Mccance Test BankEarlCollinsmapcs100% (31)
- Understanding Pathophysiology 6th Edition Test BankDocument8 pagesUnderstanding Pathophysiology 6th Edition Test BankAlex0% (1)
- Good Information BTC PDFDocument45 pagesGood Information BTC PDFPatrick Perez75% (4)
- Answer Key For EmpleoDocument17 pagesAnswer Key For EmpleoAdrian Montemayor100% (2)
- Krebs Cycle Anions in Metabolic Acidosis: CommentaryDocument2 pagesKrebs Cycle Anions in Metabolic Acidosis: CommentaryAriadna Vieyra CalderónNo ratings yet
- Sir David Cuthbertson Medal Lecture - Fluid, Electrolytes and Nutrition: Physiological and Clinical AspectsDocument15 pagesSir David Cuthbertson Medal Lecture - Fluid, Electrolytes and Nutrition: Physiological and Clinical AspectsThinh VinhNo ratings yet
- Nutritional Support in The Perioperative Period: 4 Fluid Balance and Metabolism in SurgeryDocument29 pagesNutritional Support in The Perioperative Period: 4 Fluid Balance and Metabolism in SurgeryFreddy Negron HuamaniNo ratings yet
- FLUID, ELECTROLYTE, AND ACID-BASE PHYSIOLOGY - A PROBLEM-BASED APPROACH (4E) (2010) (UnitedVRG) PDFDocument614 pagesFLUID, ELECTROLYTE, AND ACID-BASE PHYSIOLOGY - A PROBLEM-BASED APPROACH (4E) (2010) (UnitedVRG) PDFCristinaLucan100% (2)
- Schillaci 2017Document22 pagesSchillaci 2017Sarranya ParanthamanNo ratings yet
- Structural Studies of Flaa1 From Helicobacter Pylori Reveal The Mechanism For Inverting 4,6-Dehydratase ActivityDocument8 pagesStructural Studies of Flaa1 From Helicobacter Pylori Reveal The Mechanism For Inverting 4,6-Dehydratase Activityjuan acostaNo ratings yet
- Kwasiorkor 2022Document2 pagesKwasiorkor 2022Gilbert MenesesNo ratings yet
- Case 1 CKDocument4 pagesCase 1 CKmcpaulfreemanNo ratings yet
- Hypokalemia and Anesthetic Implications: Wong, Patrick Schafer, and John R. SchultzDocument23 pagesHypokalemia and Anesthetic Implications: Wong, Patrick Schafer, and John R. SchultzRidski D. MiruNo ratings yet
- Hiperpotasemia KDIGODocument20 pagesHiperpotasemia KDIGOAndy MaciasNo ratings yet
- Metabolic Regulation of The Cell Cycle: in Hye Lee and Toren FinkelDocument6 pagesMetabolic Regulation of The Cell Cycle: in Hye Lee and Toren FinkelLuis RojasNo ratings yet
- KDIGO Potassium Management Corrected ProofDocument20 pagesKDIGO Potassium Management Corrected ProofshaheershayanqaziNo ratings yet
- 3 The Unexpected Capacity of Melanin To PDFDocument2 pages3 The Unexpected Capacity of Melanin To PDFOdessa FileNo ratings yet
- Hipercloremia en SepsisDocument8 pagesHipercloremia en SepsisConsuelo Noriega de MolinaNo ratings yet
- No Resucitar Con SalinaDocument4 pagesNo Resucitar Con SalinaAntonia Holguin HoyosNo ratings yet
- In Vivo Antiaging Effects of Alkaline Water Supplementation: Research PaperDocument8 pagesIn Vivo Antiaging Effects of Alkaline Water Supplementation: Research PaperSandeep_Charu_2989No ratings yet
- The Red Cell Storage Lesion andDocument12 pagesThe Red Cell Storage Lesion andhasanahNo ratings yet
- Hyperkalemia: Pathophysiology, Risk Factors and ConsequencesDocument10 pagesHyperkalemia: Pathophysiology, Risk Factors and Consequences李德富No ratings yet
- Lac TranspDocument13 pagesLac Transpfarinha2009No ratings yet
- Balanced Versus Unbalanced Salt Solutions What (Raisul)Document13 pagesBalanced Versus Unbalanced Salt Solutions What (Raisul)irmaarmiyahNo ratings yet
- Lymphoid Crisis Myeloid Leukaemia: Blast in ChronicDocument2 pagesLymphoid Crisis Myeloid Leukaemia: Blast in ChronicThistell ThistleNo ratings yet
- AP Biology SGO ContentDocument5 pagesAP Biology SGO ContentIrina ShutovskyNo ratings yet
- Acid-Base and Potassium HomeostasisDocument8 pagesAcid-Base and Potassium HomeostasisVeronica WongNo ratings yet
- Hypo Kale MiaDocument11 pagesHypo Kale MiaAlifianiii KartikaNo ratings yet
- New Acid BaeDocument6 pagesNew Acid BaeEnrique MartinezNo ratings yet
- Phenylketonuria. Differentiate "MapleDocument3 pagesPhenylketonuria. Differentiate "MapleTim SeidenstückerNo ratings yet
- Lactic Acidosis: D. de BackerDocument4 pagesLactic Acidosis: D. de BackerindrekvNo ratings yet
- Metabolic Acidosis: Pathophysiology, Diagnosis and ManagementDocument13 pagesMetabolic Acidosis: Pathophysiology, Diagnosis and ManagementPedro Daniel Alcívar MendozaNo ratings yet
- Asidosis Laktat 2Document10 pagesAsidosis Laktat 2MizanMaulanaNo ratings yet
- CBS Signalling TutorialDocument7 pagesCBS Signalling TutorialAbdulmuizz QNo ratings yet
- Kwashiorkor Revisited: The Pathogenesis of Oedema in Kwashiorkor and Its SignificanceDocument6 pagesKwashiorkor Revisited: The Pathogenesis of Oedema in Kwashiorkor and Its SignificanceAimee PhNo ratings yet
- N-Acetyltransferase The Practical Consequences of Polymorphic Activity in ManDocument16 pagesN-Acetyltransferase The Practical Consequences of Polymorphic Activity in ManIsrael GonzalezNo ratings yet
- Biochimica Et Biophysica ActaDocument7 pagesBiochimica Et Biophysica ActaPayam ParaviNo ratings yet
- The Role of Fatty Acid Metabolism and Lipotoxicity in Pancreatic B-Cell Injury: Identification of Potential Therapeutic TargetsDocument7 pagesThe Role of Fatty Acid Metabolism and Lipotoxicity in Pancreatic B-Cell Injury: Identification of Potential Therapeutic TargetsHarsh Agarwal phya 016No ratings yet
- 2013 Basic Concepts of Fluid and Electrolyte TherapyDocument137 pages2013 Basic Concepts of Fluid and Electrolyte Therapytd5xb7w4dpNo ratings yet
- Intestinal Ion Transport and The Pathophysiology of DiarrheaDocument13 pagesIntestinal Ion Transport and The Pathophysiology of Diarrheajuanfraflores9777No ratings yet
- Aka ReviewDocument4 pagesAka ReviewminhaboomboxNo ratings yet
- A Single Nutrient Feed Supports Both Chemically Defined NS0 and CHODocument11 pagesA Single Nutrient Feed Supports Both Chemically Defined NS0 and CHOMingzhong ChenNo ratings yet
- 2013 Basic Concepts of Fluid and Electrolyte TherapyDocument137 pages2013 Basic Concepts of Fluid and Electrolyte TherapySarahNo ratings yet
- Urea and Protein Carbamylation in ESRD: Surrogate Markers or Partners in Crime?Document3 pagesUrea and Protein Carbamylation in ESRD: Surrogate Markers or Partners in Crime?m29hereNo ratings yet
- Risks of Chronic Metabolic Acidosis in Patients With Chronic Kidney DiseaseDocument9 pagesRisks of Chronic Metabolic Acidosis in Patients With Chronic Kidney DiseaseAkbar GazaliNo ratings yet
- Jurnal 5Document4 pagesJurnal 5Ciendy ShintyaNo ratings yet
- Structural Studies of A Calmodulin Mutant With Defective Regulation of Muscle Contraction John Emmons and Adina KilpatrickDocument10 pagesStructural Studies of A Calmodulin Mutant With Defective Regulation of Muscle Contraction John Emmons and Adina KilpatrickzaxNo ratings yet
- Role of CFTR in Epithelial Physiology: Cellular and Molecular Life SciencesDocument23 pagesRole of CFTR in Epithelial Physiology: Cellular and Molecular Life Sciencesshaheena ahmedNo ratings yet
- Mitochondrial Correction A New Therapeutic Paradigm For Cancer and Degenerative Diseases JOM 33.4Document20 pagesMitochondrial Correction A New Therapeutic Paradigm For Cancer and Degenerative Diseases JOM 33.4La Isla OesteNo ratings yet
- AJKD Atlas of Renal Pathology Lecithin-CholesterolDocument3 pagesAJKD Atlas of Renal Pathology Lecithin-CholesterolSa7arNo ratings yet
- Late-Onset Alzheimers Disease Is Associated WithDocument13 pagesLate-Onset Alzheimers Disease Is Associated WithAlix AliNo ratings yet
- ALCAR Longevity GenesDocument16 pagesALCAR Longevity GenescumbredinNo ratings yet
- Tendency: A To atDocument5 pagesTendency: A To atAdria Putra FarhandikaNo ratings yet
- Engle Hart 2006Document6 pagesEngle Hart 2006pinandhitaNo ratings yet
- Adv Nutr 2011 Levine 78 88Document11 pagesAdv Nutr 2011 Levine 78 88Wilson Campos RojasNo ratings yet
- Clinical Use of Plasma Lactate Concentration. Part 1: Physiology, Pathophysiology, and MeasurementDocument21 pagesClinical Use of Plasma Lactate Concentration. Part 1: Physiology, Pathophysiology, and MeasurementJeaneth SamaniegoNo ratings yet
- Role of Nadph:Cytochrome C Reducã-Aseand Dt-Diaphorase in The Biotransformation of Mitomycin C1Document7 pagesRole of Nadph:Cytochrome C Reducã-Aseand Dt-Diaphorase in The Biotransformation of Mitomycin C1Krys tallNo ratings yet
- Radiology, Hospital, Assistance Making: of We Owe Com-OnDocument9 pagesRadiology, Hospital, Assistance Making: of We Owe Com-OnSanja KaranovicNo ratings yet
- Erazo-Oliveras Et Al. 2022 Dysregulation of Cellular Membrane Homeostasis As A Crucial Modulator of Cancer RiskDocument54 pagesErazo-Oliveras Et Al. 2022 Dysregulation of Cellular Membrane Homeostasis As A Crucial Modulator of Cancer RiskMARIANGEL CARO REYESNo ratings yet
- The Acinar-Ductal Tango in The Pathogenesis of Acute PancreatitisDocument10 pagesThe Acinar-Ductal Tango in The Pathogenesis of Acute Pancreatitispruebaprueba321765No ratings yet
- Role of the Gut Flora in Toxicity and CancerFrom EverandRole of the Gut Flora in Toxicity and CancerI RowlandNo ratings yet
- 1993 - Linolenic Acid Flaxseed (Linum Usitatissimum)Document12 pages1993 - Linolenic Acid Flaxseed (Linum Usitatissimum)Geanelly SALGADO URIOSTEGUINo ratings yet
- 2020 - Draft Genome of Meyerozyma GuilliermondiiDocument6 pages2020 - Draft Genome of Meyerozyma GuilliermondiiGeanelly SALGADO URIOSTEGUINo ratings yet
- 2020 - Cyanobacterial PolyhydroxyalkanoatesDocument24 pages2020 - Cyanobacterial PolyhydroxyalkanoatesGeanelly SALGADO URIOSTEGUINo ratings yet
- 1981 - Immunological Comparison of Ribosomal Proteins FromDocument7 pages1981 - Immunological Comparison of Ribosomal Proteins FromGeanelly SALGADO URIOSTEGUINo ratings yet
- YSI 5300A Biological Oxygen Monitor Manual ADocument48 pagesYSI 5300A Biological Oxygen Monitor Manual AGeanelly SALGADO URIOSTEGUINo ratings yet
- 2020 - Outdoor Cultivation of Chlorella Sorokiniana in Third GenerationDocument7 pages2020 - Outdoor Cultivation of Chlorella Sorokiniana in Third GenerationGeanelly SALGADO URIOSTEGUINo ratings yet
- 1991 - Metabolism of (2-14C) Acetate and Its Use in Assessing Hepatic KrebDocument6 pages1991 - Metabolism of (2-14C) Acetate and Its Use in Assessing Hepatic KrebGeanelly SALGADO URIOSTEGUINo ratings yet
- 2020 - Effect of Iron Oxide Nanoparticles On Growth and Biofuel Potential ofDocument11 pages2020 - Effect of Iron Oxide Nanoparticles On Growth and Biofuel Potential ofGeanelly SALGADO URIOSTEGUINo ratings yet
- 1 s2.0 S0960852410008023 MainDocument9 pages1 s2.0 S0960852410008023 MainGeanelly SALGADO URIOSTEGUINo ratings yet
- 2011 - Preparation of Monolithic CatalystsDocument38 pages2011 - Preparation of Monolithic CatalystsGeanelly SALGADO URIOSTEGUINo ratings yet
- Circadian RhythmsDocument2 pagesCircadian RhythmsOmar Saleh100% (1)
- GTAG3 Audit KontinyuDocument37 pagesGTAG3 Audit KontinyujonisupriadiNo ratings yet
- Secret of Richard HadleeDocument3 pagesSecret of Richard HadleeucallmeshwetaNo ratings yet
- DuwarDocument2 pagesDuwarMy ChannelNo ratings yet
- Capital Structure DeterminationDocument20 pagesCapital Structure DeterminationJeet SummerNo ratings yet
- Methodology For Wood Door Jamb InstallationDocument1 pageMethodology For Wood Door Jamb InstallationKamen RiderNo ratings yet
- Last Call For Love Montana Dreams Book 3 Ember Kelly Full ChapterDocument67 pagesLast Call For Love Montana Dreams Book 3 Ember Kelly Full Chaptermary.brinks380100% (9)
- Normal To Real Flow Rate and FAD Flow RateDocument25 pagesNormal To Real Flow Rate and FAD Flow RateChristopher LloydNo ratings yet
- Thermal Protection and Gate Protection of SCRDocument5 pagesThermal Protection and Gate Protection of SCRSnehasis BarikNo ratings yet
- Battery Unit ServicingDocument8 pagesBattery Unit ServicingLeonardo Alfonso Carcamo CarreñoNo ratings yet
- Technical Writing by Steve M. Gerson.Document696 pagesTechnical Writing by Steve M. Gerson.mharis.bee22seecsNo ratings yet
- Validation LetterDocument2 pagesValidation LetterChrisper EscotoNo ratings yet
- R514A CVHE Centravac Centrifugal Chiller Dimension DrawingsDocument13 pagesR514A CVHE Centravac Centrifugal Chiller Dimension DrawingsBegundalz PotterNo ratings yet
- N2XCY 1 X (1.5-800) MM 0.6/1 KVDocument5 pagesN2XCY 1 X (1.5-800) MM 0.6/1 KVCombox BlackNo ratings yet
- Abcam Adhesion and MethastasisDocument1 pageAbcam Adhesion and MethastasisJosé Jiménez VillegasNo ratings yet
- Resolution For Improving Sip1Document2 pagesResolution For Improving Sip1ARGIE DEJECASION100% (2)
- Leadership Blueprint For SuccessDocument37 pagesLeadership Blueprint For SuccessYusranNo ratings yet
- Caltech - PG Program in Cloud ComputingDocument22 pagesCaltech - PG Program in Cloud ComputingkaperumaNo ratings yet
- LBCDocument14 pagesLBCanililhanNo ratings yet
- Renal Failure Practice QuestionsDocument3 pagesRenal Failure Practice QuestionsJoslyn Gross100% (3)
- Capacitor - Wikipedia, The ...Document17 pagesCapacitor - Wikipedia, The ...srikanthjenaNo ratings yet
- Loans and AdvancesDocument9 pagesLoans and AdvancesidealworldNo ratings yet
- Digital Image and Video Processing Nov 2022Document5 pagesDigital Image and Video Processing Nov 2022khushiduppalaNo ratings yet
- The PalecallersDocument348 pagesThe Palecallersapi-208769579No ratings yet
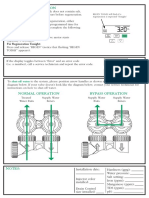
- Manual Regeneration: Shut-Off Water Bypass OperationDocument2 pagesManual Regeneration: Shut-Off Water Bypass OperationcaroNo ratings yet
- Spes Gardening Accomplishment FormDocument2 pagesSpes Gardening Accomplishment FormOliver MendozaNo ratings yet
- Section 1: Try Your Best! Practice Makes Perfect!Document8 pagesSection 1: Try Your Best! Practice Makes Perfect!Hm Ken06No ratings yet
- User Manual RedpackAPI English 1.0Document23 pagesUser Manual RedpackAPI English 1.0GogodzillaNo ratings yet